Farmacoterapia dellasma Categories of Medications Longterm control maintenance

 medications – Corticosteroids – Long-acting beta-agonists –")
 medications – Short acting -2 agonists –")
 Classification of Asthma Severity 1 2 3 4")
")

 (Modificatori malattia) Barnes, Nature Reviews Drug Discovery 3; 831 -844 (2004)")

. Onset: 5 min,")





 or albuterol (USAN) is a short-acting β 2 adrenergic receptor")
-DBTA Resolution: Harteley, et al 16 Total yield of (+)-DBTA Resolution 30 -40%. Greater")

 Dose/puff Metoproterenol (Alupent, Metaprel) 650 mcg")


-albuterol §Potent binding to the 2 -receptor ++ § Intracellular Ca ; Airway reactivity")



 Ventolin) 2 -4 puffs prn 2")
 • Long acting betaagonist/bronchodilator • Binds to an exosite adjacent to the")








 determina: • Rilassamento bronchiale; • Inibizione del")
 Aumento frequenza,")

 è metabolizzata ad ac. 1, 3 -dimetil")


 Somministrazione per via orale (150 mgx 4 die) e parenterale")

 Nausea, vomito, cefalea,")
 • Daxas, è il primo di una nuova classe di farmaci")


 • • • Drugs which bind to cholinergic receptor")
 12. 1 Atropine easily racemised • • • Racemic")
 12. 2 Hyoscine (scopolamine) • • • Source -")
 12. 3 Comparison of atropine with acetylcholine • •")
 12. 4 Analogues of atropine Ipratropium (bronchodilator & anti-asthmatic)")

 12. 6 SAR for Antagonists R' = Aromatic or")





 – Inhibits 5 -lipoxygenase – Blocks production of all")


 • Dosing: – ages 15 & older: 10 mg po daily –")


 • 600 mg po four times a day • Drug interactions –")
 • 20 mg po BID • Drug interactions – Warfarin, aspirin, theophylline,")



 Inhalation Aerosol Tilade (nedocromil")


 is a drug which was developed for the treatment of respiratory")









 • Immunosoppressione con diminuzione delle")

 Asthma Severity Score Placebo 0. 6 0.")
 Bronchodilator Use 2. 5 Placebo 2. 0 1. 5")


 • Dysphonia • Systemic effects at high doses")








 • Proven as effective as combination therapy with separate flovent and")








 e delle terapie di rimpiazzo nicotinico (NTR) ad")




- Slides: 116
Farmacoterapia dell’asma
Categories of Medications • Long-term control (maintenance) medications – Corticosteroids – Long-acting beta-agonists – Leukotriene modifiers – Cromolyn and nedocromil – Methylxanthines
Categories of Medication • Quick relief (rescue) medications – Short acting -2 agonists – Anticholinergics
NAEPP (National Asthma educatio prevention program) Classification of Asthma Severity 1 2 3 4 Severe Persistent Moderate Persistent Mild Intermittent
E per le malattie broncopolmonari croniche ostruttive (BPCO)
Modello concettuale della immunopatogenesi dell’asma bronchiale • Le Ig. E si legano ai mastociti nelle mucose delle vie respiratorie che liberano istamina, triptasi, PGD 2, LTC 4 e PAF = broncocostrizione immediata e riduzione della FEV 1 (Forced Expiratory Volume one second – Volume espiratorio massimo al secondo). Inoltre si sintetizzano e si rilasciano citochine, IL-4 e IL-5, TNF- , GM-CSF, (fattore stimolante le colonie granulocitariemacrofagiche), TGF (tissue growth factor), il LTB 4. Le citochine, il LTB 4 ed il TNF- inducono l’espressione di molecole di adesione endoteliale (ICAM, VCAM), richiamano e stimolano eosinofili e neutrofili che a loro volta producono ECP (proteina cationica degli eosinofili) e MBP (proteina basica maggiore), proteasi. Tali fattori provocano edema, ipersecrezione mucosa, costrizione della muscolatura liscia. Inoltre si ha la produzione di ROS (NO, O 2 - e ONOO-), specie altamente ossidanti che ulteriormente distruggono i tessuti circostanti. Inoltre…. .
(Sintomatici) (Modificatori malattia) Barnes, Nature Reviews Drug Discovery 3; 831 -844 (2004)
Treatment • Bronchodilators. There are three types of bronchodilators used clinically: • β 2 -agonists, • anticholinergics • methylxanthines. These drugs relax the smooth muscles of the airway allowing for improved airflow. Many patients feel less breathless after taking bronchodilators.
β 2 -agonisti • ad azione rapida (salbutamolo, terbutalina, fenoterolo, orciprenalina). Onset: 5 min, durata: fino a 6 h • protratta (salmeterolo, formoterolo) Onset: 20 -30 min, durata: fino a 12 h • Si somministrano per via inalatoria (topica) in sospensioni con particelle di 2 -5 micron di diametro che raggiungono facilmente i bronchi di piccolo calibro
Historic • Initially, subcutaneous injections of epinephrine were used, followed by a nebulized epinephrine solution. • Epinephrine is one of the most potent vasopressor (i. e. causes constriction of the blood vessels and corresponding rise in blood pressure) drugs known. • Epinephrine affects respiration primarily by relaxing the bronchial muscle. • Epinephrine is rapidly metabolized by COMT, primarily in the liver.
Equal selectivity for Both and -receptors Greater selectivity for receptors Perhaps, still greater selectivity for -receptors could be Generated by appending larger alkyl substituent on nitrogen
An improvement! • Isoprenaline was synthesized by German chemists in the 1940’s • It had less cardiovacular side effects than adrenaline • Became the most widely used inhaled treatment for asthma for the next 20 years.
Further improvements needed • Needed an agent which was longer lasting, more resistant to COMT • Needed an agent which was more selective for the 2 receptors in the lung and less selective for the 1 receptors of heart.
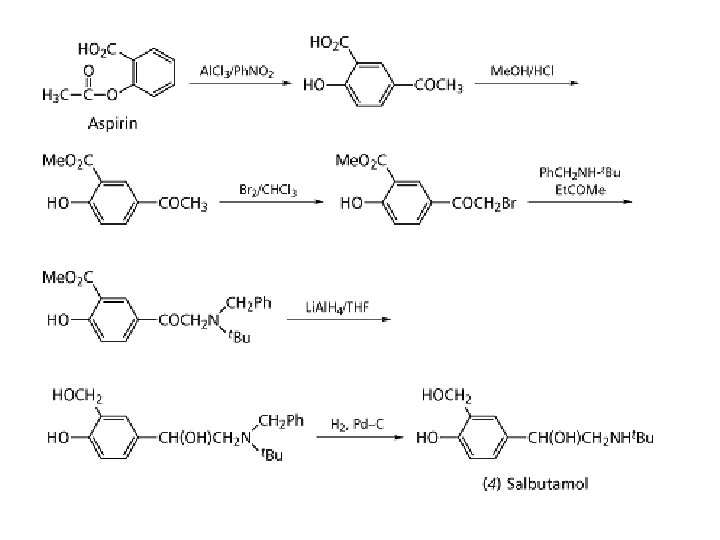
Arrives Salbutamol • Tert-butyl group renders salbutamol more selective for 2 • Hydroxymethyl group (in place of OH) renders salbutamol resistant to COMT • Remains the most widely used antiasthma drug in the world
Salbutamol • Salbutamol (INN) or albuterol (USAN) is a short-acting β 2 adrenergic receptor agonist used for the relief of bronchospasm in conditions such as asthma and COPD. Salbutamol sulphate is usually given by the inhaled route for direct effect on bronchial smooth muscle. This is usually achieved through a metered dose inhaler (MDI), nebuliser or other proprietary delivery devices (e. g. Rotahaler or Autohaler). In these forms of delivery, the effect of Salbutamol can take place within 5 to 20 minutes of dosing. Salbutamol can also be given orally or intravenously. However, some asthmatics may not respond to these medications as they will not have the required DNA base sequence in a specific gene. Salbutamol became available in the United Kingdom in 1969 and in the United States in 1980 under the trade name Ventolin.
(+)-DBTA Resolution: Harteley, et al 16 Total yield of (+)-DBTA Resolution 30 -40%. Greater than 99. 5% pure R-salbutamol The process is advantageous as the process are short and efficient. Optical resolution of racemic alcohols by diastereoisomeric complex formation with O, O -dibenzoyl-(2 R, 3 R)-tartaric acid.
Short-acting -2 agonists • Mechanisms – -2 agonist effects (smooth muscle relaxation due to increased cyclic AMP) – Repeated high dose exposure to agonist leads to down regulation of receptors • Side effects – Tachycardia – Tremor – Hypokalemia, hypomagnesemia – Increased lactic acid – Hyperglycemia
ß 2 Agonists Short Acting (3 -6 hr) Dose/puff Metoproterenol (Alupent, Metaprel) 650 mcg Albuterol (Proventil, Ventolin) 90 mcg Bitolterol (Tornalate) 370 mcg Pirbuterol (Maxair) 200 mcg Terbutaline (Brethaire) 200 mcg Long Acting (12 hr +) Salmeterol (Serevent) Diskus) Formoterol 21 mcg (50 mcg in 12 mcg
SAR 2 - Agonisti Albuterol Metoproterenol Bitolterol Pirbuterol Terbutaline
Oral β 2 Agonists • Less effective than inhaled beta agonists • Produce more adverse effects • Have a slower onset of action • Oral syrup may be useful for young children and elderly with infrequent mild symptoms who cannot use an inhaler and spacer device *Medical Letter Vol 42 Page 20
(R)-albuterol §Potent binding to the 2 -receptor ++ § Intracellular Ca ; Airway reactivity § Eosinophil activation §Rapid metabolism §No effect on mucus production § Ciliary beat frequency & mucocilary transport velocity
§Very limited binding to b 2 - receptor ++ § Intracellular Ca ; Hyperresponsiveness § Eosinophil activation; Mast cell histamine release §Metabolized at 1/10 th the rate of (R)albuterol § Mucus production by epithelial cells § Ciliary beat frequency & mucociliary transport velocity (S)albuterol
Levalbuterol “Levoalbuterol…appears to have NO clinically significant advantage over racemic albuterol” The Medical Letter. Volume 41, Page 51. “Levalbuterol, the R-isomer of racemic albuterol, offers no clinically significant advantage over racemic albuterol” The Medical Letter. Volume 42, Page 19.
Long-Acting Bronchodilators Dose Character Albuterol Salmeterol (Proventil, (Serevent) Ventolin) 2 -4 puffs prn 2 p q 12 (MDI) 1 p q 12 (Diskus) Formoterol (Foradil) 1 p q 12 Hydrophilic Lipophilic Hydrophilic & Lipophilic Onset of action Rapid (2 -5 minutes) Duration Short (4 -6 hours) Delayed (>30 minutes) Long (12 hours)
Salmeterol (Serevent) • Long acting betaagonist/bronchodilator • Binds to an exosite adjacent to the regular beta receptor • Slower onset of action – maximum effect in 3 hours • Longer duration of action (12 hours)
Salmeterol is a long-acting beta 2 -adrenergic receptor agonist drug that is currently prescribed for the treatment of asthma and chronic obstructive pulmonary disease COPD. It is currently available in both dry-powder inhalers (DPIs) and pressurised metered dose inhalers (p. MDIs). It is a long acting beta-adrenoceptor agonist (LABA), usually only prescribed for severe persistent asthma following previous treatment with a short-acting beta agonist such as salbutamol and is prescribed concurrently with a corticosteroid, such as beclometasone. The primary noticeable difference of salmeterol to salbutamol is that the duration of action lasts approximately 12 hours in comparison with 4 -6 hours of salbutamol.
10% lung deposition, 90% swallowed
CS-30 Chemical Structures Formoterol O HN O HO OH N H Salmeterol HO HO O OH N H
CS-31 Exosite model proposed by johson et al.
CS-32 Diffusion microkinetic model Salbutamolo Formeterolo Salmeterolo
Pharmacologic Differences: β 2 Receptor Binding for Formoterol Differs From Salmeterol u Both molecules bind to the β 2 adrenergic receptor active site, however – Prolonged salmeterol activity depends on binding with an exosite – Prolonged activity of formoterol is independent of exosite binding u Mutation in the exosite region (Ile 164) could affect duration of action of salmeterol Green SA, et al. J Biol Chem. 1996; 271: 24029 -24035. CS-33
β 2 -agonisti: meccanismo d’azione β 2 -recettore
2 -agonist MLCK phosphorylation 2 -receptors S. muscle relaxation Inhibition PI hydrolysis Sequestration of intracellular calcium Calcium extrusion Activation of calcium gated potassium channels Inhibition mediator release
L’aumento del c. AMP (β 2 -agonisti) determina: • Rilassamento bronchiale; • Inibizione del release di mediatori flogogeni dai mastociti/macrofagi; • Aumento della clearence mucociliare
Catecolamine e recettori • Recettori β-adrenergici Cuore (β 1 e β 2) Aumento frequenza, contrattilità e velocità di conduzione Rene ap. jux. -glom. (β 1) Aumento renina Bronchi (β 2) Broncodilatazione Muscolatura liscia vasale (β 2) Rilasciamento m. scheletrici, renali, coronarie, Pancreas (β 2) Aumento insulina Fegato (β 2) Glicogenolisi, gluconeogenesi T. adiposo (β 3) Catabolismo trigliceridi α 1 α 2 β 1 β 2 β 3 Adrenalina ++ ++ +++ + α 1 α 2 β 1 β 2 β 3 Noradrenalina +++ ++ +++
Effetti collaterali dei 2 -agonisti • Cardiocircolatori: tachicardia, aritmie, alterazioni elettrocardiografiche, ischemia miocardica, “myocardial contraction band necrosis” • Controndicati in pazienti cardiopatici: può provocare aritmie e morte • Neuromuscolari: tremori, agitazione, insonnia • Metabolici: iperglicemia, aumento degli ac. grassi non esterificati, ipo. K, ipo. Mg ed ipo. PO 4, iperinsulinemia
Teofillina* • La teofillina (1, 3 -dimetilxantina) è metabolizzata ad ac. 1, 3 -dimetil urico dal CYP 1 A 2 (8 -idrossilazione) e parzialmente dal CYP 2 E 1 a 1 -metilxantina per 3 demetilazione *Si usa il sale di etilendiamina o aminofillina
Teofillina: meccanismo d’azione Inibizione = accumulo di c. AMP
Meccanismo d’azione della teofillina • Inibizione delle PDE ed accumulo di c. AMP ; • Antagonismo su recettori adenosinici (A 1 -, A 2 A -, A 2 B-receptors) • Aumento del rilascio di catecolamine • Inibizione del rilascio di prostaglandine e TNF - • Inibizione della traslocazione di NF-k B • Aumento apoptosi • Possibile diminuzione della trascrizione geni proinfiammatori per interferenza con istone deacetilase
Farmacocinetica della teofillina 1) Somministrazione per via orale (150 mgx 4 die) e parenterale (e. v. 5 mg/kg per infusione lenta fino a 25 mg/min; i. m. e rettale); 2) Legame alle proteine plasmatiche 60%; 3) Metabolismo epatico (CYP 1 A 2) (variazioni individuali); 4) Emivita: da 3, 5 a 9 h;
Toxicity • Nausea, vomiting, diarrhea • Irritability, insomnia • Seizures, hyperthermia, brain damage • Hyperglycemia, hypokalemia, hypotension, arrhythmias • Must monitor levels
Effetti collaterali e tossici della teofillina (concentrazione ematica > 20 mg/l) Nausea, vomito, cefalea, ipotensione, brividi, palpitazioni, tachicardia, convulsioni In infusione rapida può provocare aritmie e morte
Roflumilast (Daxas® ) • Daxas, è il primo di una nuova classe di farmaci per il trattamento della BPCO ed anche il primo trattamento antinfiammatorio specifico per la BPCO. • Il farmaco è stato recentemente approvato dalla European Medicine Agency (EMA), è già disponibile in Germania, Inghilterra e in altri Paesi europei, e dovrebbe entrare in commercio a breve nella maggior parte degli altri Paesi europei, compresa l’Italia. • Daxas® è indicato per la terapia di mantenimento della BPCO di grado severo (FEV 1 inferiore al 50% dopo broncodilatazione) associata a bronchite cronica nei pazienti adulti con storia di frequenti riacutizzazioni, in aggiunta al trattamento con broncodilatatori.
Meccanismo d’azione • • • Roflumilast è un inibitore della PDE 4, un agente antinfiammatorio, nonsteroideo, studiato per attaccare sia l’infiammazione sistemica sia quella polmonare associate alla BPCO. Il meccanismo d’azione è l’inibizione della PDE 4, il principale enzima responsabile del metabolismo dell’adenosin monofosfato ciclico (c. AMP) situato nelle cellule strutturali ed infiammatorie importanti per la patogenesi della BPCO. Roflumilast agisce sulle varianti strutturali 4 B e 4 D della PDE 4 A con una potenza simile in un range nanomolare. L’affinità alle varianti strutturali PDE 4 C è più bassa di 5 -10 volte. Questo meccanismo d’azione e la selettività si applicano anche a roflumilast N-ossido, che è il principale metabolita attivo di roflumilast. Roflumilast è estensivamente metabolizzato nell’uomo, con la formazione di un metabolita principale farmacodinamicamente attivo, roflumilast N-ossido. Poiché sia roflumilast che roflumilast N-ossido contribuiscono entrambi alla attività inibitoria sulla PDE 4 in vivo, le considerazioni farmacocinetiche sono basate sull’attività inibitoria totale sulla PDE 4 (cioè sulla esposizione totale a roflumilast N-ossido).
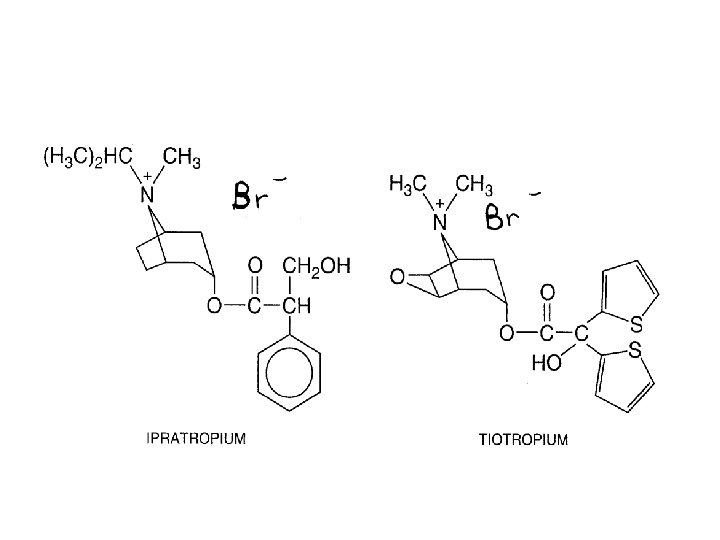
Anticolinergici correntemente utilizzati • Ipratropio bromuro • Ossitropio bromuro • Tiotropio bromuro* * Farmaco a lunga durata di azione (1 sola somministrazione/die), in quanto ha una dissociazione lenta dai recettori muscarinici M 1 e M 3
12. Cholinergic Antagonists (Muscarinic receptor) • • • Drugs which bind to cholinergic receptor but do not activate it Prevent acetylcholine from binding Opposite clinical effect to agonists Postsynaptic nerve Ach Ach Antagonist © 1
12. Cholinergic Antagonists (Muscarinic receptor) 12. 1 Atropine easily racemised • • • Racemic form of hyoscyamine Source - roots of belladonna (1831) (deadly nightshade) Used as a poison Used as a medicine decreases GIT motility antidote for anticholinesterase poisoning dilation of eye pupils CNS side effects - hallucinations © 1
12. Cholinergic Antagonists (Muscarinic receptor) 12. 2 Hyoscine (scopolamine) • • • Source - thorn apple Medical use treatment of motion sickness Used as a truth drug (CNS effects) © 1
12. Cholinergic Antagonists (Muscarinic receptor) 12. 3 Comparison of atropine with acetylcholine • • • Relative positions of ester and nitrogen similar in both molecules Nitrogen in atropine is ionised Amine and ester are important binding groups (ionic + H-bonds) Aromatic ring of atropine is an extra binding group (vd. W) Atropine binds more strongly than acetylcholine © 1
12. Cholinergic Antagonists (Muscarinic receptor) 12. 4 Analogues of atropine Ipratropium (bronchodilator & anti-asthmatic) • • • Analogues are fully ionised Analogues unable to cross the blood brain barrier No CNS side effects © 1
The combination preparation ipratropium/salbutamol is a formulation containing ipratropium bromide and salbutamol sulfate (albuterol sulfate) used in the management of chronic obstructive pulmonary disease (COPD) and asthma. It is marketed by Boehringer Ingelheim as metered dose inhaler (MDI) and nebuliser preparations under the trade name Combivent. Medications commonly used in asthma and COPD (primarily R 03) edit Anticholinergics: Ipratropium, Tiotropium Short acting β 2 -agonists: Salbutamol, Terbutaline Long acting β 2 -agonists (LABA): Bambuterol, Clenbuterol, Fenoterol, Formoterol, Salmeterol Corticosteroids: Beclometasone, Budesonide, Ciclesonide, Fluticasone Leukotriene antagonists: Montelukast, Pranlukast, Zafirlukast Xanthines: Aminophylline, Theobromine, Theophylline Mast cell stabilizers: Cromoglicate, Nedocromil Combination products: Budesonide/formoterol, Fluticasone/salmeterol, Ipratropium/salbutamol © 1
12. Cholinergic Antagonists (Muscarinic receptor) 12. 6 SAR for Antagonists R' = Aromatic or Heteroaromatic Important features • Tertiary amine (ionised) or a quaternary nitrogen • Aromatic ring • Ester • N-Alkyl groups (R) can be larger than methyl (unlike agonists) • Large branched acyl group • R’ = aromatic or heteroaromatic ring • Branching of aromatic/heteroaromatic rings is important © 1
Anticolinergici correntemente utilizzati • Queste molecole sono usate per uso topico inalatorio • Escrete immodificate nelle feci • Gli effetti collaterali sistemici sono scarsi; si può avere secchezza delle fauci. • Meno efficaci dei 2 -agonisti a cui possono essere associati; attivi su sottogruppi di pazienti asmatici, efficacia ridotta nel trattamento cronico. • Usati anche nel trattamento dell’attacco acuto d’asma
Combivent • Ipratropium/Albuterol • Indicated for COPD for patients who were not controlled with single therapy • Not FDA approved for use in asthma • Contraindicated with soy allergy – Some dosage forms may contain soya lecithin
Tiotropio RESPIMAT® 2, 5 microgrammi (dose totale 5 microgrammi in 2 erogazioni da 2, 5 microgrammi una volta al giorno) ha un effetto terapeutico paragonabile a tiotropio Handi. Haler® 18 microgrammi 9. RESPIMAT® è un dispositivo pratico da usare, multi dose, con indicatore di dosaggio, che contiene una quantità di farmaco sufficiente per un mese di terapia. *Tiotropio è commercializzato con il nome commerciale di SPIRIVA®. *Inalatore Predosato a Idrofluoroalcano, Turbohaler®, Diskus® Tecnologia avanzata; facilità d'uso Per utilizzare tiotropio RESPIMAT® il paziente deve semplicemente girare la base dell'inalatore di 180 gradi. Con questa operazione viene compressa la molla che provvederà a far salire la dose prestabilita del principio attivo nel tubo capillare e di qui a una micro pompa. L'inalatore che eroga la fine nebulizzazione Soft Mist™ è stato realizzato applicando i principi d'uso consolidato nella tecnologia dei microchip.
Leukotriene Modifiers
Leukotriene Modifiers • Leukotrienes are one of many mediators active in patients with asthma • Cysteinyl LT’s have major role in asthma – Bronchoconstriction – Airway hyperresponsiveness – Vascular permeability – Increased mucous production • LTB 4 less well understood – Neutrophil chemoattractant
Leukotriene Modifiers • Zileuton (Zyflo) – Inhibits 5 -lipoxygenase – Blocks production of all leukotrienes • Zafirlukast (Accolate) – Leukotriene receptor antagonist – Blocks only effects of LTC 4, D 4, E 4 • Montelukast (Singulair) – Newest agent – Also leukotriene receptor antagonist
5 -LO inhibitors - zileuton Cysteinyl-LT receptor antagonists - zafirlukast montelukast
Clinical Effects • Increase in FEV 1 by 10 -15% • Reduces – Beta-agonist use – Daytime and nocturnal symptoms • Often used in combination with inhaled steroids – Potentially first-line in mild asthma – Consider in mild asthma and allergic rhinitis • Treatment of choice in aspirin-
Montelukast (Singulair) • Dosing: – ages 15 & older: 10 mg po daily – ages 6 -14: 5 mg chewable dose daily – ages 2 -5: 4 mg chewable dose daily • Recommended to take dose in the evening • Can be taken with or without food
Montelukast
Cys. LTs-receptor antagonists LTD 4 Pranlukast Zafirlukast Montelukast
Zileuton (Zyflo) • 600 mg po four times a day • Drug interactions – Theophylline, propranolol, warfarin • Monitor hepatic function – Every month x 3 months – Then every 3 -4 months • Can take without regard to meals • Approved for use down to age 12
Zafirlukast (Accolate) • 20 mg po BID • Drug interactions – Warfarin, aspirin, theophylline, erythromycin • Rare hepatic events reported • Rare cases of Churg-Strauss • Absorbed poorly with food – Take 1 hour pre- or 2 hours postmeals • Approved for use down to age 12
Effetti collaterali degli antileucotrienici • Alcuni soggetti trattati hanno sviluppato la sindrome di Churg-Strauss (vasculite sistemica, eosinofilia, sinusite e rinite), probabilmente indotta dalla riduzione della dose di glucocorticoidi • Alcuni casi di epatopatie con alterazione dei parametri ematici con zafirlukast
Cromoni • “Stabilizzazione” della membrana dei mastociti/macrofagi con inibizione del rilascio di mediatori flogogeni, inibizione della produzione di Ig. E, inibizione delle fibre C (neuroni sensori), forse mediata da inibizione canali del cloro espressi neuroni sensori • Sono utilizzati nella profilassi per la terapia dell’asma bronchiale. Non hanno attività broncodilatatoria. • Si somministrano per via inalatoria
Inibitori della liberazione di mediatori chimici Cromolyn sodium Nedocromil
Last reviewed on Rx. List: 7/29/2008 Tilade® Inhaler (nedocromil sodium) Inhalation Aerosol Tilade (nedocromil sodium) is an inhaled anti-inflammatory agent for the preventive management of asthma. Nedocromil sodium is a pyranoquinoline with the chemical name 4 H-Pyrano[3, 2 -g]quinoline -2, 8 -dicarboxylic acid, 9 -ethyl-6, 9 -dihydro-4, 6 -dioxo-10 -propyl-, disodium salt, and it has a molecular weight of 415. 3. The empirical formula is C 19 H 15 NNa 2 O 7. Nedocromil sodium, a yellow powder, is soluble in water. The molecular structure of nedocromil sodium is: Chemical Class: Pyranoquinoline Tilade Inhaler (nedocromil sodium inhalation aerosol) is a pressurized metered-dose aerosol suspension for oral inhalation containing micronized nedocromil sodium and sorbitan trioleate, as well as dichlorotetrafluoroethane and dichlorodifluoromethane as propellants. Each Tilade canister contains 210 mg nedocromil sodium. Each actuation meters 2. 00 mg nedocromil sodium from the valve and delivers 1. 75 mg nedocromil sodium from the mouthpiece. Each 16. 2 g canister provides at least 104 metered actuations. After 104 metered actuations, the amount delivered per actuation may not be consistent and the unit should be discarded. Each Tilade Inhaler canister must be primed with 3 actuations prior to the first use. If a canister remains unused for more than 7 days, then it should be reprimed with 3 actuations.
Cromolyn sodium and Nedocromil • Block chloride channel of mast cells – Mast cell stabilizers – Decrease histamine release • Inhibit neutrophil chemotaxis • Nedocromil also inhibits eosinophil degranulation
Barnes, Nat Rev Drug Discov. 3: 831 -844, 2004
CILOMILAST Cilomilast (ARIFLO) is a drug which was developed for the treatment of respiratory disorders such as asthma and Chronic Obstructive Pulmonary Disease (COPD). It is orally active and acts as a selective Phosphodiesterase-4 inhibitor. Phosphodiesterase (PDE) inhibitors, such as theophylline, have been used to treat Chronic Obstructive Pulmonary Disease (COPD) for centuries; however, the clinical benefits of these agents have never been shown to out-weigh the risks of their numerous adverse effects. Four clinical trials were identified evaluating the efficacy of cilomilast, the usual randomized, double-blind, and placebo -controlled protocols were used. It showed reasonable efficacy for treating COPD, but side effects were problematic and it is unclear whether cilomalast will be marketed, or merely used in the development of newer drugs. Cilomilast is a second-generation PDE 4 inhibitor with antiinflammatory effects that target bronchoconstriction, mucus hypersecretion, and airway remodeling associated with COPD.
ARIFLO • • Glaxo. Smith. Kline filed for drug approval with the US FDA at the end of 2002 and in January 2003 with the European Medicines Evaluation Agency (EMEA). In October 2003 the FDA issued an approvable letter for use of Ariflo in maintenance of lung function in COPD patients poorly responsive to salbutamol, despite an earlier decision by the FDA advisory panel to reject approval. Before issuing final approval, however, the FDA has requested additional efficacy and safety data. This is likely to focus on sustainability of clinical benefits and safety of Ariflo in long-term use.
Asthma Treatment Summary Mild Intermittent Use: Albuterol, Asthma Action Plan Mild Persistent Use: Albuterol and Controller medications (low dose steroids, nedocromil, cromolyn, montelukast) Moderate Persistent Use: Combination of medications (low to medium dose steroid plus long acting beta agonist, and/or Leukotriene modifiers) Severe Persistent Use: High dose inhaled steroids, long acting beta agonist, and leukotriene modifier. May need oral steroids
Cellular effect of corticosteroids, Barnes et al. , Ann. Int. Med. , 139, 359 -370, 2003
Structure/activity relationships • Functional groups essential for and which delineate aldosterone or cortisol activity: • double bond at D 4 • C 3 ketone • C 20 ketone
Structure/activity relationships • • • Functional groups essential for glucocorticoid activity: C 21 hydroxyl C 11 ketone or hydroxyl In vivo, C 11 ketone gets reduced to b-hydroxyl group. This is the reason why cortisone is active as an antiinflammatory agent). For glucocorticoids, the C 17 a-hydroxyl group enhances activity, but is not essential. For example, corticosterone is active but lacks a C 17 hydroxyl group.
Steroid analogs with antiinflammatory activity • • • Add fluorine to C 9. 9 -a-fluorocortisol has 10 times more activity compared to the parent cortisol. However, it also has 125 times the mineralcorticoid activity, so considerable specificity is lost! Add double bond at C 1. Prednisolone (1, 2 -dehydrocortisol) and prednisone (1, 2 dehydrocortisone) are five times more active than their parent compounds cortisol and cortisone, respectively, without changing mineralcorticoid activity. Add a C 16 methyl group. A methyl group added to either the a or b face increases glucocorticoid activity and decreases mineralcorticoid activity for overall increased selectivity.
Combinations of modifications which optimize antiinflammatory activity • Betamethasone has 25 times and dexamethasone has 30 times the activity of cortisol. Triamcinolone, with a hydroxyl instead of a methyl group, has a shorter duration of action than betamethasone and dexamethasone, but is roughly as potent. None have mineralcorticoid activity. http: //www. neurosci. pharm. utoledo. edu/MBC 3320/glucocorticoids. htm
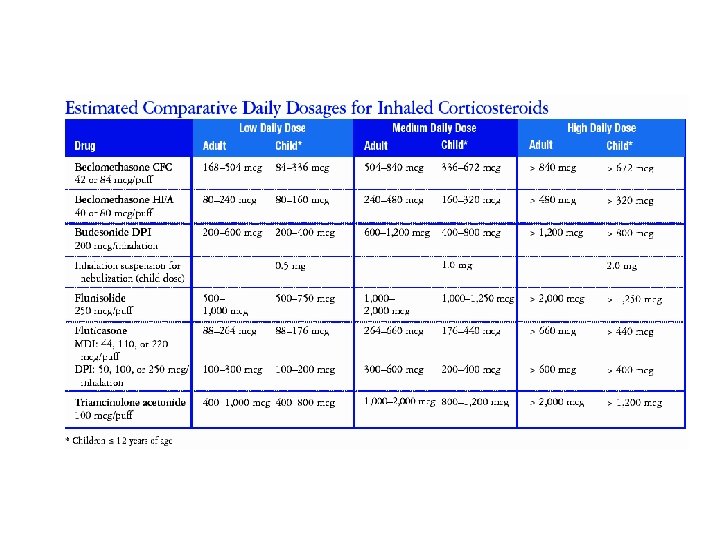
CORTICOSTEROIDI USATI NEI NUOVI DISPOSITIVI Budesonide Mometasone Fluticasone Ciclesonide
Glucocorticoidi: effetti collateri della terapia a lungo termine • Obesità e ridistribuzione del grasso nell’organismo (”buffalo hump, “moon facies”, area sopraclavicolare, strie addominali); • Riduzione dello spessore ed atrofia della cute con difficoltà nella cicatrizzazione delle ferite; • Riduzione delle masse muscolari e miopatie; • Osteoporosi (inibizione osteoblasti, diminuito assorbimento calcio ed aumento PTH, attivazione osteoclasti indiretta, difetti nella mineralizzazione), osteonecrosi; • Modificazioni dell’umore (euforia e psicosi); • Cateratta, glaucoma;
Glucocorticoidi: effetti collaterali della terapia a lungo termine (segue) • Immunosoppressione con diminuzione delle difese naturali contro le infezioni; • Ritenzione idrosalina ed ipertensione (per effetto mineralcorticoide di alcune molecole ed aumento epatico della sintesi di angiotensinogeno ed aumento delle risposte pressorie catecolaminergiche ); • Ritardo della crescita nei bambini; • Dopo trattamento prolungato, inibizione e soppressione dell’asse ipotalamo-ipofisi-surrene ed atrofia surrenalica. L’interruzione della somministrazione deve avvenire gradualmente; • Ulcere peptiche; • Iperglicemia e diabete mellito iatrogeno;
Clinical Effects • Corticosteroids are the most effective treatment for long term control of asthma – Reduce symptoms – Decrease use of bronchodilators – Improve peak flows – Decrease exacerbations • Let’s look at some examples of existing data
Clinical Effectiveness 1. 0 0. 8 (max=6) Asthma Severity Score Placebo 0. 6 0. 4 Inhaled Steroid 0. 2 0 3 6 9 12 Time (Months) Juniper et al. , Am Rev Resp Dis, 1990
Clinical Effectiveness 3. 0 (puffs/day) Bronchodilator Use 2. 5 Placebo 2. 0 1. 5 1. 0 0. 5 Inhaled Bronchodilatator 0 3 6 9 12 Time (Months) Juniper et al. , Am Rev Resp Dis, 1990
Mechanism of Action • Inhibit production of inflammatory cytokines • Decrease number of eosinophils & mast cells • Decrease mucous secretion • Increase synthesis of ß-2 receptors Important with concomitant beta-agonist use
Effects of Inhaled Corticosteroids on Inflammation Compromised Epithelium Intact Epithelium Thickened BM Inflammatory Cells Laitinen et al. J Allergy Clin Immunol 1992; 90: 32 -42
Adverse Effects • Oral candidiasis (thrush) • Dysphonia • Systemic effects at high doses – Potential for pituitary-adrenal axis suppression – Osteoporosis/osteopenia – Growth rate suppression in children
Oral Candidiasis • • Related to total dose Incidence 5 - 10% Spacer reduces incidence Mouth washing helpful – Good recommendation: Use ICS before brushing teeth • Twice a day • Mouth gets rinsed after use
Dysphonia • Occurs in 30 -50% • Related to total dose • Laryngeal myopathy – May diagnose by rhinoscopy • Spacers do not reduce incidence • Maybe less common with dry powder inhalers
Pituitary-Adrenal Axis Suppression • Marked variability from patient to patient • Cumulative dose (inhaled, nasal, oral) important – Probably not clinically significant • No current recommendation for monitoring – Some check annual morning serum cortisol for patients on higher total doses (>1500 mcg/day) • Rare case reports of adrenal crisis in children • No case reports in adults
Pituitary-Adrenal Axis Suppression • Doses of 1500 -2000 mcg more frequently associated with suppression – Most studies looks at urinary cortisol – Clinical significance • Daily doses of 1500 mcg in adults and 400 mcg in children show little suppression • Budesonide 800 mcg/d and flunisolide or triamcinolone up to 1000 mcg/d caused no suppression in children • May be caused by lower doses of fluticasone than other inhaled steroids
Osteoporosis • Risk is not clear – CAMP study: children – no effect on BMD – NEJM 2001: adult women – decreased BMD in hip but no spine or femoral neck - ? significance • Consider in all patients – Calcium daily: 1000 – 1500 mg/d – Vitamin D daily – 400 -800 IU/d – Weight bearing exercise • High dose inhaled or oral steroids – Bone density study – Specific osteoporosis therapy
Effects on Growth • Some studies have shown an effect on short-term growth – Short-term growth in children is highly variable – Approx. 1 cm/year less in some studies • Some evidence that bone age is also delayed proportionately – Final height attained more relevant end-point – Long-term studies to date show no effect on adult height
Oral Bioavailability • Majority of systemic activity comes from steroid that enters the GI tract • 10 -20% of MDI dose reaches the lungs • 80 -90% of dose is swallowed • Spacer device increases the amount of steroid that reaches the lungs – Less available for systemic activity
Triamcinolone - Azmacort • Low dose • Need to take 4 times a day
Fluticasone/Salmeterol DPI (Advair) • Proven as effective as combination therapy with separate flovent and serevent inhalers • Improves compliance – Only one inhalation twice a day required • Diskus dry powder inhaler – Must instruct on delivery technique – Shows number of remaining doses
Patogenesi ASMA BPCO Allergeni Fumo di sigaretta Infiammazione bronchiale Linfociti T CD 4+ Eosinofili Infiammazione bronchiale Linfociti T CD 8+ Macrofagi, neutrofili REVERSIBILE RIDUZIONE DEL FLUSSO AEREO ESPIRATORIO IRREVERSIBILE
BPCO fumatore: TERAPIA • La disassuefazione dal fumo di tabacco è prioritaria e deve essere indicata al primo posto nella terapia consigliata • Al BPCO fumatore motivato a smettere deve essere sempre offerta la possibilità di accedere agli interventi per il trattamento del tabagismo che si sono dimostrati di maggiore efficacia ( counseling intensivo associato a terapia farmacologica), anche ricorrendo agli ambulatori specialistici per la prevenzione e il trattamento del tabagismo ( Centri Antifumo)
Trattamento della BPCO Riduzione dei fattori di rischio • Sono disponibili diverse terapie farmacologiche efficaci ed almeno una di queste dovrebbe essere somministrata in aggiunta ai consigli pratici se necessario ed in assenza di controindicazioni. • Sono considerati di prima scelta i seguenti farmaci: terapia sostitutiva nicotinica, bupropione a lento rilascio e vareniclina.
il fumo di tabacco: aerosol di sostanze nocive: idrocarburi aromatici policiclici, nitrosamine, -benzopirene sost. cancerogene benzoantracene HCN, CH 3 CHO , CH 2 O, NH 3 sost. irritanti CO lega l'emoglobina (=> carbossiemoglobina) Dipendenza e Assuefazione
NICOTINA Aspirata, tramite il circolo ematico, giunge al sistema nervoso, data la sua capacità di attraversare la barriera ematoencefalica Nel brain attiva i recett. acetilcolinergici nicotinici sui corpi cellulari dopaminici dell'Area Ventro-tegmentale e terminali dopaminici del Nucleo Accumbens e stimola la produzione di dopamina a livello della corteccia frontale Inibisce la MAO responsabile della degradazione neurotrasmettitori monoamminergici (Dopa) Azione periferica: Rilascio di Adrenalina dalle ghiandole surrenali Riduzione dei livelli di insulina Iperglicemia Metabolismo accelerato
Terapia sostitutiva con nicotina TIPO DISP. DOS. GOMMA automed. 2 -4 mg CEROTTO automed. 5 (7) mg 10 (14) mg 15 (21) mg INALATORE automed. CPR (subl/menta) automed. 10 mg 2 mg
BUPROPIONE • Il Bupropione, conosciuto anche con i nomi commerciali di Zyban, Wellbutrin, Elontril, è un antidepressivo atipico, di recente commercializzazione in Italia, che agisce inibendo la ricaptazione della dopamina e della noradrenalina. È stato altresì utilizzato, in passato e soprattutto in altri paesi, come molecola antagonista della nicotina; lo scopo principale per il quale tale farmaco è stato studiato e introdotto, riguarda in ogni caso il trattamento della depressione. • La sintesi di questa molecola avvenne nel 1966; tuttavia la sua registrazione avvenne nel 1974, a cura dell'attuale Glaxo. Smith. Kline il farmaco è stato approvato anche come supporto nella terapia per interrompere la dipendenza dal fumo a partire dal 2006, solo dal 2008 si è avviata la diffusione del farmaco sotto copertura totale del SSN. •
Trattamento della BPCO Riduzione dei fattori di rischio • Fra i nuovi farmaci, la vareniclina potrebbe avere un effetto terapeutico aggiuntivo rispetto alle terapie farmacologiche attualmente disponibili nel promuovere la cessazione della abitudine al fumo. • Una recente metanalisi ha evidenziato che la vareniclina aumenta la probabilità di smettere di fumare di circa tre volte rispetto al placebo (astinenza continua a 12 mesi OR 3. 22 ( CI 95% 2. 43 -4. 27) ( K. Cahill, LF Stead, T. Lancaster Nicotine receptor partial agonists for smoking cessation Cochrane Database of Systematic Reviews 2007 , Issue 1. Art. No: CD 006103)
VARENICLINA E’ un’alternativa del bupropione (zyban) e delle terapie di rimpiazzo nicotinico (NTR) ad esempio cerotti di nicotina, gomme l'inhaler e compresse sublinguali Caratteristiche agonista parziale del sottotipo 4 2 del recett. nicotinico per l’Ach Nome IUPAC: 7, 8, 9, 10 -tetrahydro-6, 10 -methano-6 H-pyrazino [2, 3 h][3]benzazepine, (2 R, 3 R)-2, 3 -dihydroxibutanedioate (1: 1) Citisina Vareniclina L’approvazione definitiva del FDA è giunta l’ 11 maggio 2006 L’unico “anti-fumo” non nicotinico
• • quando la V. fitta con il recett. stimola il rilascio di dopamina, sebbene produca un effetto più lento ma più duraturo rispetto alla nicotina. Inoltre V. parzialmente lo blocca (perché agonista “parziale”), riduce il sito di binding disponibile per la nicotina, e qualora il paziente dovesse fumare durante il trattamento, darebbe una risposta meno efficace e il fumo risulterebbe sgradevole • poiché la V ha una affinità maggiore per i recett. Acetilcolinici-nicotinici spiazza la nicotina dal recettore, come il monossido di carbonio spiazza l’ossigeno dall’emoglobina, pertanto limita l’effetto della nicotina. • Non ha un effetto forte come la nicotina nel rilascio di dopamina, quindi il potenziale di assuefazione risulta minore
• La dose standard è 1 mg 2 volte al gg, con variazioni permesse dalla FDA, che ne ha approvato l’uso per 2 settimane; se il paziente smette di fumare, la somministrazione va continuata per altre 12 settimane. • V non è stata testata in adolescenti (under 18) e nemmeno in donne in attesa, pertanto non è raccomandato l’uso in questi soggetti. Donne in allattamento devono evitare questo prodotto, in quanto la v potrebbe fluire nel latte materno, portando ad effetti sconosciuti sul bambino
Effetti collaterali del Chantix • Nausea • headache • Vomiting • Flautulence • Insomnia (30%) • Abnormal dreams • Dysgeusia (alteration in • • taste) Epidermal Rash Dry mouth
SINTESI VARENICLINA