LUNGS PLEURA Dr Shathaly Mustafa Majed MSc Human
. U of K. MSc")











")










- Slides: 35
LUNGS & PLEURA Dr. Shathaly Mustafa Majed. MSc. Human Morphology(Anatomy). U of K. MSc molecular medicine U of K. MSc. Medical education. U of K. MD Surgery. SSMB Diploma in research methodology and biostatistics. UMST
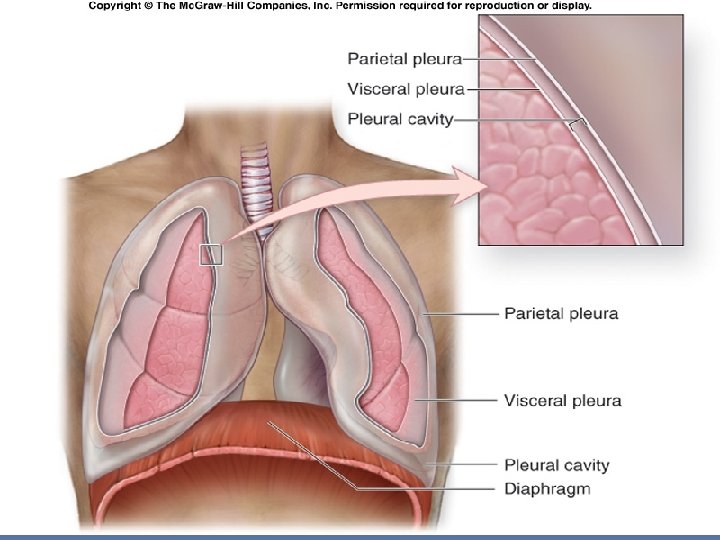
Pleura and Pleural Cavities Pleura is a serous membrane lines the outer surface of each lung and the adjacent internal thoracic wall Two layers separated by cavity: 1. The visceral pleura: tightly covers the outer surface of each lung, and follows the fissures. 2. The parietal pleura: lines the internal thoracic walls, the lateral surfaces of the mediastinum, and the superior surface of the diaphragm.
Pleura and Pleural Cavities The parietal and visceral pleural layers are continuous at the hilum of each lung. The potential space between these serous membrane layers is a pleural cavity. The pleural membranes produce a thin, serous fluid that circulates in the pleural cavity and acts as a lubricant, ensuring minimal friction during breathing.
Pleurae The parietal pleura is supplied by numbers of intercostal and phrenic nerves (somatic spinal nerves). Thus, sensitive to pain. The subdivisions of parietal pleura according to their locations are: a) Costal b) Diaphragmatic c) Mediastinal d) Cervical (cupola). The visceral are innervated by sympathatic (T 4 and T 5). Thus, not sensitive to pain.
At the root of the lungs visceral pleura joins the parietal pleura and encloses all the structures entering and leaving the lungs. There it forms folds called the pulmonary ligaments enclosing potential spaces. Provide dead space for pulmonary vein and allow the roots to descend
Pleural reflections These are the sites where the parietal pleura turns from lining the surface of one structure, such as diaphragm, to another, such as thoracic wall. At these locations the pleura folds and changes direction. The vertebral reflection covers the vertebral bodies, the sternal is located anteriorly and the costal along the costal margins
Recesses These are located at the edges of the pleural cavities where there is normally no lung tissue. 1. The costodiaphragmatic is inferior, between diaphragmatic and costal pleura. Extends from the 8 th and 10 th ribs along the midaxillary line 2. The costomediastinal (sternocostal) is anterior, between the mediastinal and costal pleura.
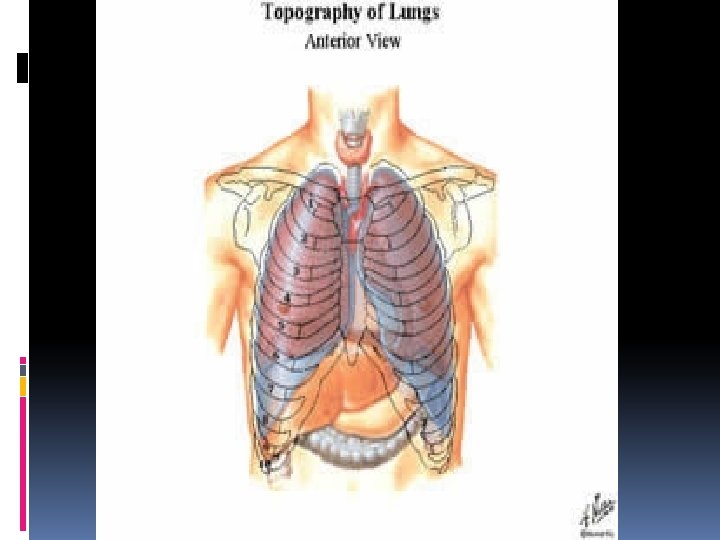
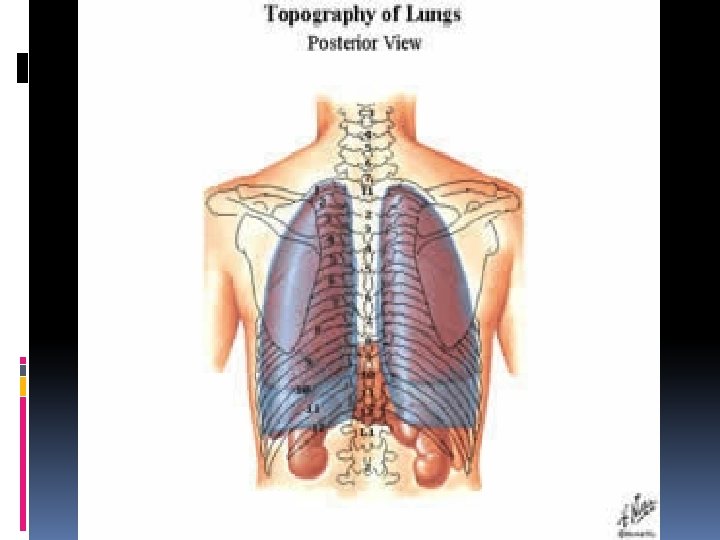
Surface Anatomy v Surface projections of the pleural spaces reflect the differences in size on the left and right. v The reflections run parallel to one another until rib 4 where the left is indented; the right continues to rib 6. Both turn laterally there. The reflections reach rib 8 at the midclavicular line, reach rib 10 in the midaxillary line and the lower border of 12 th vertebra posteriorly.
Endothoracic fascia The endothoracic fascia is connective tissue between ribs and costal pleura. It is thickened superiorly to form the suprapleural membrane
Blood supply and lymphatic driange of pleura Parietal Arteries Veins Visceral Same as thoracic wall Same as lung Intercostal. internal thoracic and musculophrenic Azygos and internal thoracic veins Lymphatics Intercostal, internal thoracic, and diaphragmatic LNs Bronchial arteries Bronchial veins Bronchopulmonary LNs
Clinical Pneumothorax is air in the pleural cavity. Pyothorax is pus in the pleural cavity. Hemothorax is blood in the pleural cavity. Chylothorax is lymphatic fluid in the pleural cavity
Clinical Irritation of the central diaphragmatic and mediastinal pleurae results in referred pain in the shoulder and lower neck. Irritation of the periphery of the diaphragmatic and costal pleurae is referred to the corresponding region of the thoracic wall. Pleuritis, or pleurisy, is an inflammation of the pleurae which may cause friction and result in auscultation of the pleurae during breathing. Normal pleural movements are quiet.
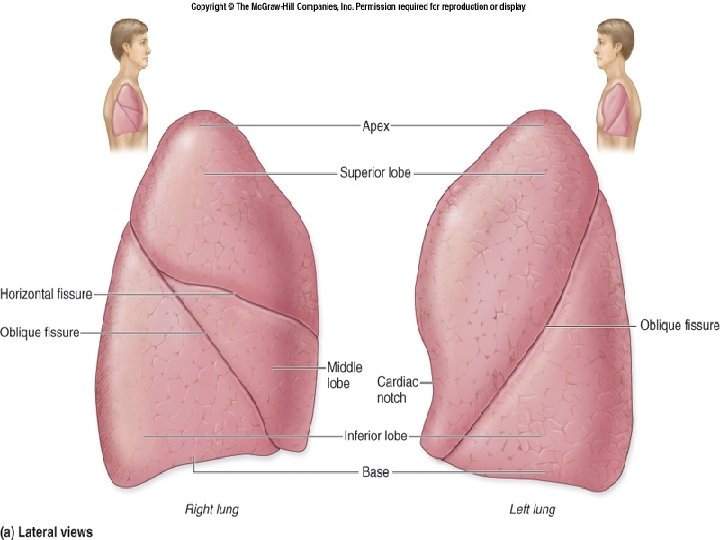
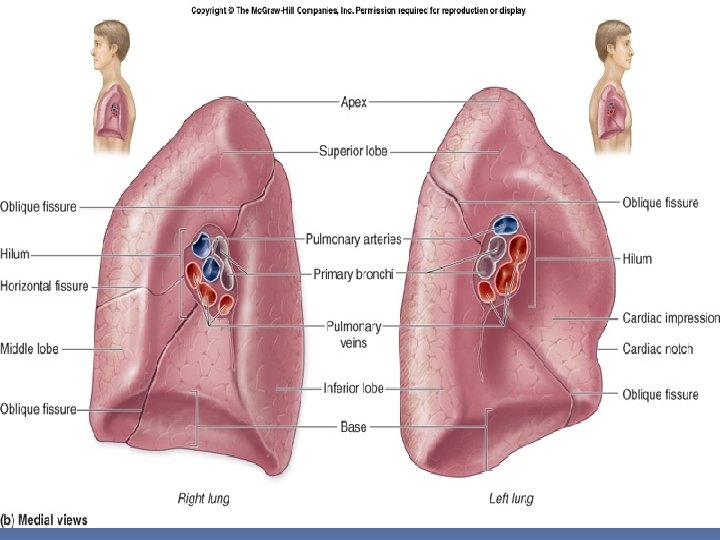
Gross Anatomy of the Lungs Ø It conical in shape. Ø It has 1) Apex at the upper end 2) Base resting on the diaphragm. 3) Three borders: anterior, posterior. 4) Two surfaces: costal and medial (vertebral and mediastinal). Ø Toward the midline, the lungs are separated from each other by the mediastinum.
Differences between right and left lungs Right Left It has 2 fissures (oblique and horizontal) and 3 lobes. It has only one fissure (oblique) and 2 lobes Anterior border is straight Anterior border is interrupted by the cardiac notch and has lingula at the lowest part of the upper lobe Larger and heavier (about 700 mg) Smaller and lighter (about 600 mg) Shorter and broader Longer and narrower
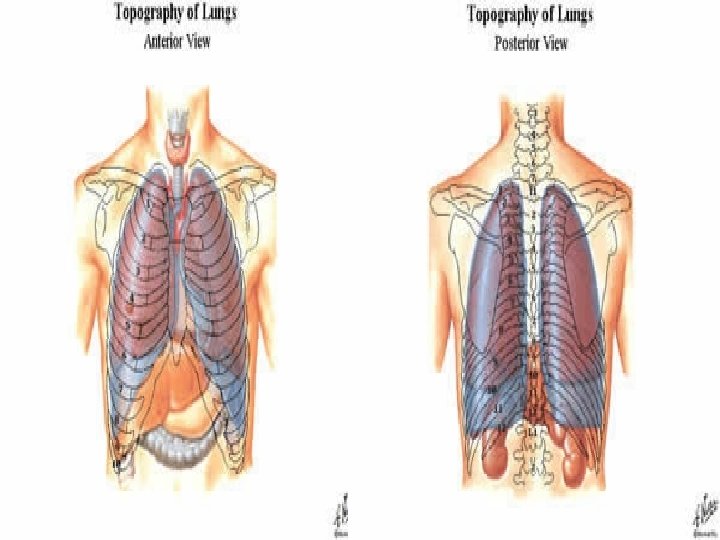
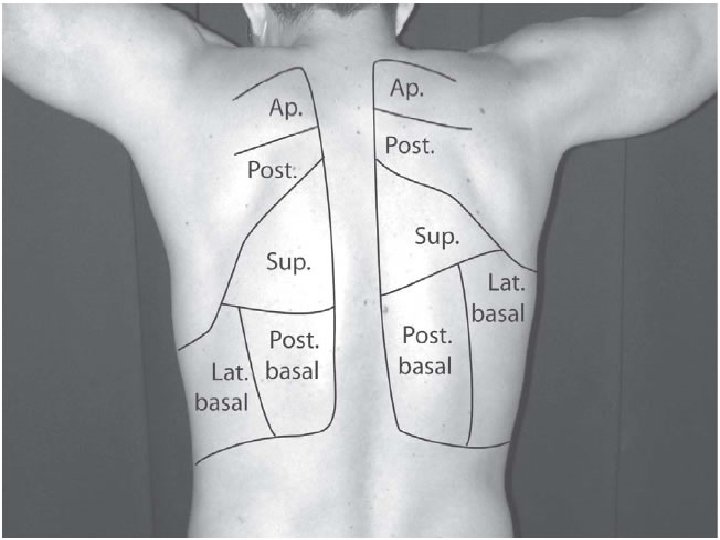
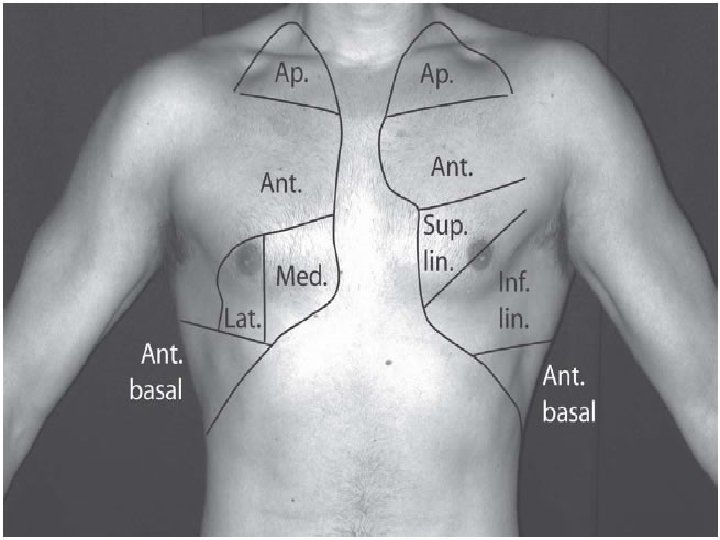
Surface projections In general, most of the lower lobe projects posteriorly, and the upper, and middle in the case of the right, project anteriorly The apex of each lung projects 1 inch above the medial 1/3 of the clavicle The oblique fissures project anteriorly at the sixth rib and costal cartilage, and the horizontal fissure follows the 4 th on the right side The lower borders of the lungs follow costal cartilage 6 on the anterior side, cross rib 6 at the mid-clavicular line and are found at vertebral body 10 on the posterior side.
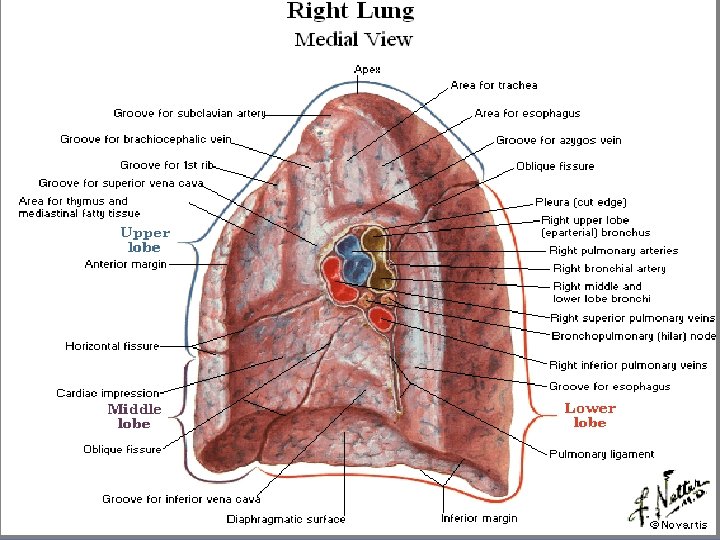
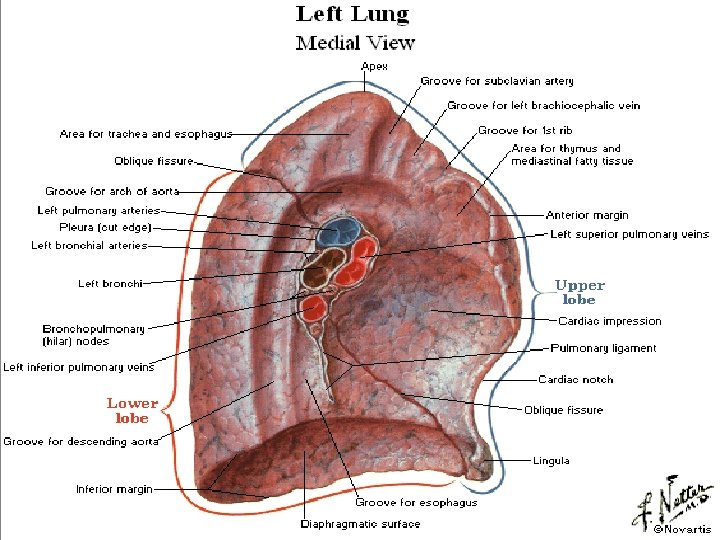
Roots of the lung and their relations Is formed by structures which either enter or come out of the lung hilum. Each lung root is bounded by pleura. Roots of the lungs lies opposite to bodies of T 4, T 5, and T 6. The roots are surrounded by the pleura which form pulmonary ligaments on the inferior portions of the roots. The heart, pericardium, phrenic nerves and pericardiophrenic vessels are anterior, and the vagus nerves and the pulmonary plexus are posterior. The azygos vein arches over the right lung root, and the aorta arches over the left.
Root contents 1. principal bronchus on left side, and eparterial and hyparterial bronchi on right side 2. Two pulmonary veins, superior and inferior. 3. One pulmonary artery 4. Bronchial arteries, one on right side and two on the left side. 5. Bronchial veins 6. Bronchopulmonary lymph nodes, 7. Ant and post pulmonary plexus of nerves 8. lymphatics of the lungs 9. Areolar tissue
Relations and impressions on the medial surface of lungs Please see the next 2 slides and observe the relations and impressions on each side
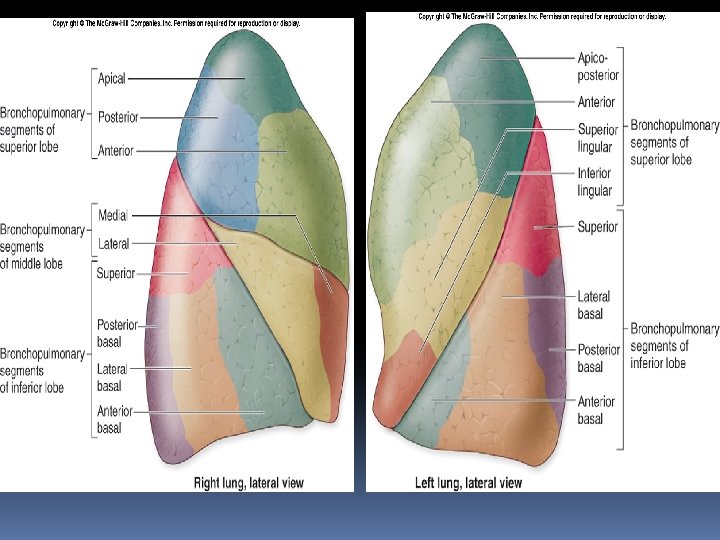
Bronchial tree Primary bronchi enter the hilum of each lung with pulmonary vessels, lymphatic vessels and nerves. Secondary (or lobar) bronchi Branch of primary bronchus left lung: �two lobes + two secondary bronchi right lung �three lobes + three secondary bronchi. Tertiary (or segmental) bronchi Branch of secondary bronchi left lung is supplied by 8 to 10 tertiary bronchi. right lung is supplied by 10 tertiary bronchi supply a part of the lung called a bronchopulmonary segment.
Clinical Correlations The carina is an important landmark on X-rays. It is the most distal point of the respiratory tree capable of the initiation of a cough reflex. It is one of the most sensitive areas in the respiratory tree The right primary bronchus is more directly in line with the trachea and is the most likely place for a foreign body to lodge. The left primary bronchus is closely related to the pulmonary trunk and aorta. Resection of a bronchopulmonary segment along the border of a segment offers the least bloody field. The pulmonary veins and occasionally pulmonary arteries have tributaries and branches which cross segmental boundaries Knowledge of the direction of the tertiary bronchioles and bronchopulmonary segments is important for proper positioning of the patient to encourage drainage of lung segments (postural drainage) or to predict the route of drainage. Blockage of a segment may result in segmental atelectasis or collapse.
Blood supply of lungs Has two distinct blood supplies. The pulmonary arteries carry deoxygenated blood from the pulmonary trunk. They lie anterior to the bronchi, following them closely and branching at the same points. Bronchial arteries: supply pulmonary tissues and the bronchial tree with oxygenated blood. Number variable One on right, arises from 3 rd posterior intercostal artery or upper left bronchial artery Two on left, arises from descending aorta
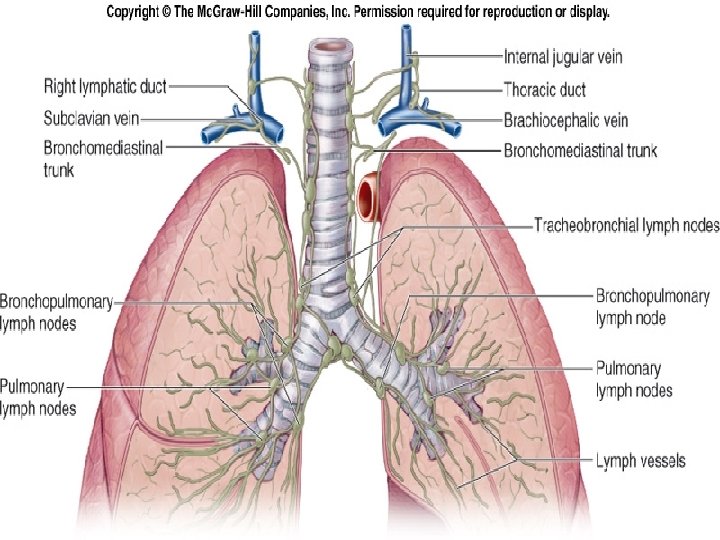
Lymphatic drainage Lymph from the superficial lymphatic plexus flows into the bronchopulmonary nodes at the hilum. Lymph from the deep plexus flows to the pulmonary nodes and the bronchopulmonary nodes. The bronchopulmonary nodes drain into the tracheobronchial nodes, the paratracheal nodes, and finally, the bronchomediastinal trunks Clinical Correlate: Lymphatic flow is important in the lung owing to the incidence of cancer of the lung. Cancer of a bronchus, or bronchogenic carcinoma is common; a typical site of metastasis is the brain. The palpable supraclavicular nodes or `sentinel' nodes are often enlarged in bronchogenic carcinoma.
Nerve supply The nerves supplying the lung come from the pulmonary plexuses. The parasympathetic nerves are from the vagus nerve. The sympathetic nerves are from the cervical and upper thoracic ganglia (origin from. T 2 to T 5). Briefly, the sympathetic nerves actions are: constrict the pulmonary arteries dilate the bronchi inhibit glands secretion The parasympathetics do increase the vascular leak from the lung capillaries constrict the bronchi stimulate secretion mediates the sensory component of coughing and other reflexes.