LUNG FUNCTION TESTS LUNG FUNCTION TESTS Identification of





")



















, DLCO/VA (TLCO/VA) or Krogh")



 Spirometry is")

 the highest forced expiratory flow measured with a peak")







- Slides: 40
LUNG FUNCTION TESTS
LUNG FUNCTION TESTS Identification of disease of the respiratory system Monitoring of treatment Assessment, preventive, research role
METHODS Spirometry Complete lung function test – body pletysmography, diffusing lung capacity testing, arterial blood gas Bronchomotoric tests – bronchodilation, bronchoprovocation Special function tests – e. g. ergometry, polysomnography
LUNG VOLUMES Dynamic /depending on time/ Static
DYNAMIC VOLUMES BR – breath rate MV – minute ventilation MVV – maximal minute ventilation FVC – forced vital capacity FEV 1 – forced expiratory volume in 1. second FEV 1/VC, FEV 1/FVC - ratio FEV 1/VC MMEF 25 -75% - maximum midexpiratory flow between 25 -75% FVC Aex – area under expiratory flow-volume loop 12 -16/min 6 - 10 l 120 -170 l >4 l > 3. 5 l > 70%
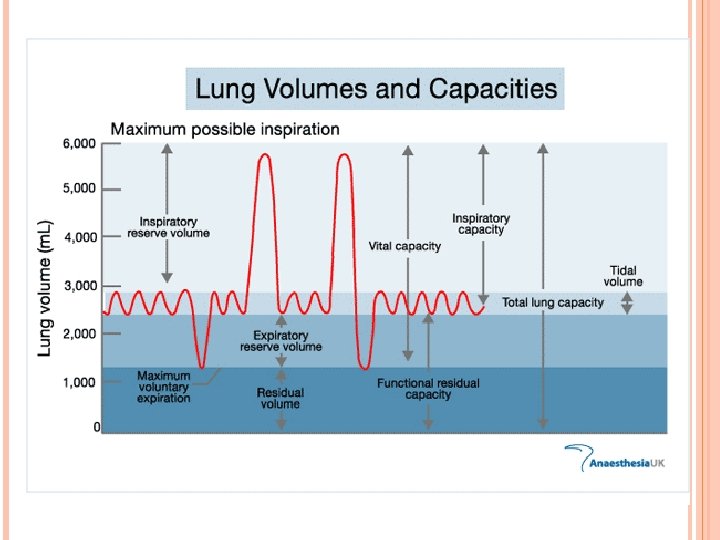
STATIC LUNG VOLUMES TLC – total lung capacity VC – vital capacity (IVC, EVC) VT – tidal volume IRV – inspiratory reserve volume ERV – expiratory reserve volume RV – residual volume – (Helium dilution method, nitrogen washout, body pletysmography) FRC - functional residual capacity (RV+ERV) TGV- thoracic gas volume
VT – tidal volume, 500 ml, the amount of air inspired during normal, relaxed breathing ERV - expiratory reserve volume, 1 200 ml, is the additional air that can be forcibly exhaled after the expiration of a normal tidal volume IRV - inspiratory reserve volume, 3100 ml, is the additional air that can be forcibly inhaled after the inspiration of a normal tidal volume VC - vital capacity, 5000 ml, is the total amount of air that can be expired after maximal inspiration (VT+IRV+ERV), 80% TLC IC - inspiratory capacity, 3600 ml, maximum amount of air that can be inspired after relaxed expiration (VT + IRV) BR – breath rate, number of breaths per 1 minute
SPIROMETRY Open Circuit Spirometer F PR F – Flow transducer PR – Pneumatic resistance - Cooperation of examined person
SPIROMETRY FEV 1 – forced expiratory volume exhaled in 1. second after maximal inspiration
FLOW-VOLUME LOOP FVC – forced vital capacity; maximum expiration after maximum inspiration during a forced breath FEV 1/VC (%) – Tiffeneau ratio PEF – Peak expiratory flow: The highest forced expiratory flow measured with a peak flow meter FEF – forced expiratory flow at the exhaled level of FVC (25%, 50% a 75%) PIF – peak inspiratory flow
Predicted Values Based on: Age Sex Weight Ethnicity Maximal values until the age of 25, then decrease
FLOW-VOLUME LOOP
FLOW VOLUME LOOP IN EXTRA INTRATHORACIC OBSTRUCTION Fixed Obstruction Tracheal stenosis Variable Extrathoracic VCD, Tumor of larynx AND Variable Intrathoracic Tumor of trachea
Spirometry: 1 -acceptable effort, 2 -submaximal effort, 3 - submaximal forced inspiration, 4 - expirium interrupted with cough, 5 - slow start of expirum, 6 - expirium stops prematurely or glottic closure, 7 -submaximal inspiration, 8 - tongue occlusion
BODY PLETYSMOGRAPHY Airtight chamber Boyle – Mariott law – the relationship between the pressure and volume of a gas at a constant temperature p 1. V 1 = p 2. V 2 Pressure changes in chamber caused by thorax movement Assessment of indirectly measured volumes
BODY PLETYSMOGRAPHY FRC - functional residual capacity; the volume in the lungs at the end-expiratory position during quiet, relaxed breathing, ERV + RV RV - residual volume; the volume of air remaining in the lungs after a maximal exhalation TLC - total lung capacity; the volume in the lungs at maximal inflation, the sum of VC and RV (VC+RV nebo FRC+IC) Raw – airway resistance
TYPES OF VENTILATORY DISEASE Obstructive lung disease Restrictive lung disease Mixed lung disease
OBSTRUCTIVE LUNG DISEASE /GOLD, ATS/ERS 2004/ FEV 1/VC < 0. 70 Post-Bronchodilator FEV 1 Mild FEV 1 > 80 % predicted Moderate FEV 1 50 - 79 % predicted Severe FEV 1 30 - 49 % predicted Very Severe FEV 1 < 30 % predicted
OBSTRUCTIVE LUNG DISEASE /ATS/ERS 2005/ FEV 1/VC < lower limit of normal value Mild FEV 1 > 70 % predicted Moderate FEV 1 60 - 69 % predicted Moderately severe FEV 1 50 - 59 % predicted Severe FEV 1 35 - 49 % predicted Very severe FEV 1 < 35 % predicted
OBSTRUCTIVE LUNG DISEASE Asthma, COPD, cystic fibrosis, bronchiectasis Tumor airway obstruction, compression of airways Foreign body
RESTRICTIVE LUNG DISEASE FEV 1/VC > 75% VC, TLC Mild VC 65 – 80 % predicted Moderate 50 – 65 % predicted Severe < 50 % predicted
RESTRICTIVE LUNG DISEASE /ATS/ERS 2005/ FEV 1/VC ˃ lower limit of normal value Decreased TLC Mild FEV 1 > 70 % predicted Moderate FEV 1 60 - 69 % predicted Moderately severe FEV 1 50 - 59 % predicted Severe FEV 1 35 - 49 % predicted Very severe FEV 1 < 35 % predicted
RESTRICTIVE LUNG DISEASE Lung diseases with reduction of lung parenchyma and pleural diseases – interstitial lung diseases (lung fibrosis), lung edema, pneumonia, tumor, atelectasis, lung resection, pneumothorax, pleural effusion Thoracic wall diseases - neuromuscular diseases, kyfoscoliosis Extrathoracic causes – extreme obesity, pregnancy, pain
DIFFUSING LUNG CAPACITY /DLCO/ Diffusing capacity measures the transfer of gas from the alveolar space into the capillary blood stream Transfer factor /TLCO/, assessment of alveolarcapillary barrier (ATS 1981) % Mild 80 -60 Moderate 60 -40 Severe < 40
Procedure: the person inhales rapidly and completely, reaching the total lung capacity a test gas mixture of carbon monoxide (0. 3%) and helium (doesn´t cross the alveolar-capillary membrane), and holds the breath for about 10 seconds, then the subject exhales. DLCO are calculated from consumption of CO, RV and TLC is calculated from dilution of Helium, also Krogh factor (DLCO/VA) is calculated.
DIFFUSING LUNG CAPACITY /DLCO/ Transfer Coefficient- coefficient of diffusion (KCO), DLCO/VA (TLCO/VA) or Krogh factor, negatively correlates with pulmonary volume Decreased DLCO: interstitial lung disease, emphysema, lung resection, pulmonary embolus, anaemia
HYPERINFLATION RV or FRC Mild 125 -175 predicted Moderate 176 -250 predicted Severe ˃ 250 predicted
CHANGES OF STATIC VOLUMES
Asthma COPD FEV 1 Kyphos Obesity NMD coliosis Chronic PE´s ↓↓ ↓ ↓ NL NL/↓ ↓ ↓ NL FEV 1/F VC ↓ ↓ NL/↑ NL NL RV ↑ ↑ ↓ ↓ NL TLC ↑ ↑ ↓ ↓ NL DLCO NL/↑ ↓ ↓ ↓ DLCO/T LC NL ↓ ↓ NL NL ↓ FVC ↓ ILD ERV NIF/ MEF NL NL
BRONCHOMOTORIC TESTS Bronchodilation Test Detection of reversible obstruction (dif. dg. asthma, COPD) Spirometry is recorded before the inhalation 400 ug of Salbutamol and 30 minutes after Reversible Obstruction – FEV 1 > 12% or > 200 ml
BRONCHOMOTORIC TESTS Bronchoprovocation Test Inhalation of increasing concentration of aerosol – metacholin Bronchial hyperresponsiveness (asthma, chronic cough) o Positive – FEV 1 < 20% compared with the value at the beginning of testing
PEAKFLOWMETRY PEF (peak expiratory flow) the highest forced expiratory flow measured with a peak flow meter Disadvantage: less exact than spirometry Advantage: availability at home (exacerbation), work (professional asthma) PEF max –PEF min ½ x PEF max+PEF min ˃ 15 % daily variability
Case 1. An 18 year old girl with cough and wheeze waking her at night. FEV 1 2. 1 66% (3. 2) FVC 4. 2 95% (4. 4) FEV 1/FVC 50% PEF 345 (550) a) Your interpretation? b) Likely diagnosis? c) How would you confirm the diagnosis? a) Airflow obstruction (moderately severe) b) Asthma c) Response to bronchodilator >12% Demonstrating variability of PEF >15% Sputum eosinophils, blood eosinophilia, raised IGE
o o o o o Case 2. A 64 year old male with a 60 pack year history now has 2 years of cough and sputum with increasing breathlessness on exercise. FEV 1 1. 0 36% (2. 8) FVC 3. 6 90% (4. 0) FEV 1/FVC 28% PEF 260 (355) a) Your interpretation? b) Likely diagnosis? c) How would you confirm the diagnosis? a) Airflow obstruction b) COPD c) No response to steroid trial <12% variability in FEV 1, <15% variability in PEF no bronchodilator response
Case 3. A 60 year old male with a 30 year pack history attends with prolonged cough and sputum. You suspect COPD. FEV 1 2. 1 88% (2. 4) FVC 3. 0 83% (3. 6) FEV 1/FVC 75% PEF 340 (380) o o a) Your interpretation? b) Likely diagnosis? a) Within normal limits b) Chronic bronchitis not COPD
CASE 4. A 73 YEAR-OLD MAN, NON-SMOKER, PRESENTS WITH PROGRESSIVE SOB ON EXERTION OVER THE PAST YEAR. HE REPORTS A DRY COUGH, NO WHEEZE, SPUTUM PRODUCTION, FEVER. Actual FEV 1 (l) 1. 28 FVC (l) 1. 57 FEV 1/FVC (%) 82 FRC 1. 73 RV (l) 1. 12 TLC (l) 2. 7 RV/TLC (%) 41 DLCO corr 5. 06 Predicted 3. 39 4. 46 76 3. 8 2. 59 6. 45 42 31. 64 % Predicted 38 35 45 43 42 16
CASE 4. Reduced FEV 1, FVC, TLC, DLCO, a preserved FEV 1/FVC ratio Severe restrictive lung disease The patient was diagnosed with idiopathic pulmonary fibrosis
Case 5. A 25 year-old man, non-smoker presents with dyspnea and wheezing. Two years ago, he was in a major motor vehicle accident. He had a tracheostomy placed because he remained on the ventilator for a total of 7 weeks. Pre-Bronchodilator (BD) Test Actual Predicted FVC (L) 4. 73 4. 35 FEV 1 (L) 2. 56 3. 69 FEV 1/FV 54 85 C (%) % Predicted 109 69
THANK YOU FOR YOUR ATTENTION!