HKSCCM INTERHOSPITAL GRAND ROUND Doctor I cant see







:")






 • Low dose vasopressor still")






 • DIC: Plt 56/ INR")










 • Recent anal abscess Dx in private • Newly diagnosed DM •")





 • An very obese young gentlemen • Newly diagnosed DM • Presented")







 and hyerosmolar hyperglycaemic syndrome (HHS) •")
















 syndrome • Typically community-acquired • Unrelated to")




- Slides: 82
HKSCCM INTER-HOSPITAL GRAND ROUND Doctor, I can’t see Doctor, I can’t move Thriller Film? Yip Hing Wah Tom(NDH ICM trainee) TMH ICU
Content • Case presentation • Discussion
First case • M/58 • NKDA • Ex-smoker/ non-drinker • Lorry driver • No FH of DM • Unremarkable past health except • Anal abscess with drainage in private hospital 10 days ago
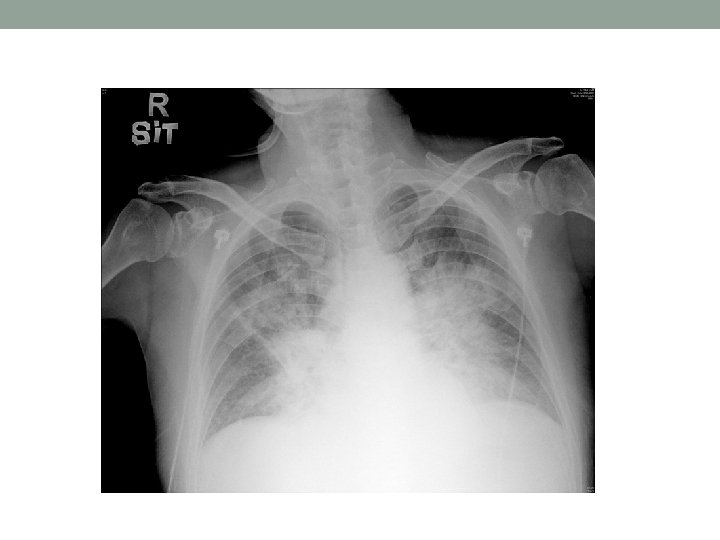
Day 1 • Presentation: • Polyuria and polydipsia for a few days • Chest discomfort and SOB for 2 -3 days • AED: • No fever • H’stix high and urine ketone +ve • ABG: BE -12. 3 • CXR-congested lungs • ECG-sinus tachycardia, no obvious ST/T changes • To ICU for DKA
Upon ICU admission • Afebrile • BP 105/76 • HR 140 • Sa. O 2 100% on 100% NRM • Overweighted • Respiratory distress+ • Alert and obey command • JVP-elevated • Chest-diffuse crepitations • Abdomen-soft, non-tender
• ECG-< 1 mm ST elevation in V 1 -3 with inv T, flatten T in inf leads • (ECG-iphone)
Day 1 • Troponin I: 0. 99 • Bedside echo: • Fair LV systolic function • LVEF(by simpson): 35 -40% • Hypokinesia over inferior, posterior and septal area
Day 1 • Intubated • Cautious rehydration • Insulin infusion • Antibiotics(WCC 27. 9): • Augmentin 1. 2 g Q 8 H • Azithromycin 500 mg Q 24 H • Aspirin and LMWH for ACS • Noradrenaline(NA) for shock
Day 1 • Initial improvement with NA weaning off • Deteriorated again with rising NA requirement • Bedside USG: • Rt lung hepatization and air bronchogram • Small amount of pleural effusion • No fluid in hepatorenal recess • But ? Thickened splenorenal recess • Both kidney normal in size, no stone, no hydronephrosis, normal corticomedullary differentiation
Day 2 • Cr climbing to 195 • Auric • CVVH started
CT abdomen
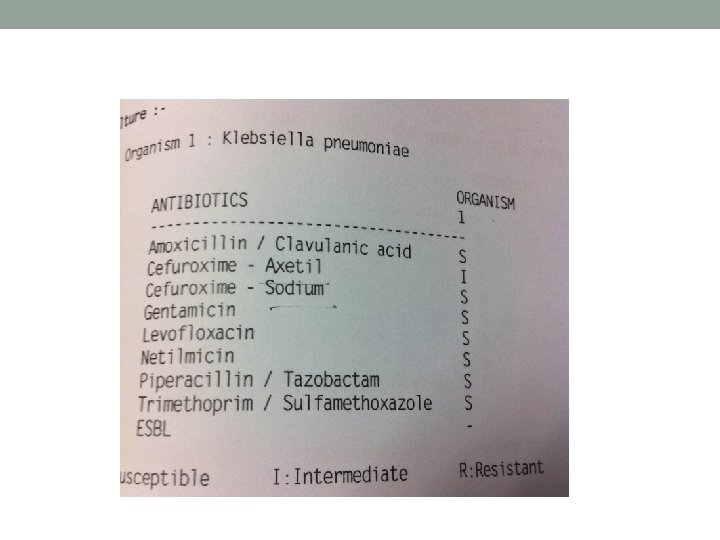
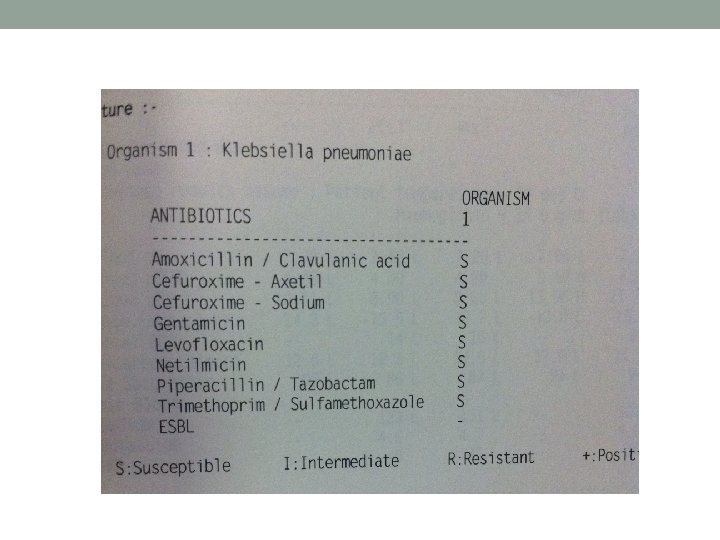
Day 2 • CT abdomen+ pelvis with contrast: • Left pyelonephritis or infarted kidney with left renal vein thrombosis • Blood culture: GNB • Anal abscess culture from private hospital: Klebsiella pnuemoniae, S strain
Day 2 • Stat dose amikacin 750 mg given • Antibiotics upgraded to tazocin • Consulted urologists • EOT done: • L renal and peri-nephric absess with renal vein thrombosis and perirenal infarct • Left nephrectomy done
Progress • Persistent shock • DIC with persistent oozing from drains • Inotropic support • Repeated blood transfusion • Renal support with CVVH • Blood/urine culture: Klebsiella (sensitive strain) • Gradual improvement • Antibiotics downgraded to zinacef as suggested by ID team
Day 9 • Clinically static • WCC still high(>20) • Low dose vasopressor still needed • CT abdomen: • Large collection in left retroperitoneal space • USG guided perinephric abscess drainage • Bloody aspirate yeilded • Culture: no growth
Progress • Further improvement • Extubated on day 12 • Dischargednto general ward on day 14 • In ward • BP/P stable • Refinement in glucose control • Physiotherapy • Planned discharge…
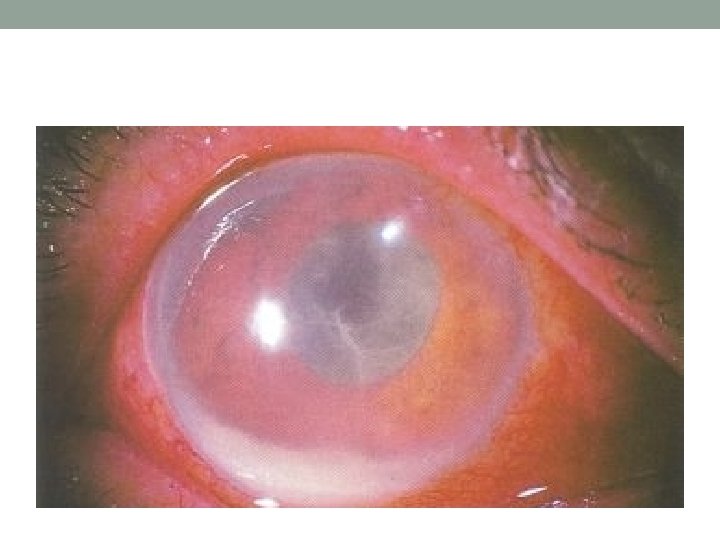
Day 20 • The fact: • Patient c/o left eye “near blindness” • Left eye no response to light
What has happened?
Second case • KTL • M/30 • Non-drinker non-smoker • Programmer • Gout , just take OTC meds for several years • FH: mother diagnosed T 2 DM at 50 years old
Day 1 • Presentation: • Malaise and decreased appetite for 1 -2 weeks • Subjective weight loss • Abdominal discomfort for 1 week • Watery diarrhea and vomiting of yellowish fluid • AED: • Fever 38. 2 °C • Mixed Metabolic and respiratory acidosis: • p. H 7. 15/ CO 2 4. 4/ HCO 3 11. 5 • Spot sugar: 54 mmol/L • To ICU for DKA
Upon ICU admission • Temp 38. 5 °C • BP 112/90, HR 130 • Sa. O 2 98%(2 L O 2) • RR 20 • BMI 35 • Obey command • Dehydrated+ • Chest clear • No cardiac murmur • Abdomen soft, non-tender
Day 1 • High WCC 22. 7 (neutrophil 86%) • DIC: Plt 56/ INR 1. 6 • AKI: Cr 172/Ur 17. 8 • LFT mildly deranged: Bili 23 /ALP 239/ ALT 38 • Amylase 14
Progress • Rehydration • Actrapid infusion • Zinacef
Day 2 • Despite treatment, no improvement • Persistent fever and tachypnea • Development of septic shock • Become unresponsive • GCS E 2 V 1 M 1 • Progressive drop in BP down to 50/20 • Intubated • Noradrenaline started
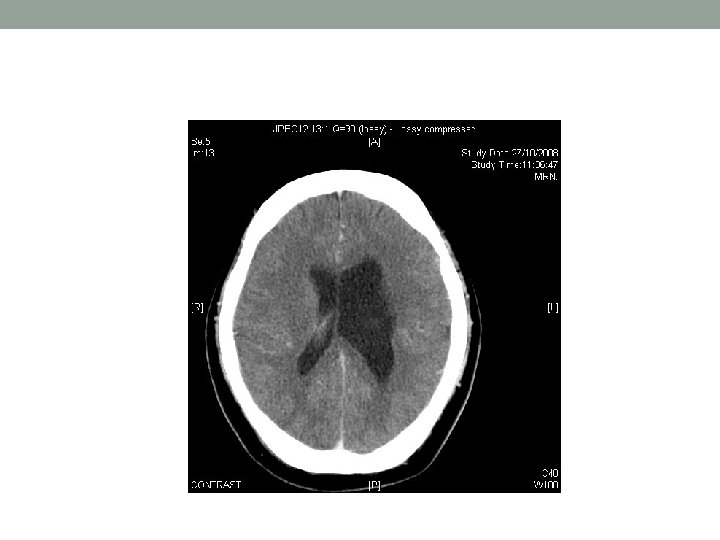
Day 2 • Review: • Neck soft • Plantar equivocal • Echo: • No effusion, LVEF OK, no obvious vegetation • CT brain: • no ICH • Focal dilatation of left lateral ventricle, ? porencephalic cyst due to previous insult in early infancy • LP: unremarkable
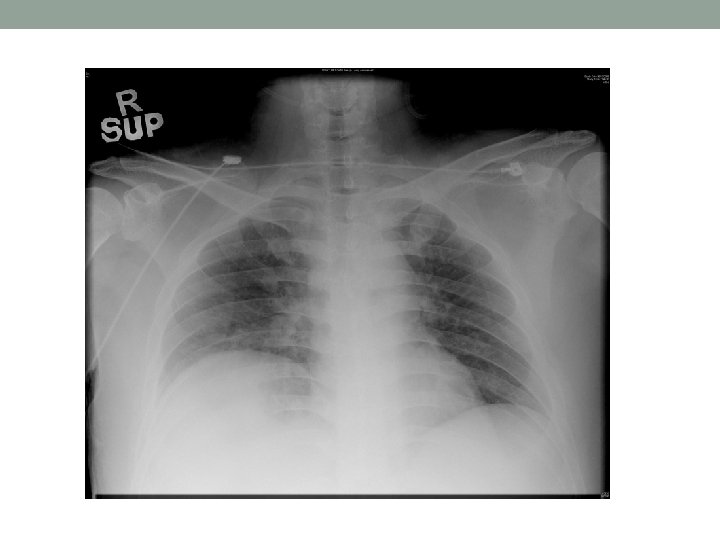
Day 2 • CXR: Rt middle zone consolidation • Antibiotics: • To rocephin and stat dose amikan(750 mg) right after deterioration • Added azithromycin after obvious consolidation shown • Tazocin after blood C/ST: GNB
Day 3 • Clinically static • Awake and obey command • Move all 4 limbs but weak • CT abdomen/pelvis with contrast booked ? liver abscess
CT abdomen
Day 4 • CT Abdomen: • Liver abscess and lumbar septic spondylitis • USG guided drainage of liver abscess done
Day 6 • Alert • Power 0/5 • Tone flaccid • Ankle reflex ++ • Knee reflex – • bicep/tricep reflex – • No pinprick sensation up to umbilicus level
What has happened?
Case 1(continued) • Recent anal abscess Dx in private • Newly diagnosed DM • Presented with DKA complicated with ACS/ AKI/ septic shock • S strain Klebsiella pneumoniae bacteraemia • Found infected and infarted L kidney with nephrectomy done • Residual retroperitoneal collection also drained • Found blindness on day 20
Progress of Case 1 • Ophthalmologist • VA: RE 6/9 ; LE no light perception • Slit lamp • RE: AC cell ++, ant. Vitreous cell ++ • LE: AC cell ++++, keratic precipitates +++ • Fundus • RE: mod proliferative DMR, patch of retinitis over inferior retina • LE: no fundal view, USG: total retinal detachment • Dx: L>>R endogenous endophthalmitis
Progress of Case 1 • Plan • LE: no visual prognosis, for injection and enucleation if needed • RE: continue antibiotics, if VA deteriorate, tapping and intravatreal antibiotics
Day 27 • Eye review • VA same, plan vitreous tapping and intravitreal antibiotics 2 days later
Day 29 • OT • RE post vitrectomy+ vitreous tapping+ intravitreal vancomycin and fortum • LE intravitreal vanco and fortum • Postop • Both eyes have no light perception • Vitreous humor grew Klebsiella pneumoniae • Another eye OT done 1 week later • Discharged with total blindness
Progress of Case 1 • Urologic • Repeated CT show retroperitoneal collection decreasing in size • Patient asymptomatic • No further intervention needed
Case 2(continued) • An very obese young gentlemen • Newly diagnosed DM • Presented with DKA precipitated by klebsiella pneumoniae bacteremia/pneumonia/ liver abscess/ lumbar spondylitis • Suddenly found tetraplegic
Progress of Case 2 • MRI • Epidural abscess with main collection at C 2 -4 level • Moderate to severe stenosis • Cord edema extending up into medulla oblongata • Suspicious epidural collection at L 4 -5/S 1 level
MRI spine
MRI spine
Progress of Case 2 • OT Finding • C 2/3 and C 3/4 disc normal • Prevertebral fascia normal • Pus noted in spinal canal behind C 3 body • Dural sac intact • Decompression+C 2 -4 ASF done • Pus grew Klebsiella pneumoniae
Progress of Case 2 • Limited neurologic recovery • Percutaneous tracheostomy done • Finished a course of antibiotics • On discharge to ward • Adduction of R thumb • Some extension of L wrist • On Bi. PAP
Rehab progress of Case 2 • Lumbar septic spondylitis on conservative treatment • Spasticity Ashworth grade II • Neurogenic bladder • Failed intermittent cathetarization, suprapubic cathetaer inserted • Sacral sore healed upon discharge • Weaned off Bi. PAP 9 months later
Rehab progress of Case 2 • Discharged to a hostel after 1 year • Wheelchair bound • Cared by a maid
Discussion • Hyperglycaemic crises • Diabetic ketoacidosis (DKA) and hyerosmolar hyperglycaemic syndrome (HHS) • American Diabetes Association
Hyperglycaemic crises • Most serious acute metabolic complications of DM • With intensive care, mortality in experienced centres was generally <10% • The 2 most common precipitating factors • Inadequate insulin therapy in patients with history of DM • Infection
Mx of Hyperglycaemic crises • Management of hyperglycaemic crises • Fluid and electrolytes replacement • Initiation of insulin therapy
American Diabetes Association 2009
Mx of Hyperglycaemic crises • Apart from fluid, electrolytes, insulin • What else?
Mx of Hyperglycaemic crises 1. High prevalence of infection as triggers of hyperglycaemic crisis (20 -25%) • Direct causal relationship between diabetes and infections were lacking • DM patients were more susceptible to infections • Mechanisms • Impaired immunity against pathogens • Increased adherence to microorganisms • Ulceration and secondary infection due to microangiopathy • Impaired bladder emptying due to neuropathy, predisposing to the development of UTI Geerlings S. E. , & Hoepelman A. I. . Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunol and Medical Microbiology 1999; 26(3– 4): 259− 265 Moutschen M. P. , Scheen A. J. , & Lefebvre P. J. Impaired immune responses in diabetes mellitus: Analysis of the factors and mechanisms involved. Relevance to the increased susceptibility of diabetic patients to specific infections. Diabete Metab. 1992; 18 (3), 187− 201
Mx of Hyperglycaemic crises • DM patients • More difficult in handling infection • Severity of infections increased in the presence of diabetes mellitus • Outcomes were worse if infection left untreated Message 1 A careful search of precipitating factors, especially infection, is mandatory Joshi N, Caputo GM, Weitekamp MR et al. Infections in patients with diabetes mellitus. N Engl J Med. 1999; 341: 1906– 12 Carton JA, Maradona JA, Nuno FJ, Fernandez-Alvarez R, Perez-Gonzales F, Asensi V. Diabetes mellitus and bacteraemia: a comparative study between diabetic and non-diabetic patients. Eur J Med 1992; 1: 281– 7
Mx of Hyperglycaemic crises • Can clinical symptoms predict the presence of infection?
Mx of Hyperglycaemic crises 2. Most clinical symptoms at presentation were not predictive of infection • Abdominal symptoms • May mimic acute abdomen • Correlated with degree of acidosis rather than infection per se Umpierrez G, Freire AX. Abdominal pain in patients with hyperglycemic crises. J Crit Care. 2002; 17: 63 -7 • Neurological symptoms • Due to cellular dehydration or hyperosmolar state • Not indicative of presence of infection • Need to look for other causes of mental dullness and trigger of hyperglycaemic crises e. g. CVA Zara R. Brenner. Management of Hyperglycemic Emergencies. AACN Clinical Issues 2006; 17( 1): 56– 65
Mx of Hyperglycaemic crises • Afebrile state was common in hyperglycaemic crises • Due to the vasodilation and to the low-fuel substrate availability, especially in the elderly Gaglia JL, Wyckoff J, Abrahamson MJ. Acute hyperglycemic crisis in the elderly. Med Clin N Am. 2004; 88: 1063– 1084. Message 2 • Hypothermia carries poorer prognosis in hyperglycaemic crises Clinical symptoms not helpful in diagnosis of infection in DKA • Absence of fever on admission is not reassuring in hyperglycaemic crises Guerin JM, Meyer P, Segresta JM. Hypothermia in diabetic ketoacidosis. Diabetes Care 1987; 10: 801– 2 • Look for possible sites of infection if patient had history of fever before admission
Mx of Hyperglycaemic crises • If clinical symptoms not helpful, are there any lab results pointing to the presence of infection?
Mx of Hyperglycaemic crises 3. Useful lab result predicting presence of infection • Leukocytosis was a common finding in hyperglycaemic crises • Due to haemoconcentration and stress response resulting from elevation of the counterregulatory hormones • Slovis et al • Leucocytosis with cell counts >25000 mm 3 designated infection and required further evaluation • Result could not be reproduced in paediatric group in which leucocytosis merely indicated severity of DKA rather than the presence of infection Slovis CM, Mork VG, Slovis RJ, Bain RP. Diabetic ketoacidosis and infection: leucocyte count and differential as early predictors of serious infection. Am J Emerg Med 1987; 5: 1– 5
Mx of Hyperglycaemic crises • CRP • An acute phase protein • Rise with infection • But low NPV to exclude infection Message 3 High WCC/CRP signify high chance • Pro-calcitonin • Better predictor of infection CRPabsence of them of infection, butthan the • But not readily available cannot exclude it
Mx of Hyperglycaemic crises • Where and what is the infection?
Mx of Hyperglycaemic crises 4. Common site and type of infection • Respiratory and urinary tract infections remained the most common source of infection Message 4 • Common pathogens in these systems, namely Pathogens in Chest/UTI accountspecies for majority Staphylococcal or Streptococcal and of infection. Empirical antibioticsaccounted should cover these organisms Enterobacteraceae, for majority of infections found • Staphylococcus species and Escherichia Coli reported to be the leading causes of infection in diabetes Gupta S. Koirala J. Khardori R. Khardori N. Infections in diabetes mellitus and hyperglycemia. Infectious Disease Clinics of North America. 2007; 21(3): 617 -38 • Guide empirical antibiotics use
Mx of Hyperglycaemic crises • Hyperglycaemic crises= No big deal?
Mx of Hyperglycaemic crises 5. Infection with a seemingly sensitive organism may still carry uncommon but severe complications in the context of CIKPLA syndrome
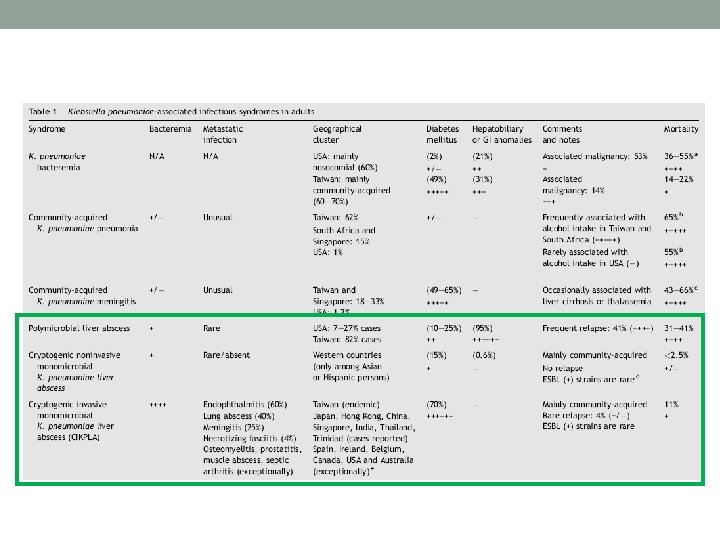
Cryptogenic invasive K. pneumoniae-associated liver abscess (CIKPLA) syndrome • Typically community-acquired • Unrelated to gastrointestinal or hepatobiliary anomalies • Highly associated with distant septic seeding • Distinguished by its geographical distribution • Exclusive to Taiwan (endemic) • A few cases have also been described in China, Korea, Singapore, Japan, India, Thailand, Trinidad, and Jamaica
CIKPLA syndrome • 20 -fold increased association with diabetes mellitus • Frequently complicated by metastatic infections • Endophthalmitis is the most common (as many as 60% of cases) • Lung abscesses (40%), meningitis (25%), and necrotizing fasciitis (4%) • Prostatitis, osteomyelitis, septic arthritis, septic epidural abscesses, and muscle abscesses have occasionally been reported
CIKPLA syndrome • Pathogenesis of CIKPLA • Patient factors • Different socioeconomic background • Genetic makeup • Comorbidity: DM, alcoholism • Bacterial virulence • Capsular polysaccharide serotypes K 1 or K 2, resistance to phagocytosis and intracellular killing • Lack of mannose-α 2/3 -mannose and L-rhamnose-α 2/3 -rhamnose which are sequences that interact with a macrophage lectin • Presence of adhesion molecules e. g. type I and type III fimbriae, CF 29 K • Presence of iron acquisition system
CIKPLA syndrome • Bacterial virulence • Presence of virulence gene mag. A, which encode outer membrane protein ? associated with hypermucoviscosity Message 5 mag. A gene is part of the serotype-specific region of the K 1 capsule gene cluster of mag. A by PCR analysis is an easy, fast and highly specific diagnostic SE Detection Asia+DM+Klebsiella pneumoniae method for identification of the K. pneumoniae K 1 capsule serotype bacteraemia+/-Monomicrobial liver abscess Think of CIKPLA • •
Conclusions • Infection is a common precipitating factor of hyperglycaemic crises • While most pathogens responsible for the infection were sensitive organisms, severe complications can still occur if occult abscesses were not dealt with e. g. CIKPLA syndrome • Symptoms and signs of these complications can be easily missed in an unstable patient in ICU • When patient says “Dr, I can’t see and move”, it is probably too late