PYNEH Presenters Dr Helen Wu Dr HP Shum























 Latency period of 2 to 40 days Ranged from 1")




























")












- Slides: 80
PYNEH Presenters: Dr Helen Wu, Dr HP Shum Chairman: Dr KW Chan ONE TREATMENT, TWO DISEASES
Case 1 Ms Fok, 25 yrs old Good past health Admitted on 27/5/08, found lying unconscious inside a villa in Cheung Chau, burning charcoal was found at the scene; her boyfriend was found dead Transferred by helicopter to PYNEH
E 1 VTM 1, pupils 3+ Sa. O 2 100% on 100% O 2 BP 117/88, sinus tachycardia 168/min Temp 38. 1 C Chest, CVS exam unremarkable No major trauma
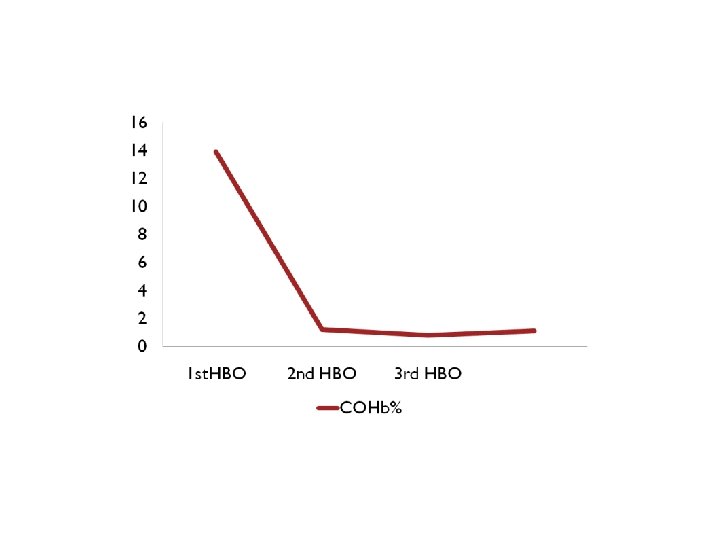
Tn. T 0. 43 ECG: sinus tachycardia with poor R wave progression over V 1 -2 COHb 13. 9% Dx: CO poisoning Hyperbaric chamber contacted for urgent HBO therapy Consult ENT x bilateral myringotomies Post HBO COHb 1. 2%
2 nd and 3 rd session of HBO performed on D 2 and D 3 respectively Extubated on D 3 E 4 V 5 M 6 Transferred to general ward on D 3 Seen by psychiatrist and discharged home on D 16
Case 2 Ms Chan, 34 yrs old, 24 th week gestation Adjustment disorder, hx of suicide in 2007 Found collapse at home, burning charcoal was found at scene E 4 V 1 M 1 BP 93/23, P 70 ECG: SR, no acute ishcaemic change Fetal HR 169/min
COHb 18. 9% Dx: CO poisoning Intubated with RSI Bilateral myringotomies performed by ENT Transferred to Stonecutters Island x HBO on the same day Post HBO COHb 1. 2% E 4 VTM 6 and extubated on D 2 Sessions of HBO performed on D 2 and D 3 Transfer to general ward on D 3 Discharged home on D 6
Case 3 M/40, Ah Sing Mainland professional diver Dived at 20 m depth, no scuba, worked for 1 hr and then saw ghost and quickly ascended to sea surface SOB, multiple joint pain, abdominal pain, transient LOC x 20 -25 min No drug/alcohol intake
GCS 15/15 BP 166/85, SR 105/min Sa. O 2 100% on 100% O 2, RR 20/min Chest: slightly AE over L side Abdomen: diffuse guarding RUL power 1/5, other limbs power 5/5
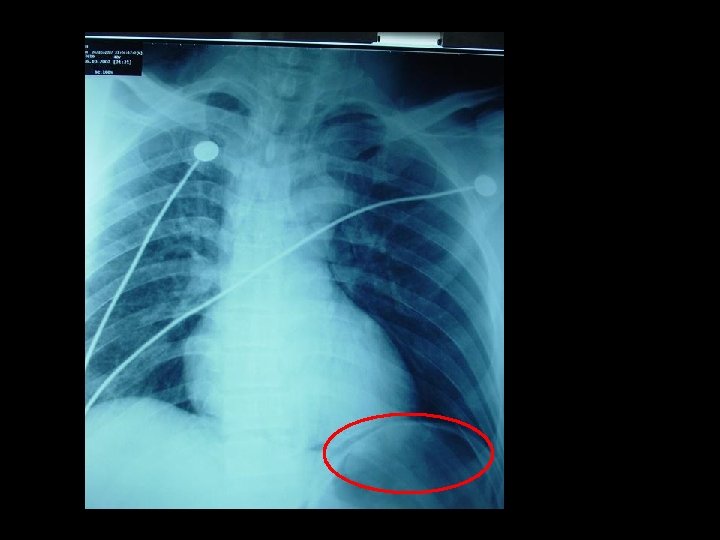
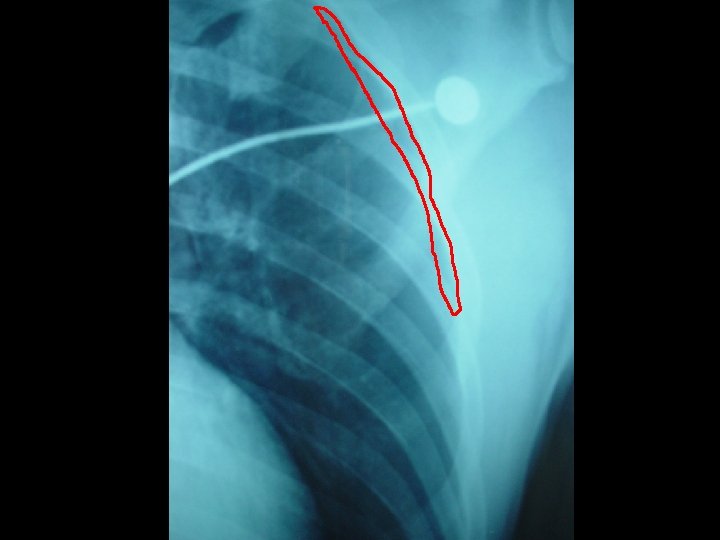
Dx: decompression sickness bilateral chest drain inserted Bilateral myringotomies performed 1 st session of recompression Urgent contrast swallow: no definite leakage in thoracic region
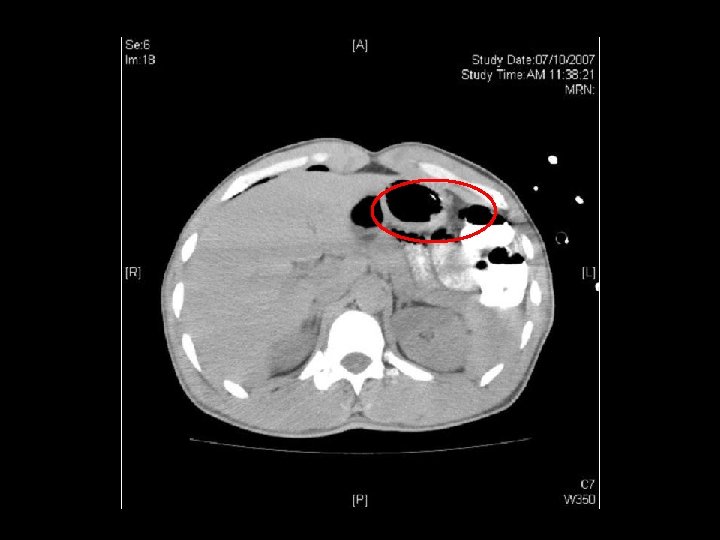
2 nd, 3 rd and 4 th session recompression on D 2, D 3 and D 4 respectively Persistent RUL monoparesis CT brain: hypodensity over L frontaloccipital lobe ? recent infarct MRI brain: acute infarct over L frontoparietal region Dx: deompression illness with pneumothorax, pneumoperitoneum and cerebral air embolism
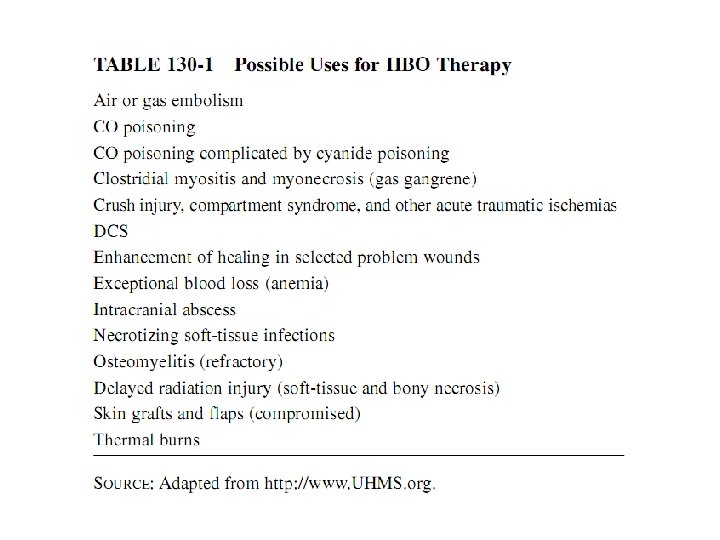
USE OF HYPERBARIC OXYGEN
Physiological basic of HBO Based on gas laws ◦ Henry’s law ◦ Dalton’s law ◦ Boyle’s law Pascal’s principle
Henry’s law At constant temperature, the amount of gas that will dissolve in a liquid is proportional to the partial pressure of that gas over the liquid ◦ 1 ATA = x litres of gas in solution ◦ 10 ATA = 10 x liters of gas in solution Drive more oxygen dissolve in plasma and increase oxygen delivery to tissue even when Hb oxygen carrying capacity is impaired
Dalton’s law The total pressure exerted by a mixture of gases is the sum of the partial pressures that would be exerted by each of the gases if it alone occupied the total volume Flooding the body with one gas tends to “wash out” the others
Boyle’s law At constant temperature, the absolute pressure and the volume of gas are inversely proportional In decompression sickness, nitrogen initially dissolved within the blood may come out of solution and causing gas embolism
Pascal’s principle A pressure applied to a liquid will be transmitted “equally” throughout the liquid
Physiological effect of HBO Increased O 2 delivery ◦ O 2/ antioxidant balance disturbed by increased PO 2 ◦ Oxygen toxicity CNS: seizure, vertigo, hallucination Pulmonary: burning on inspiration, SOB, coughing Pressure difference between body compartments ◦ Barotrauma affecting middle ear / sinus Decompression illness
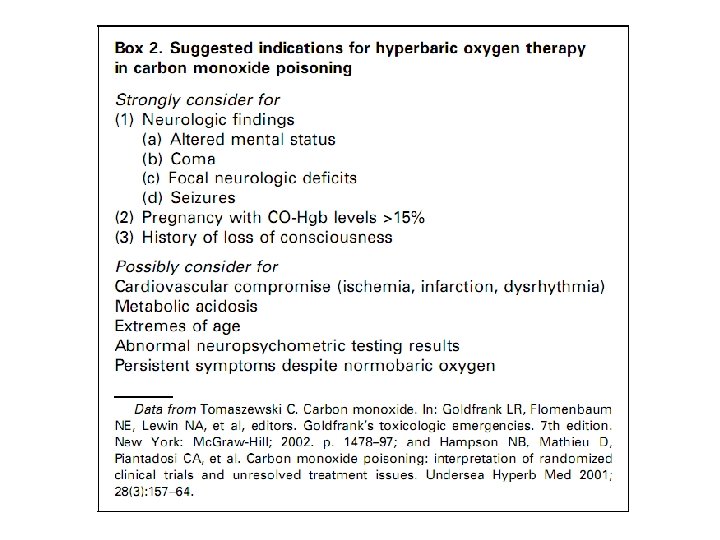
Carbon monoxide poisoning and use of hyperbaric oxygen
Carbon monoxide A colorless, odorless, non-irritating gas produced primarily by incomplete combustion of any carbonaceous fossil fuel Burning charcoal has become a popular way of attempting suicide in Hong Kong Incidence rate increased from 6% to 28% in the period between 1998 and 2001 Second most common method of suicide in Hong Kong Med J 2003; 9: 419 -26
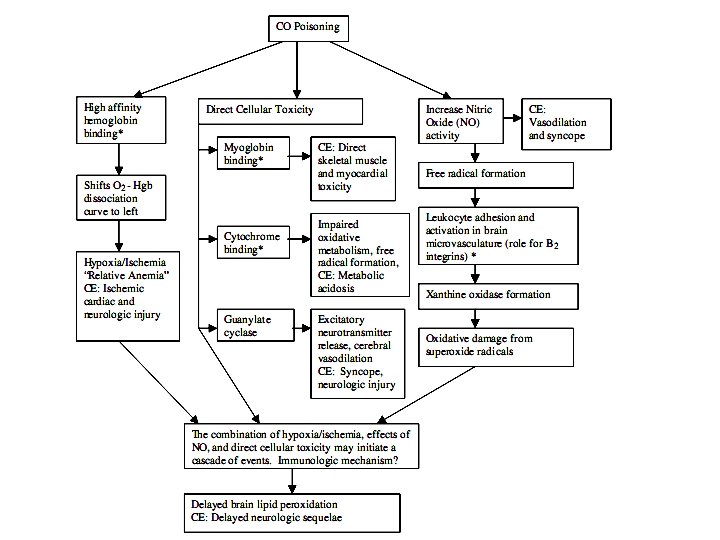
Pathophysiology Hemoglobin binding ◦ Affinity more than 200 times that of oxygen Decreasing oxygen delivery to the tissues and resulting in tissue hypoxia Am J Physiol 1944; 141: 17 -31
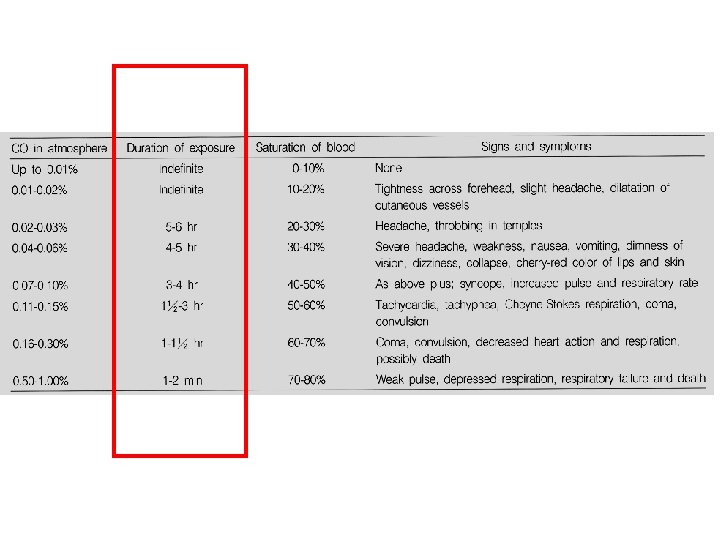
Acute effects
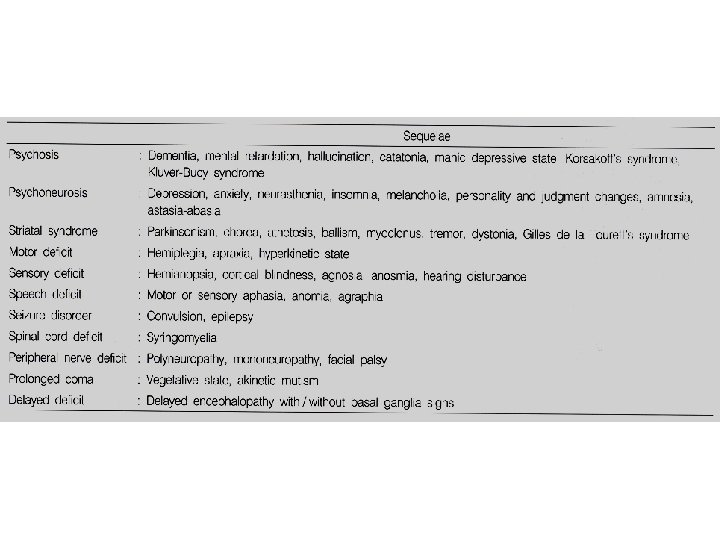
Delayed neurologic sequelae (DNS) Latency period of 2 to 40 days Ranged from 1 -47% More frequent in those present with coma, in older patients and those with prolonged exposure
CO poisoning in pregnancy CO crosses the placenta readily Fetal CO-Hgb levels reach higher peak and eliminate more slowly than maternal CO-Hgb Even in mildly symptomatic mothers, the effect on fetus may be severe ◦ Stillbirth ◦ Anatomic malformations ◦ Neurologic disability Fetal brain damage located at basal ganglia and globus pallidus Ann Emerg Med 1988; 17(7): 714 -7 J toxicol Clin. Toxicol 1982; 19(3): 297 -301 Neurology 1976; 26(1): 15 -23
General CO poisoning management ◦ Maintain an open airway and assist ventilation if necessary ◦ Give supplemental oxygen (100% O 2 shorten elimination t 1/2 from 6 hrs to 1 hrs) ◦ Continuously monitor the ECG, haemodynamic condition and provide support if needed ◦ Treat seizures ◦ Consider the possibility of cyanide poisoning , methemoglobinemia and irritant gas injury
History HBO for CO poisoning was first discussed by Haldane JS in the 1890 s Haldane JS was known for experimentation on himself to find the amount of carbon dioxide in the blood was a stimulus for the respiratory centre of the brain. He reported on investigations of the effects of carbon monoxide from mine fires and explosions (1896). He produced the first staged decompression tables and apparatus (1907). He also invented a gas mask used in WW I.
Potential benefit of HBO Hastens elimination of COHb (t½ decrease from 4 -6 hr to <30 min) Increase tissue oxygen delivery Promote CO dissoication from cytochrome-C oxidase Reduce brain lipid peroxidation Inhibit neutrophil activation and adhesion Science 1950; 111: 652 -4 Toxicol Appl Pharmacol 1990; 105: 340 -4 J Clin Invest 1992; 89: 666 -72 Toxicol Appl Pharmacol 1993; 123: 248 -56
Trial of normobaric and hyperbaric oxygen for acute carbon monoxide intoxication Prospective unblinded RCT 4 groups of patients, started within 12 hr No LOC: A 0 (170) NBO x 6 hr vs A 1 (173) HBO 2 ATA 2 h + 4 h NBO -> FU 1 mo -> 34 vs 32% with DNS LOC: B 1 (145) HBO 1 session vs B 2 (141) 2 session HBO -> FU 1 mo -> 46 vs 48% with DNS Conclusion: HBO is useful in those with LOC but multiple sessions of HBO may not give extra benefit Rahael et al: Lancet. 1989 Aug 19; 2(8660): 414 -9
Non-comatose patients with acute carbon monoxide poisoning: hyperbaric or normobaric oxygenation? 24 non comatous patients, RCT 100% NBO vs 100% HBO (2. 8 ATA) for 2 h, followed by NBO x 10 h COHb normalized both group NBO: more EEG abnormalities and reduced cerebral blood flow reactivity to acetazolamide Conclusion: HBO reduces the time of initial recovery and the number of delayed functional abnormalities in non-comatose patients with acute CO poisoning. Ducasse JL et al: Undersea Hyperb Med. 1995 Mar; 22(1): 9 -15.
Delayed neuropsychologic sequelae after carbon monoxide poisoning: prevention by treatment with hyperbaric oxygen. Prospective RCT, unblinded 65 non-comatose patients, within 6 hrs of removal from exposure All patients given 100% O 2 till HBO started HBO: started within 6 hr, 2. 8 ATA x 30 min than 2 ATA x 90 min NBO: till symptom resolved (mean 4. 2 h) 4 wk FU DNS: 23% vs 0% in favor of HBO Conclusion: HBO treatment decreased the incidence of DNS after CO poisoning. Thom et al: Ann Emerg Med. 1995 Apr; 25(4): 474 -80.
Randomized prospective study comparing the effects of HBO vs 12 hours NBO in non-comatose CO-poisoned patients Prospective unblinded RCT 575 non-comatose patient HBO 2. 5 ATA 90 min vs 12 hr NBO 1 month FU DNS 23% vs 26%, no significant difference between groups Conclusion: no significant benefit of HBO over NBO on CO poisoning Mathieu et al: Undersea Hyperb Med 1996, 23: suppl 27
Hyperbaric or normobaric oxygen for acute carbon monoxide poisoning: a randomised controlled clinical trial Prospective, double blinded, RCT 230 patients, average COHb 21%, 50% with hx of LOC, within 7 hr Daily 100 min 100% O 2 tx within hyperbaric chamber, 60 min 2. 8 ATA HBO or 1 ATA NBO, three days 1 month FU was 46% DNS 65% vs 58% in favor of NBO Conclusion: HBO therapy did not benefit, and may have worsened, the outcome Scheinkestel et al: Med J Aust. 1999 Mar 1; 170(5): 203 -10
Hyperbaric oxygen for acute carbon monoxide poisoning Prospective double RCT 152 patients, started within 24 hr, 65% HBO: 1 session 3 ATA 1 hr and 2 ATA with LOC 1 hr, followed by 2 sessions 2 ATA 2 hr at 6 -12 hr intervals NBO: sham tx at 1 ATA FU 12 mos DNS 25 vs 46% in favor of HBO Conclusion: Cognitive sequelae were less frequent in the HBO Weaver et al: N Engl J Med. 2002 Oct 3; 347(14): 1057 -67
Managing carbon monoxide poisoning with hyperbaric oxygen Prospective unblinded, RCT 153 patients with hx of LOC HBO: 2 ATA 1 hr followed by NBO 4 hr NBO: 6 hr NBO tx FU 1 mo DNS HBO 42% vs NBO 39%, no difference Conclusion: HBO did not benefit the outcome Raphael et al: J Toxico Clin Toxico 2004; 42: 455 -6
Favour HBO Favour NBO Cochrane Database Syst Rev. 2005 Jan 25; (
Existing randomized trials do not establish whether the administration of HBO to patients with carbon monoxide poisoning reduces the incidence of adverse neurologic outcomes. Additional research is needed to better define the role , if any, of HBO in the treatment of patients with carbon monoxide poisoning
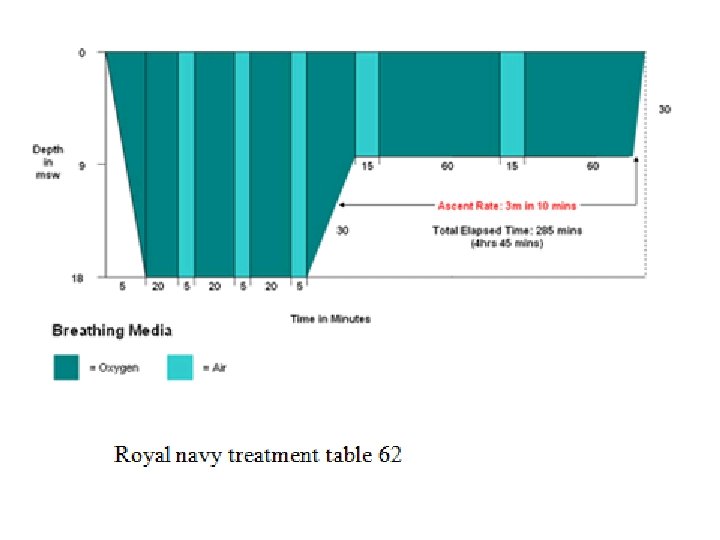
US Royal Navy table 60 2. 8 bar
Decompression illness nitrogen bubbles forming in the bloodstream and tissues of the body move from deep water towards the surface in a short period of time. Type I ◦ Skin symptoms, lymph node swelling, joint/muscle pain
Type II decompression illness Arterial gas embolism ◦ CNS – dizziness, paralysis, numbness, blurred vision, convulsion ◦ CVS – cardiopulmonary arrest ◦ pneumothorax ◦ Pneuomperitoneum ◦ Inner ear – tinnitus, hearing loss, vertigo, dizziness, nausea and vomiting
Protocol for ICU patients undergoing HBO treatment Hazards exist if HBO therapy is not done with proper preparation and monitoring Balance between benefit obtained from HBO therapy and risk associated should be considered by ICU doctors
Medical conditions requiring special consideration before HBO –Respiratory • COPD / Asthma • URTI • Hx of thoracic surgery • Hx or presence of pneumothorax • CXR with asymptomatic pulmonary lesions –Otolaryngologic • Chronic sinusitis • Hx of ear surgery –Ophthalmologic • Hx of optic neuritis –Neurological • Seizure disorder Insert chest drain before –Haematological HBO • Congenital spherocytosis –Systemic • Viral infection • Hyperthermia –Others • Pregnancy ENT assessment to ensure normal eustachian tube function and may need prophylactic myringotomy
Try to simplify patient’s treatment and monitoring Explain the risk and benefit to patients and relatives, get the consent Experienced ICU doctor should accompany the patient during the whole treatment period although he /she may not need to enter the pressure chamber Doctors on call of the hyperbaric chamber should be contacted directly
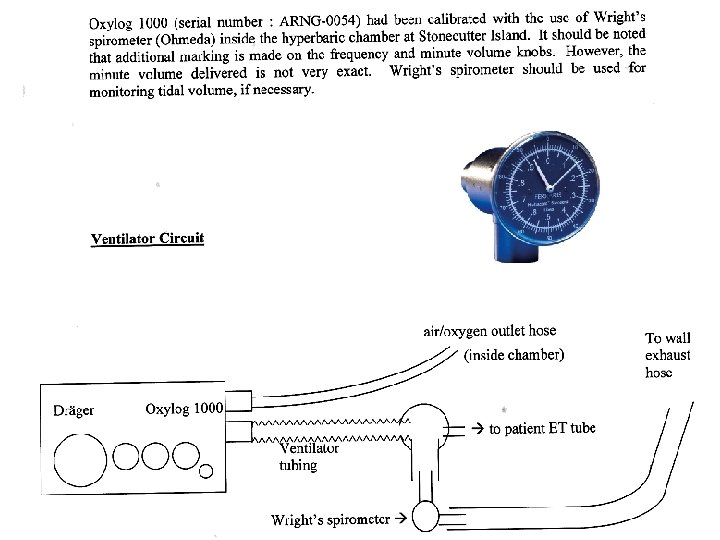
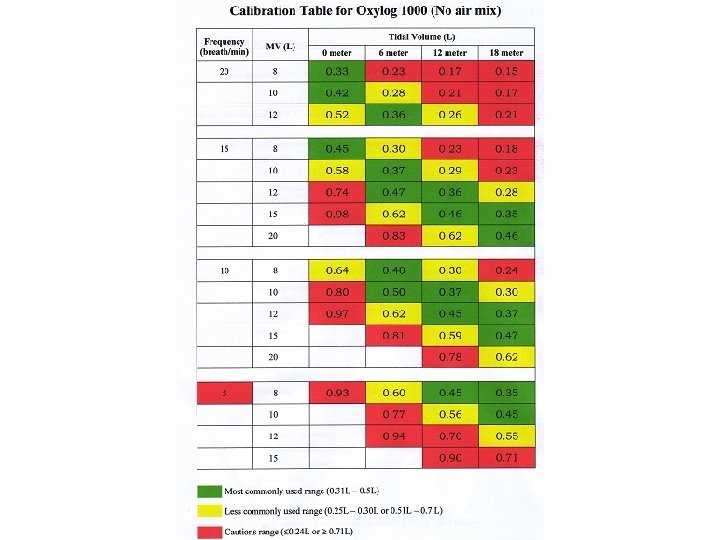
ETT / tracheostomy tube ◦ Use water to inflate the cuff Mechanical ventilator system ◦ Oxylog 1000 is to be used within the chamber ◦ When the chamber pressure is changed, tidal volume delivered to patient will change accordingly and required adjustment ◦ Wright’s spirometer should be connected to the ventilator circuit for TV monitoring ◦ Anesthetic PEEP valve can be used if needed
Chest tube drainage systems ◦ Must have thoracostomy apparatus ready available within the chamber Chest drain box ◦ Maintain suction, monitor air-fluid level during ascent and descent ◦ Substitute with one-way valve (eg Heimlich valve) Oxygen breathing device ◦ Use of O 2 within the chamber must be controlled carefully ◦ Only aqueous solutions should be used because of fire hazards
IV infusion equipment ◦ Avoid glass bottles ◦ Iv infusion pump may carry potential fire hazard ◦ Ensure absolutely no air entrapment ◦ Avoid puncturing rubber injection sites and use 3 way stopcocks Nasogastric tubes ◦ Leave unclamped or on intermittent suction Central line placement ◦ Avoid subclavian puncture ◦ For PAC, ensure balloon at catheter tip is deflated and balloon port must be left open, avoid obtaining wedge pressure during the dive
Monitoring equipment ◦ Space. Lab monitor is available within chamber ◦ For intra-arterial pressure monitoring Further inflate pressure bag during compression and deflate during decompression Avoid air entrapment within tubing Zero pressure transducer with reference to chamber pressure ◦ Function of pulse oximeters / capnography may be unreliable ◦ Do not put monitor with a hot wire stylus inside the chamber ◦ Make sure all device attached to patient’s body are HBO compatible
Injections ◦ Avoid IM/ SC injection because of impaired absorption due to vasocontriction secondary to HBO ◦ Be careful with multiple use vial Defibrillation ◦ Should only be done when the patient was surfaced because of fire hazard Suction device ◦ Available inside chamber Foley catheter ◦ Ensure balloon inflated with water
NIBP ◦ Do not use mercury filled type Staff accompanying patient should not carry combustible materials ◦ Cigarettes, matches, lighters ◦ Oil based cosmetic, face cream, body oil, hair spray ◦ Nylon clothing ◦ Ink filled pen ◦ Electronic devices ◦ Pagers, mobile phone, watches (except diving watch)
Potential HBO complications associated with ◦ Barotrauma Most commonly involve the ear on descent, other sites including sinuses, lungs, teeth ◦ Oxygen toxicity Acute toxicity usually presented with seizure Other symptoms: palpitation, bradycardia, sweating, nausea, vertigo, hallucination ◦ Claustrophobia ◦ Reversible worsening of visual acuity ◦ Transient GI pain ◦ Fire / explosion hazards
Occupational safety and health for staff Normal eustachian tube function No hx of pneumothorax, COPD, chest surgery Not pregnant No recent diving
Occupational safety and health for staff No flying after dive for at least 24 hr Stop at least 48 hrs before another dive Recognize symptoms of complications ◦ Barotrauma esp. ears ◦ Decompression illness eg joint pain / numbness/ weakness Inform OMD if DCI occur
Stonecutters Island (Ngong Shuen Chau)
Control panel with the fireman
Main entrance
Entry lock
Drinking water Sanitary facility Communication facility
Wright’s spirometer
Oxygen hose
CO poisoning, PYNEH, 20072008 7 cases 3 M, 4 F All survived
AN uneventful Patient Gender Age COHb% HBO energy pain emotion sleep social physical 1 F 34 18. 9 X 2 F 30 31 X 3 F 46 45 X X 4 5 6 7
Thank you! THE END