CC Wong PYNEH Skin cancer Nonmelanoma Basal cell

CC Wong PYNEH

Skin cancer Non-melanoma Basal cell carcinoma Squamous cell carcinoma Dermatofibrosarcoma Merkel cell carcinoma Kaposi sarcoma Angiosarcoma Melanoma

Non-melanoma skin cancer

Non-melanoma skin cancer Most common cancer in the USA Over 1, 000 new cases in the USA per year Fair skinned population
 Ionizing radiation Chemical exposure eg. arsenic")
Risk factors Environmental factors Sunlight exposure (Ultraviolet radiation) Ionizing radiation Chemical exposure eg. arsenic agent Patient factors Genetics disease Precursor lesion HIV and HPV infection

UV radiation

More carcinogenic 95%

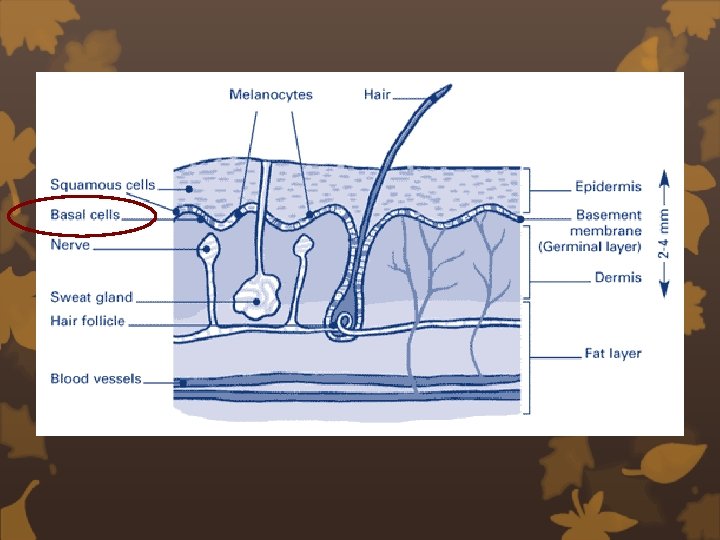
Basal cell carcinoma

Basal cell carcinoma 75% of non-melanoma skin cancer Male : female = 3: 2 Sunlight exposure Head & neck Slow growing Rarely metastasizes

Basal cell carcinoma Nodular most common, pearly appearing papule Pigmented more frequent in darker-skinned population Cystic bluish or gray cystic nodule Superficial scaly patch-like lesion pink to red to brown
 aggressive variant scar-like appearance with ill-defined")
Basal cell carcinoma Micronodular aggressive variant Morpheaform (infiltrating) aggressive variant scar-like appearance with ill-defined border

Squamous cell carcinoma

Squamous cell carcinoma Second most common skin cancer Male : female = 2 -3: 1 Sunlight exposure Old scar, chronic inflammation and ulcer Area of pre-exiting skin damage Faster growing

Squamous cell carcinoma Actinic keratosis: precursor Bowen's disease: SCC in-situ Unhealed ulcer with "heaped up" edge Enlarging lesion irregular border Cranial nerve dysfunction perineural invasion


Diagnosis Clinical diagnosis Incisional / excisional biopsy Imaging

Treatment

Surgical excision Major treatment method High clearance rate ~95% in both SCC and BCC Low recurrence rate (in 5 year) 5. 8% in SCC, <2% in BCC N. R. Telfer et al. British J of Dermatology. 2008 Murad Alam et al. N Engl J Med. 2001

How much margin should we take?
 Trunk & extremities <2 cm Head &neck <1")
BCC Lesion Low risk Margin (mm) Trunk & extremities <2 cm Head &neck <1 cm Around eyes, ears, nose, mouth, hand feet <6 mm 4 -5 High risk Recurrent tumor Immunocompromised Previous radiation site Perineural invasion Micronodular, sclerosing, morpheaform 10

SCC Lesion Low risk Trunk & extremities <2 cm Head &neck <1 cm Margin (mm) 4 -5 Around eyes, ears, nose, mouth, hand feet <6 mm High risk Recurrent tumor Immunocompromised Previous radiation site Perineural invasion Poorly differentiated Adenoid, adenosquamous, desmoplastic 10

Facial H area

Mohs' micrographic surgery Frederic E. Mohs in 1938 Complete circumferential peripheral and deep margin assessment Performed in stages / single day 5 year local control rate SCC BCC Primary 96. 9% 99% Recurrent 90 -93. 3% 94. 4% Murad Alam et al. N Engl J Med. 2001 Nicole W. J. et al. The Lancet 2004

Mohs' micrographic surgery Preserve healthy skin tissue Time consuming High cost

Mohs' micrographic surgery Important site: eyelids, ear, nose, lips, nasolabila fold, forehead, scalp or embryonic fusion plane Recurrence Size >2 cm Perineural involvement Poorly defined margins in high-risk area Nicole W. J. et al. The Lancet 2004

Radiation therapy Primary vs adjuvant 5 -year local control rate ~90% Multiple visits No histological result Side effect: dermatitis, telangiectasia Contraindication: Genetic condition eg. xeroderma pigmentosa Connective tissue disease I. R. Aguayo-Leiva et al. Actas Dermosifiliogr. 2010

Electrodesiccation and Curettage Indication: Small lesion <1 cm Superficial Well-defined 5 -year local control rate: 95% in low risk BCC Multiple attempts No histopathology I. R. Aguayo-Leiva et al. Actas Dermosifiliogr. 2010 N. R. Telfer et al. British J of Dermatology. 2008

Cryotherapy Liquid nitrogen Frozen the skin -> tissue necrosis Multiple cycles 5 -year recurrence rate: 8% in low risk BCC No histopathology Good cosmetic result I. R. Aguayo-Leiva et al. Actas Dermosifiliogr. 2010 N. R. Telfer et al. British J of Dermatology. 2008

Cryotherapy Indication: Low risk BCC Size <1 cm Superficial, nodular Well-defined margin I. R. Aguayo-Leiva et al. Actas Dermosifiliogr. 2010 N. R. Telfer et al. British J of Dermatology. 2008

Topical immunotherapy Imiquimod Toll-like receptor 7 agonist Modify the immune response -> antitumor activity -> tumor cell apoptosis 5 application a week for 6 week Indication: Small superficial BCC Initial response rate 89. 6% Lack of long term data Excellent cosmetic result I. R. Aguayo-Leiva et al. Actas Dermosifiliogr. 2010

Photodynamic therapy Photosensitizing agent followed by illumination of visible light Produced activated oxygen molecule -> destroy target cell Usually 2 cycles 5 -year recurrence rate: 14% Excellent cosmetic effect I. R. Aguayo-Leiva et al. Actas Dermosifiliogr. 2010

Photodynamic therapy Limited penetration Indication: Superficial lesion Depth <2 mm I. R. Aguayo-Leiva et al. Actas Dermosifiliogr. 2010

5 -Fluorouracil Topic chemotherapeutic agent Blocking DNA synthesis Apply twice a day for minimum 6 week Cure rate: 93% Indications: Superficial BCC Small ~1 cm Local inflammatory response I. R. Aguayo-Leiva et al. Actas Dermosifiliogr. 2010

Interferon Intralesional injection Induce apoptosis 3 injections per week for 3 week Complete response rate: 50 -80% Indications: Surgery could be disfiguring Not a surgical candidate Influenza-like symptom I. R. Aguayo-Leiva et al. Actas Dermosifiliogr. 2010

Conclusion Non-melanoma skin cancer Common Rate of cure is high with proper treatment in local disease Surgical excision is associated with lowest recurrence rate Other non-surgical treatment Early superficial disease Non-surgical candidates

Thank you

SLN No definite guideline Lack of large scale study on nonmelanoma skin cancer Renzi et al. : 22 patients Reschly et al. : 9 patients Useful in high risk SCC

Involved margin ~30 -41% do not recur Re-excision of margin Mohs micrographic surgery Radiotherapy
- Slides: 39