Limportanza delle interazioni farmacologiche nella gestione dellHIVAIDS delle

 può subire")




 50 0 1 2 3 4 5 6 7 number")



 Change in RPV exposure (AUC) Change in other")



 Antimetabolites: mycophenolate (UGT) Mamalian target-of-rapamycin")

 Amphetamines Metabolism Actual/theoretical interaction Potential significance 2 -3")









 Drug HIV-infected HIV/HCV co-infected* ATV ↓ (Reyataz SPC) ↑")
 * Decreased albumin associated more with cirrhosis and significant")
: Rifabutin 150 mg (half dose) every other day or three")


 1 5. 53 2 6.")



 of Patients Achieving HIV RNA <50 copies/m. L (95% CI) Over Time")
 of Patients with v. RNA <50 copies/m.")




 Spring 2 e Single (Glasgow,")

- Slides: 45
L’importanza delle interazioni farmacologiche nella gestione dell’HIV/AIDS, delle comorbosità e della co-infezione HCV Stefano Bonora Università di Torino 12 Aprile 2013
Premessa § Un farmaco introdotto nell’organismo (per via orale, parenterale, ecc. ) può subire varie trasformazioni, in funzione delle sue caratteristiche fisico-chimiche, ed essere eliminato per vie diverse, in varie forme molecolari. § Può accadere che un farmaco non venga quasi per nulla modificato e sia eliminato come tale, oppure che subisca numerose trasformazioni verso forme che possono essere ancora farmacologicamente attive (o anche più attive rispetto alla molecola originale) oppure del tutto inerti (non attive) per quanto concerne l’effetto desiderato.
Premessa § Le interazioni possono avere differenti meccanismi (non solo inibizione o induzione del metabolismo). § Le interazioni possono alterare la quantità di farmaco disponibile nell’organismo con potenziale impatto su efficacia e tossicità. § L’effetto di un farmaco interagente nel tempo è diverso in funzione del meccanismo di interazione.
OUTLINE • Epidemiology • New antiretrovirals/drugs combination • Sources of information • Interpretation and management of DDIs
OUTLINE • Epidemiology • New antiretrovirals/drugs combination • Sources of information • Interpretation and management of DDIs
Considerations in Management of the Older HIV Patient Earlier appearance of comorbidities supports an earlier ‘older’ age designation in HIV patients, ie 55 vs 65 years!
30 20 patients (%) 50 0 1 2 3 4 5 6 7 number of co-medications Number of co-medications >8 io ca va rdi scova us C lacula an NS Cr d ga ti- a a NSrurugs i ng ag st ro ga a nfeti-inefn gesn in strna ct ectts ts te oinlganiaveive st te e lg s s s e m ina tinsaicssics et ml d l dr an h e r ug h tip or adh othaudgss la a m or n one te ntipa onmoe le lant n ts tel il a es es n e i /a tsp til nt /aind ipi A an C icoticeomdem gi B E ACagagiuc ics ot a e in E u las enngita Bhibinhla nts siote bn l eta it ibintots ca i n sioc bloo r rs lc ns II n I k cks iu cul i I e e m al inins d nhiinhribs rs c iu /aulinu d bi ito ham nt /are iur to rs nnchaidntidticeticrs elnneiabiabs s inl in etetic hihibicss bi ito tors rs A ca rd patients (%) Patients (%) Drug Interactions will be greater as patients age << 50 years 0 B >50 years 60 ? 50 years *** 10 10 < 50 years ? 50 years > 50 years 40 50 40 30 *** 20 *** *** * *** *** 0 Marzolini C et al J Antimicrob Chemother 2011; 66: 2107
Failure to Recognise Drug Interactions • HIV drugs amongst the most therapeutically risky - 20 -40% patients on ARVs at risk of clinically significant interactions • PIs > NNRTIs >> MVC/RAL > NRTIs - PIs associated with 5 -fold prevalence risk of significant DDIs compared to raltegravir, and 10 -fold risk compared to NRTIs • Physicians recognise only around a third correctly - Pharmacist pre-screening of 200 HIV clinic patients told physicians something they did not know about medication history (20%), adherence (31%) or drug interactions (38%), and changed patient management in 13. 6% Patel et al. Ann Pharmacother 2011, Miller et al Pharmacother 2007; 27: 1379, Evans-Jones et al. CID 2010; 50: 1419, de Maat et al. Ann Pharmacother 2002; 36: 410 -15 Mok et al. Am J Health Sys Pharm 2008; 65: 55, Seden et al. Int J STD AIDS 2012 (in press) Seden et al (unpublished)
Quindi § Il rischio di interazione è funzione del numero di farmaci assunti dal paziente. § Tale rischio è probabilmente sottostimato nella pratica clinica. § Alcune classi di farmaci hanno un rischio di interazione significativamente ridotto rispetto ad altre (per es. INI, inibitori dell’integrasi vs. NNRTI o IP).
OUTLINE • Epidemiology • New antiretrovirals/drugs combination • Sources of information • Interpretation and management of DDIs
Drug Interaction Data for RPV (Rilpivirina) Change in RPV exposure (AUC) Change in other drug’s exposure (AUC) TDF 1 « +23% LPV/r 2 +52% (CYP inhibition) « DRV+RTV 3 +130% (CYP inhibition) « Maraviroc « « Raltegravir « « Ketoconazole 4, 5 + 49% (CYP inhibition) - 24% Acetaminophen 6 « « Rifampicin 4 -80% (CYP induction) « Rifabutin 7 -46% (CYP induction) « Ethinylestradiol 8 or norethindrone 8 « « Atorvastatin 9 « « Famotidine 10 « (if separated by 4 hrs) ¯-16% Methadone 11, 12 « «, « Chlorzoxazone 4 « « -40% (p. H increase) « Omeprazole 13 Sildenafil 14 Crauwels H, et al. ACTHIV 2011; Denver. Colorado. #TPOI-4 «
Rilpivirine Drug Interaction: Rationale for Contraindication & Spacing • H 2 antagonists must be taken 12 hours before or 4 hours after RPV since when taken 2 hours before RPV resulted in 85% reduction in RPV exposures • PPIs are contraindicated with RPV due to significant 40% reduction in RPV exposure • Antacids should be given ≥ 2 h before or ≥ 4 h after RPV Parameter Mean % Change (90% CI) Famotidine 40 mg single dose taken 2 hours before rilpivirine Omeprazole 20 mg once daily Cmax AUC 85% ( 88 to 81) 76% ( 80 to 72) 40% ( 52 to 27) 40% ( 52 to 29) RPV/TVD US Prescribing Information, Gilead Sciences, Inc. July 22, 2011 Atripla does NOT have an indication for the treatment of naïve patients and there is NO Atripla promotion concerning treatment NAÏVE patients. For internal Gilead use only Eviplera does NOT have an indication for the treatment of experienced patients and there is NO Eviplera promotion concerning treatment experienced patients and until Italian AIC is granted Do not copy or distribute
Tuberculosis Protease inhibitors NNRTIs Entry / Integrase inhibitors Fonte: http: //www. hiv-druginteractions. org/
ANRS 12 180 Efficacy Outcomes, W 24 Primary endpoint : HIV RNA<50 cp/m. L at W 20 and W 24, m. ITT (M=F, D/C=F) PRIMARY ENDPOINT n EFV RAL 400 RAL 800 N = 51 % [95% CI] n % [95% CI] Success 32 63 [49 -76] 39 76 [65 -88] 40 78 [67 -90] Failure 19 37 [24 -51] 12 24 [12 -35] 11 22 [10 -33] Virologic failure 15 12 4 AE leading to treatment discontinuation 2 0 3 Death 2 0 2 Withdrawal / Lost to Follow-up 0 0 2 Secondary endpoint : HIV RNA<400 cp/m. L at W 20 and W 24, m. ITT (M=F, D/C=F) SECONDARY ENDPOINT Success Failure Virologic failure AE leading to treatment discontinuation Death Withdrawal / Lost to Follow-up EFV RAL 400 RAL 800 N = 51 n % [95% CI] 39 12 8 2 2 0 76 24 [65 -88] [12 -35] 41 10 10 0 80 20 [69 -91] [9 -31] 42 9 2 3 2 2 82 18 [72 -93] [7 -28]
Immunosuppressant agents CNI: cyclosporine, tacrolimus (CYP 3 A, Pgp) Antimetabolites: mycophenolate (UGT) Mamalian target-of-rapamycin (m. TOR) inhibitors: sirolimus, everolimus (CYP 3 A, Pgp) Van Maarseveen EM, et al. AIDS Pat Care & STD 2012
Antineoplastic agents Drug Metabolism Cyclophosphamide 2 B 6 active 3 A 4 toxic Ifosfamide 3 A 4 active 2 B 6, 3 A 4 toxic Docetaxel 3 A 4 Paclitaxel 2 C 8>>3 A 4 Potential significance IDV CPA CL by 1. 5 in 40 patients RTV DOC AUC x 50 -fold in mice Mild interactions with NVP Severe mucositis/neutropenia with SQV/DLV Vinca alkaloids 3 A 4 Neurotoxicity, myelosuppression Severe neutropenia with vinblastine + LPV/r Doxorubicin Daunorubicin AKR No interactions in 40 patients with IDV No interactions in 19 patients with IDV/NFV/SQV Etoposide 3 A 4>>2 E 1, 1 A 2 Irinotecan Carboxylesterases UGT, CYP 3 A 4 Mucositis, myelosuppression, transaminitis Higher incidence of severe mucositis with SQV LPV/r IRI CL by 47% in 7 patients 50% dose-reduction Persistent neutropenia in one patient Edmunds-Ogbuokiri et al. HIV Clinician 2009
Recreational drugs Drug Ecstasy (X, MDMA) Amphetamines Metabolism Actual/theoretical interaction Potential significance 2 -3 fold with RTV or EFV Fatal interactions reported. Hyponatremia, hypertermia, arrhytmias, seizures, rhabdomyolysis 2 D 6 Possible with RTV Hypertension, hypertermia, arrhytmias, seizures Expired breath as CO 2; first-pass metabolism Possible with RTV Life-threatening case with SQV/rtv Bradycardia, respiratory depression, seizures Unknown Possible with RTV Hallucinations, psychosis 2 B 6>2 C 9, 3 A 4 Possible with RTV or EFV Respiratory depression, loss of consciousness, hallucinations hydrolysis, hepatic cholinesterase >>CYP 3 A 4 Possible norcocaine with NVP or EFV Hepatotoxicity 2 D 6>>1 A 2, 2 B 6, 3 A 4 (speed, cristal) GHB (liquid ecstasy) LSD (acid, blotters) Ketamine (special K, Kit-Kat) Cocaine PCP (angel dust) CYP 3 A 4 Possible with RTV Hypertermia, seizures, rhabdomyolysis Erectile disfunction (Sildenafil…. ) CYP 3 A 4 Possible with RTV Hypotension, arrhytmias Amyl nitrite (poppers) glutathione-organic nitrates reductase Hepatotoxicity Hypotension with erectile disfunction agents Antoniou et al. Ann Pharmacother 2002
Summary of Telaprevir – ARV interactions HIV drug Effect on ARV AUC Effect on TVR AUC Can be used? Reference EFV* -7% -18% Yes Van Heeswijk et al. CROI 2011 ETR -6% -16% Yes Kakuda et al. HIV PK 2012 RPV +79% -8% Yes Kakuda et al. HIV PK 2012 ATV/r +17% -20% Yes Van Heeswijk et al. CROI 2011 DRV/r -40% -35% No Van Heeswijk et al. CROI 2011 FPV/r -47% -32% No Van Heeswijk et al. CROI 2011 LPV/r +6% -54% No Van Heeswijk et al. CROI 2011 RAL +31% +7% Yes Van Heeswijk et al. ICAAC 2011 TDF +30% 0% Yes Van Heeswijk et al. ICAAC 2008 *TVR dose 1125 mg q 8 h
Summary of Boceprevir – ARV interactions HIV drug Effect on ARV AUC Effect on BOC AUC Can be used? Reference TDF +5% +8% Yes Kassera et al. CROI 2011 EFV +20% -19% No Kassera et al. CROI 2011 ETR -23% +10% Yes Hammond et al. JAIDS 2013 ? ATV/r -35% -5% No Hulskotte et al. CID 2012 ? LPV/r -34% No Hulskotte et al. CID 2012 ? DRV/r -44% -32% No Hulskotte et al. CID 2012 RAL +1% +7%* Yes De Kanter et al. CID 2012 ? * vs. historical controls
Epatite C e HIV: cenni § Per una persona sieropositiva, che deve assumere una terapia per tutta la vita, prendersi cura del proprio fegato è una priorità. § Il fegato è il principale organo deputato al metabolismo e alla detossificazione dai farmaci e, quindi, soggetto a danno da parte delle sostanze chimiche e farmacologiche da cui ci depura. § Oggi esistono terapie che aumentano in modo sostanziale la possibilità di un successo terapeutico per la cura dell’epatite. § Affiancare queste nuove terapie a combinazioni farmacologiche anti. HIV con scarse interazioni aumenta la probabilità dell’esito positivo di questo percorso, come ci dicono gli studi clinici sui farmaci anti. HIV di nuove classi (es. : INI).
OUTLINE • Epidemiology • New antiretrovirals/drugs combination • Sources of information • Manegement of DDIs
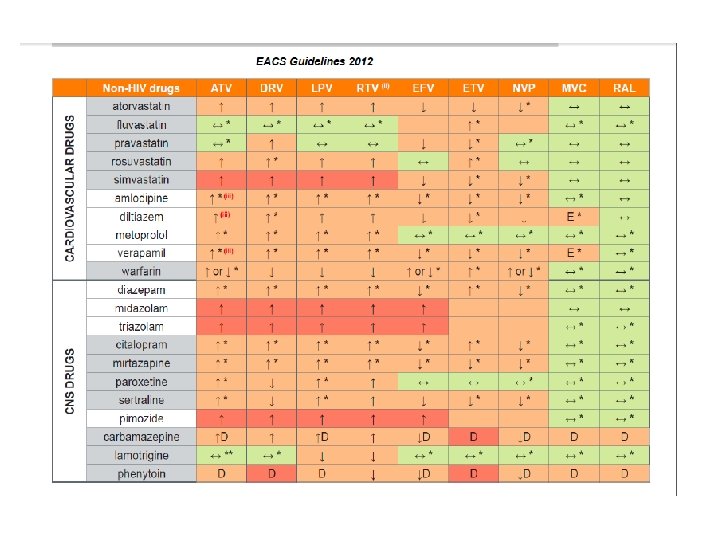
Statins and HAART: management of drug-drug interactions Nachega JB et al AIDS 2012
Cardiovascular drugs and HAART: scarce data • Digoxin serum concentrations were increased by 86% with RTV coadministration due to inhibition of P- glycoprotein (NO DATA IN HIV+) • Many antiarrhythmic medications are CYP 450 3 A 4 substrates. The use of amiodarone, bepridil, flecainide, propafenone and quinidine are contraindicated with PI/r due to the potential risk of exacerbating cardiac arrhythmias (NO CLINICAL DATA).
Corticosteroids • Case report of Cushing’s syndrome and adrenal suppression in a patient on ATV/r and dexamethasone 0. 1% eye drops 1 • Cushing’s syndrome reported with the use of intra articular triamcinolone injections in patients on boosted PIs 2– 4 • Several cases of Cushing’s syndrome with inhaled fluticasone and ritonavir 7 CHECK EVERY KIND OF MEDICATION Check every route of administration 1. Molloy A, et al. AIDS. 2011; 25: 1337– 9. 2. Dort K, et al. AIDS Res Ther. 2009; 6: 10. 3. Danaher PJ, et al. Orthopedics 2009; 32: 450. 4. Ramanathan R, et al. Clin Infect Dis. 2008; 47: e 97– 9. 5. Gray D, et al. S Afr Med J. 2010; 100: 296– 7. 6. Frankel JK, & Packer CD. Ann Pharmacother. 2011; 45: 823– 4. 7. Foisy MM, et al. HIV Medicine 2008; 9: 389– 96.
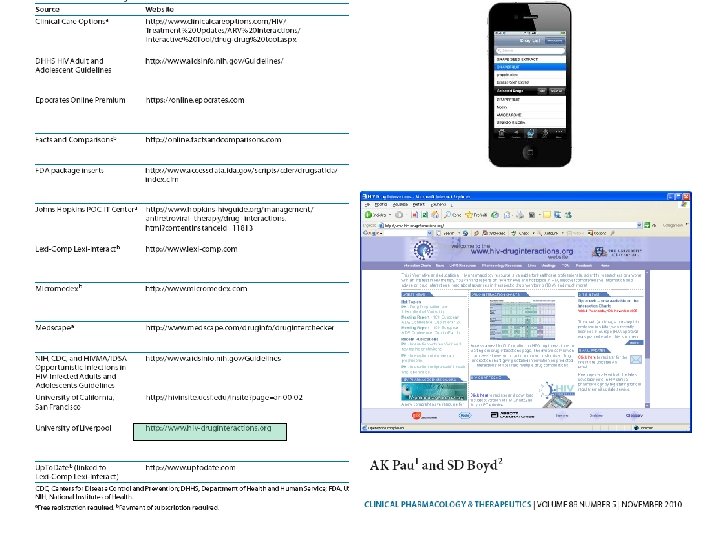
§ Le interazioni farmacologiche esistono e bisogna conviverci. § Il numero di possibili interazioni è altissimo, pertanto non è prevedibile avere dati certi di farmacocinetica per tutte le possibili interazioni. § http: //www. hiv-druginteractions. org è importante per il clinico ma non è RISOLUTIVO.
OUTLINE • Epidemiology • New antiretrovirals/drugs combination • Sources of information • Interpretation and management of DDIs • HIV+ vs Healthy volunteers • Interindividual variability • Clinical significance • New mechanisms?
PK differences (versus healthy volunteers) Drug HIV-infected HIV/HCV co-infected* ATV ↓ (Reyataz SPC) ↑ (Regazzi et al. Ther Drug Monit 2011) ATV/r ↓ (Reyataz SPC) ↔ (Di Biagio et al. J Infect Chemother 2012) ↔ (Regazzi et al. Ther Drug Monit 2011) DRV/r ↑ (Prezista SPC) ↔† (Sekar et al. Clin Pharmacokinet 2010) ↑ RTV † (Sekar et al. Clin Pharmacokinet 2010) ↔ (Sekar et al. 11 th EACS 2011) ↔ cirrhosis vs. historical controls (Curran et al. 13 th WCPHT 2012) LPV/r ↔ (Kaletra SPC) ↔ (Barreiro et al. J Infect Dis 2007) ↑ (Peng et al. J Clin Pharmacol 2006) ↑ RTV (Peng et al. J Clin Pharmacol 2006) ↔ (Canta et al. JAC 2005) ↔ but ↑ V/F (Molto et al. Clin Pharmacokinet 2007) ↑ RTV, ↓ CL/F V/F (Molto et al. Clin Pharmacokinet 2007) ↔ (Seminari et al. JAC 2005) ↓ (Dominguez et al. JAC 2010) EFV ↓ (Mukonzo et al. Clin Pharmcokinet 2011) (Ugandan study) ↓ (Dupont review report 1998) (↔ Caucasian; ↓ Black) ↔ (Katsounas et al. Eur J Med Res 2007) ↔ (Pereira et al. BJCP 2008) ↑ cirrhosis versus no cirrhosis (Barreiro et al. J Infect Dis 2007) ↑ (Dominguez et al. JAC 2010) RAL ↓ (Arab-Alameddine et al. AAC 2012 ) ↔ (composite analysis, Merck) ↑ cirrhosis versus no cirrhosis (Hemandez-Novoa et al. 19 th CROI 2012) ↔ Ұ (Iwamoto et al. AAC 2009) *Compared ҰHealthy to HIV mono-infected; †Healthy individuals with & without mild/moderate hepatic impairment individuals with and without moderate hepatic impairment
Physiological changes (versus healthy volunteers) * Decreased albumin associated more with cirrhosis and significant liver damage lower than HIV or HCV mono-infected patients † Significantly 1 Mehta SH, et al. AIDS Res Human Retrovir 2006; 22: 14– 21; 2 Graham SM, et al. AIDS Res Human Retrovir 2007; 23: 1197– 1200 3 Nagao Y & Sata M. Virology Journal 2010; 7: 375; 4 Monga HK, et al. Clin Infect Dis 2001; 33: 240– 7 5 ; Boffito M, et al. Drug Metab Dispos 2002; 30: 859– 60; 6 Ozeki T, et al. Br J Exp Path 1988; 69: 589– 95 7 Welage LS, et al. Clin Infect Dis 1995; 21: 1431– 38; 8 Nam YJ, et al. Korean J Hepatol 2004; 10: 216– 22
DHHS Guidelines (2002 -2008): Rifabutin 150 mg (half dose) every other day or three times a week is recommended
ü 10 patients with HIV infection and active tuberculosis üLopinavir-ritonavir at, twice daily + rifabutin at 150 mg thrice weekly: 9 of 10 had low rifabutin Cmax values üvalues for the area under the plasma concentration–time curve of rifabutinwere as low or lower than those associated with treatment failure or relapse and with acquired rifamycin resistance üOne of the 10 patients experienced relapse with acquired rifamycin resistance.
Concentration One concentration does not fit all patients!! Time % Inhibiition IC 50
Pravastatin and DRV/RTV Patient Pravastatin AUC Ratio (+DRV: -DRV) 1 5. 53 2 6. 78 3 4. 69 4 3. 80 5 1. 0 6 0. 85 7 0. 57 8 1. 16 9 2. 16 10 1. 31 11 2. 43 12 0. 92 13 1. 16 14 1. 49 Mean, CI Mean, 1. 81; 90% CI, 1. 23, 2. 66 Range Sekar VJ, et al. Pharmacology Workshop. 2007. Abstract 55. 0. 57, 6. 78
Statistical vs. Clinical Significance • A statistically significant effect may not be clinically relevant • A clinically relevant PK interaction would require a dose modification/warning/contra-indication A consistent 10% decrease in AUC in 10 subjects is statistically significant (p<0. 01), but not clinically relevant. Adapted from D Back
Therapeutic window Narrow therapeutic window Wide therapeutic window Adverse events Therapeutic failure Drug concentration Adverse events Therapeutic failure Adapted from D Back
Ci sono scenari clinici dove il valore aggiunto di QD e STR rispetto a schemi più complessi (BID o QD multipill) può essere controbilanciato da altri fattori? • Farmaci concomitanti (QD o BID)? • Tollerabilità a lungo termine?
Proportion (%) of Patients Achieving HIV RNA <50 copies/m. L (95% CI) Over Time Non-Completer = Failure Approach Percent of Patients with HIV RNA Levels <50 Copies/m. L 100 86 81 75 76 69 67 71% 80 82 79 60 61% 40 20 0 0 12 24 48 72 96 120 144 168 192 216 240 Weeks Number of Contributing Patients Raltegravir 400 mg bid. 281 278 279 280 281 281 277 279 Efavirenz 600 mg q. HS. 282 282 281 282 282 279
Yearly Efficacy Analyses Study Week % (n/N) of Patients with v. RNA <50 copies/m. L Change (cells/mm 3) from BL CD 4 Count RAL (N=281) EFV (N=282) RAL – EFV (95% CI) 48 86. 1 (241/280) 81. 9 (230/281) 4. 2 (-1. 9, 10. 3)* 189 163 26 (4, 47) 96 81. 1 (228/281) 78. 7 (222/282) 2. 4 (-4. 3, 9. 0)* 240 225 15 (-12, 43) 156 75. 4 (212/281) 68. 8 (194/282) 6. 6 (-0. 8, 14. 0)* 331 295 36 (3, 68) 192 76. 2 (214/281) 67. 0 (189/282) 9. 0 (1. 6, 16. 4)*° 361 301 60 (24, 95) 240 71. 0 (198/279) 61. 3 (171/279) 9. 5 (1. 7, 17. 3)*° 374 312 62 (22, 102) * P-value for non-inferiority <0. 001. ° Met criteria for superiority.
Sensitivity Analyses of Virologic Efficacy at Week 240 Different Approaches to Handling Missing Data Response by Treatment Group Treatment Effect Responder/Evaluable† Difference Estimates‡ RAL Group EFV Group Difference (95% CI) 198/279 (71. 0) 171/279 (61. 3) 9. 5 (1. 7, 17. 3) <0. 001 Yes p-Value for Non Superiority -inferiority* Concluded* Prespecified as Primary Analysis Non-Completer=Failure Prespecified as Secondary Analyses Treatment-Related D/C=Failure 198/236 (83. 9) 171/239 (71. 5) 12. 4 (4. 9, 19. 8) <0. 001 Yes Observed Failure 198/222 (89. 2) 171/212 (80. 7) 8. 6 (1. 9, 15. 5) <0. 001 Yes Number of evaluable patients in each treatment group according to the specified approach to handling missing data. The 95% CIs and p-values for treatment differences were calculated using weights proportional to the size of each stratum (screening v. RNA level >50, 000 copies/m. L or ≤ 50, 000 copies/m. L). * RAL would be considered non-inferior to EFV if the lower bound of the 95% CI for the difference in response rates was above -12%, and superior to EFV if the entire 95% CI was >0. Two post-hoc snapshot analyses with windows of +/- 6 weeks or +/- 12 weeks around the Week-240 visit were performed to test the robustness of the prespecified analyses: 1. The 6 -week window resulted in the additional exclusion of 8 patients falling outside of the window (6 came in too early and 2 came in too late) compared to the protocol-specified NC=F analysis which used the nominal visit data and yielded response rates of 66. 2% (186/281) in the RAL group and 59. 6% (168/282) in the EFV group with a ∆ (95% CI) = 6. 6% (-1. 4, 14. 5). All 8 excluded patients were in the RAL group, with 7 having v. RNA levels <50 copies/m. L at their nominal Week-240 visit. 2. Since more patients fell outside the 6 -week window for the Week-240 visit compared to previous time points, an analysis using a +/- 12 weeks window (extending the window to the prior visit at Week 228) was untaken at Week 240 which yielded response rates of 70. 8% (199/281) in the RAL group and 62. 8% (177/282) in the EFV group with a ∆ (95% CI) = 8. 1% (0. 3, 15. 8). † ‡
Subgroup Analyses
Specific Drug-Related Clinical Adverse Experiences Occurring in ≥ 5% of Either Group Gastrointestinal Disorders Diarrhoea Flatulence Nausea General Disorders Fatigue Nervous System Disorders Dizziness Headache Somnolence Psychiatric Disorders Abnormal Dreams Insomnia Nightmare Skin And Subcutaneous Tissue Disorders Rash RAL Group (N = 281) n (%) 57 (20. 3) 14 ( 5. 0) 10 ( 3. 6) 25 ( 8. 9) 28 (10. 0) 12 ( 4. 3) 51 (18. 1) 22 ( 7. 8) 26 ( 9. 3) 3 ( 1. 1) 52 (18. 5) 19 ( 6. 8) 21 ( 7. 5) 8 ( 2. 8) 16 ( 5. 7) 3 ( 1. 1) EFV Group (N = 282) n (%) 81 (28. 7) 27 ( 9. 6) 14 ( 5. 0) 29 (10. 3) 47 (16. 7) 25 ( 8. 9) 140 (49. 6) 99 (35. 1) 40 (14. 2) 21 ( 7. 4) 87 (30. 9) 37 (13. 1) 23 ( 8. 2) 15 ( 5. 3) 63 (22. 3) 23 ( 8. 2)
Patients who tolerated EFV, with less than 50 copies/ml HIV-RNA, were randomized into two groups: the RAL-first group started with RAL (400 mg twice daily) and EFV placebo, and the EFV- first group with EFV (600 mg once daily) and RAL placebo. After 2 weeks, both groups switched to the alternate regimen. Half of patients previously on a stable EFV preferred to switch to RAL, after double-blind exposure to RAL for 2 weeks. Substitution of EFV by RAL significantly impacted on lipid levels, stress, and anxiety scores.
Altri esempi Studio STa. R (Glasgow, Cohen O 425) Spring 2 e Single (Glasgow, Eron P 204) Sailing (Atlanta, Croi 2013, Pozniak 179 LB)
Grazie al contributo di MSD Italia