DIAGNOSTIC IMAGING OF BREAST By Dr Viqt Gerald

DIAGNOSTIC IMAGING OF BREAST By Dr Viqt. Gerald Z. S. A. M. Makwaruzi Radiologist and Imaging Specialist Department of Diagnostic Imaging (Radiology)

+BREAST IMAGING. . . INTRODUCTION n Mainstay of breast imaging remains radiographic to date (x-ray discovery 1895) n Breast cancer is the principle indication for mammography and other imaging modalities n Breast imaging is relatively costly: ? Specialized equipment ? One organ ? Limited use

++BREAST IMAGING. . . OVERVIEW A. B. C. D. E. F. G. H. I. J. K. Definitions Anatomy Physiology Indications for Breast Imaging BI-RADS breast composition categories Breast Malignancy Mammography and radiological signs Other Imaging Modalities: Galactography, U/S, MRI, NM Sonography: Equipment and Signs. MRI and Scintimammography BI-RADS mammary assessment categories, Risk of malignancy and Care Plan.
 Exocrine gland that produces milk. 2. IMAGING: The")
A. DEFINITIONS 1. BREAST: (=L, Mamma) Exocrine gland that produces milk. 2. IMAGING: The making of pictures (Medical, for detection of disease) 3. MAMMOGRAPHY: Medical breast imaging using x-rays. Other types of breast imaging, usually specified e. g. CT-Mammography, Scintimammography. 4. MAMMOGRAM = MAMMOGRAPH: Picture record from process of Mammography 5. XEROMAMMOGRAPHY: Mammography by discharging a reusable charged electrostatic plate and use of a special powder (High radiation dose to patient) 6. SONOGRAPHY=ULTRASONOGRAPHY: Imaging employing high frequency sound.
. 8.")
+Definitions…. . 7. SCINTIMAMMOGRAPHY: Breast Imaging using radioactive isotopes (Tc 99 m Sestamibi). 8. (NUCLEAR) MAGNETIC RESONANCE IMAGING: Imaging by means computer-registered interaction and reaction of atomic nuclei in cells of the body to magnetism and radio frequency. 9. POSITRON EMISSION TOMOGRAPHY (PET): Use of positron annihilation energy to make images (from γ-rays). 10. BI-RADS: Breast Imaging Reporting And Data System (ACR). A scheme for putting the findings of mammograms for breast cancer diagnosis into small number of well-defined categories. Adapted to MRI and U/S.

B. ANATOMY
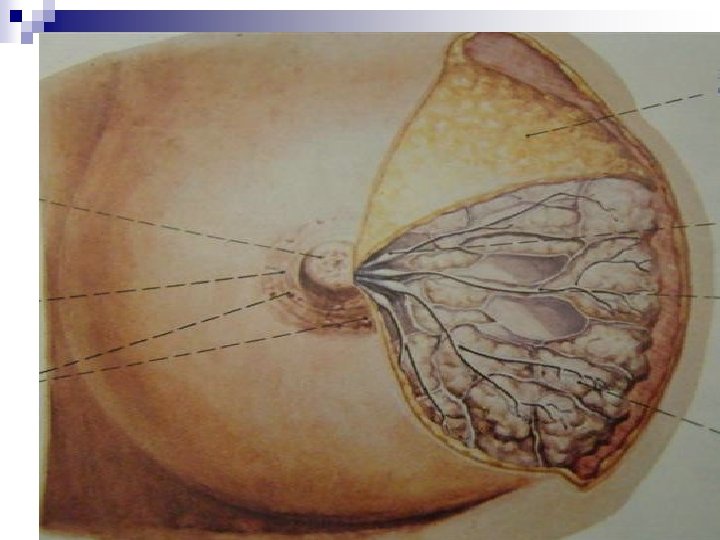
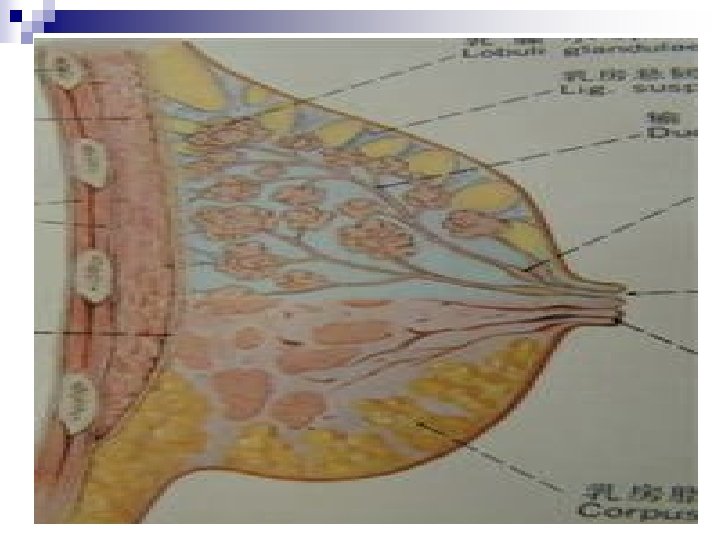

+Anatomy… n HISTOLOGY: ¨ Acini –Cuboidal Epithelium ¨ Smaller Ducts –Columnar Epithelium ¨ Major Ducts –Stratified Squamous Epithelium. n BREAST PARENCHYMA: ¨ 10 – 100 acini = Lobule ¨ Variable lobule number = Lobe ¨ 15 – 20 Lobes =Breast Parenchyma n BREAST STROMA: ¨ Fatty and fibrotic tissue which surrounds and extends into lobule.

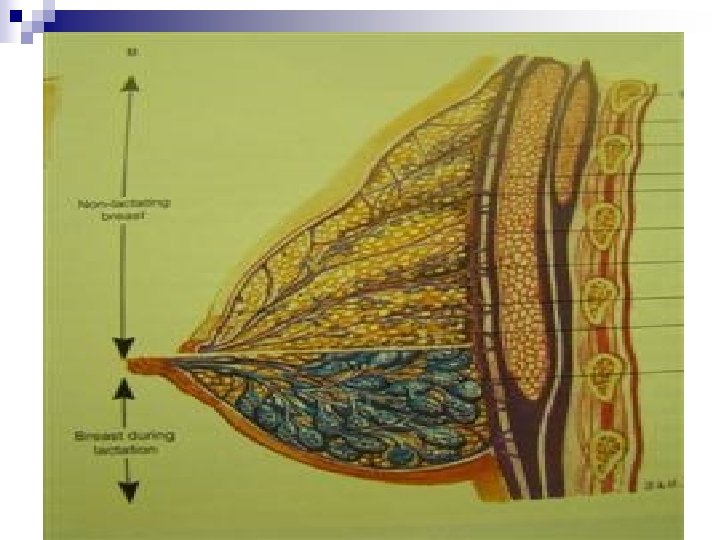
C. PHYSIOLOGY n Number of lobules per lobe and number of acini per lobule vary with Age, Parity and other factors. n Breast tissues undergo cyclic changes under hormones in menstrual cycle n With pregnancy, acini increase in number, hence breast becomes solid glandular tissue, and remains so if breastfeeding occurs. n After pregnancy/lactation –marked decrease in number of acini. n Breast of parous woman is less glandular (↓acini), than nulliparous woman of same age. n Parenchymal atrophy begins in early twenties or after first pregnancy whichever comes first. It continues with advancing age and accelerates at menopause. n Male breast is similar to female but it has no lobules (Male breast cancer always ductal)

D. INDICATIONS FOR BREAST IMAGING n Congenital/Developmental –gynaecomastia n Inflammation –abscess, TB, granulomata, Adenosis n Implants n Neoplasm ¨ Benign –fibroadenoma, ¨ Malignant –carcinoma n Guiding Aspiration/Biopsy n Masses –non specific, cysts, adenomyoepithelioma n Discharges

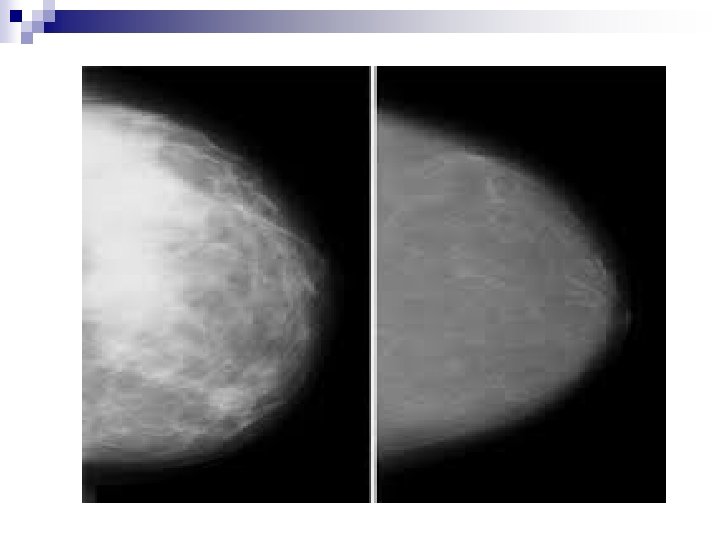
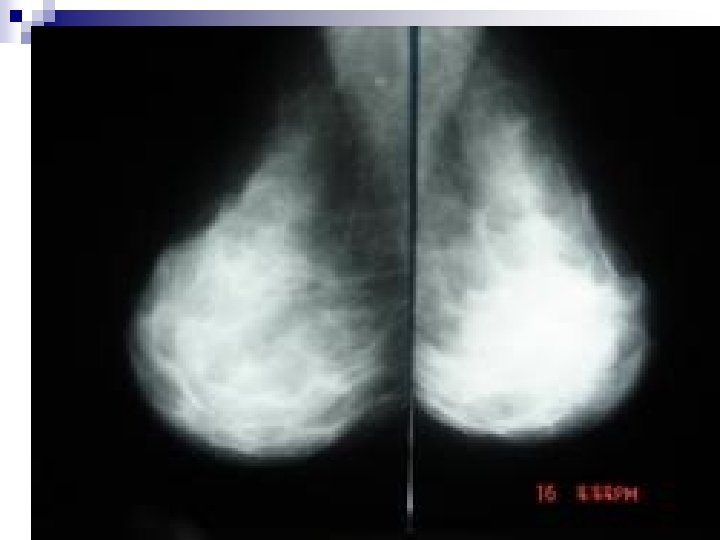
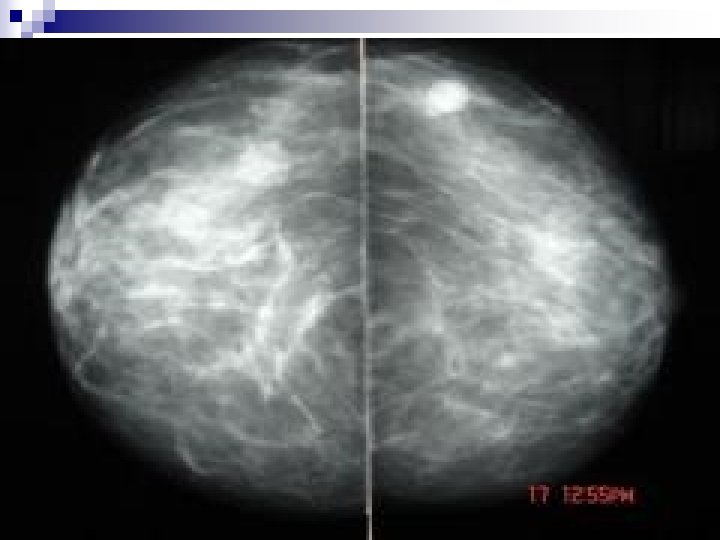
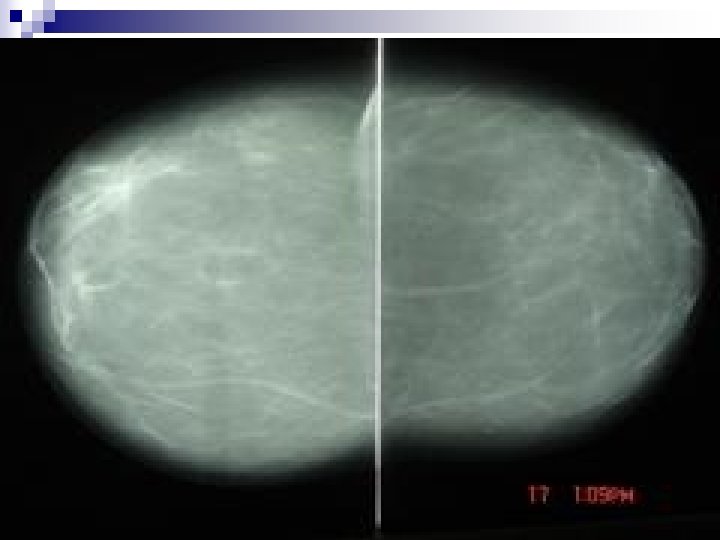
E. BI-RADS Mammographic Breast Composition Categories: a. Breasts are almost entirely fatty. n b. There are scattered areas of fibroglandular density. n c. Breasts are heterogeneously dense, which may obscure small masses. n d. Breasts are extremely dense which lowers the sensitivity of mammography. n



F. BREAST MALIGNANCY n =Cancer of the breast n Primary neoplastic disease in the breast destroying local tissues progressively and seeding distant areas as metastases n In Tanzania, breast cancer is the 3 rd killer cancer (Mortality: 6. 6/100, 000/year) after Cervical cancer (21. 4), and oesophageal cancer (11. 9). (Source, Health Profile Of Tanzania, 2010)

++Breast Malignancy…RISK FACTORS n Risk Doubles with: ¨ Menarche before age 12 yrs ¨ Menopause after age 50 yrs ¨ Nulliparity ¨ Obesity after menopause n Risk increases by factor of 2 to 4: ¨ First childbirth after age 30 yrs ¨ Breast cancer in Mother or Sister ¨ Combination of nulliparity and epithelial hyperplasia ¨ Previous endometrial, ovarian or colon ca.

+++Breast Malignancy…+Risk Factors n Other risk factors ¨ Alcohol ¨ Tobacco ¨ Hormone Replacement Therapy n Actual Facts: ¨ Majority of breast cancers are sporadic ¨ 5 – 10% of breast cancers are hereditary ¨ 70% of breast cancers occur in patients without any risk factors.

++++Breast Malignancy…Types n TYPES: ¨ Ductal Carcinoma in Situ ¨ Invasive Carcinomas n Ductal Ca n Medullary Ca n Lobular Ca n Mucinous Ca n Papillary Ca n Tubular Ca n Paget’s Disease of Nipple ¨ Other cancers


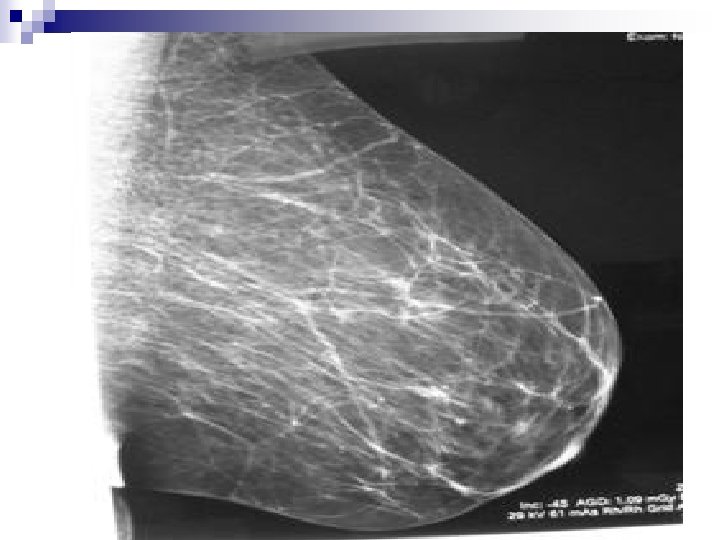
. Commonest imaging modality for the breast n X-rays are")
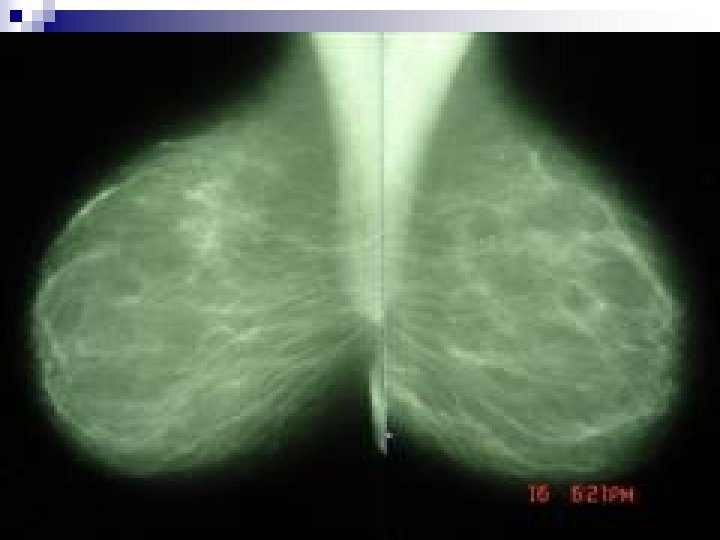
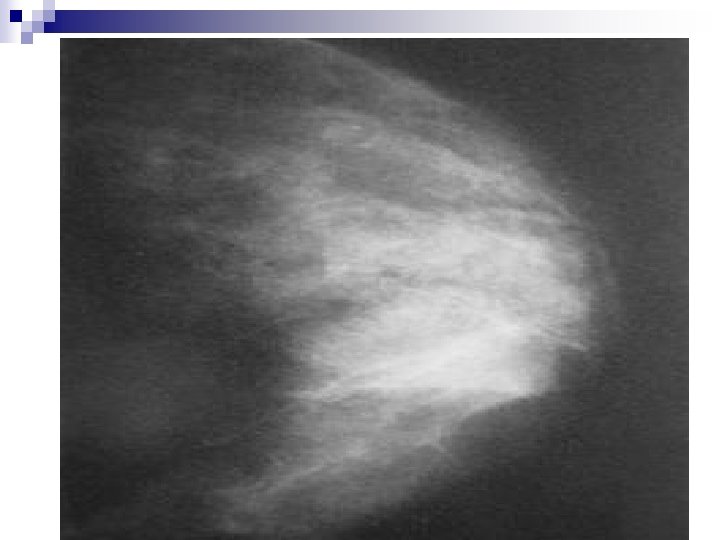
G. MAMMOGRAPHY n (X-ray Mammography). Commonest imaging modality for the breast n X-rays are the imaging energy employed with its potential hazards. n Image receptor and image management are some of reasons for different types of mammography. n Used for Screening or Diagnostic imaging. N. B: Routine Mammographic screening is not recommended in patients ≤ 40 yrs because: -Over all incidence of ca is significantly less -Tissues are more sensitive to ionizing radiation -Mammography is less effective in young dense breast

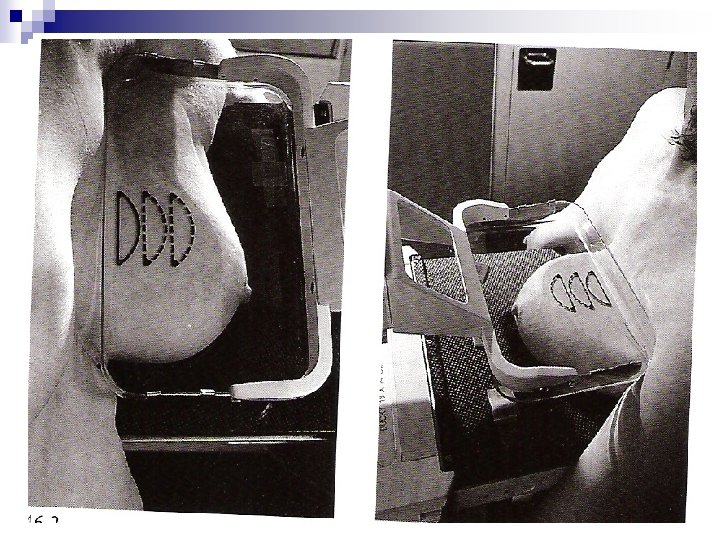
+Mammography. . . EQUIPMENT AND TECHNIQUE q Specialized X-ray Machine q Fine grain film-screen combination q Single coat film q Digital detector q Compression apparatus q Standard and Special Views

++Mammography. . . TIMING q Menstrual cycle and the breast q Ovarian follicular phase: q Breast more compressible q Compression less painful q Glandular tissue less dense q Less radiation risk (in Ovarian Luteal Phase cells are at G 2 stage of the Cell Cycle and more sensitive to ionizing radiation. q Menstrual Cycle factor frequently overlooked.

+++Mammograp hy. . . COMPRESSION Allows visualization of small Ca since normal tissue can spread under compression while Ca persists

++++Mammography. . . IONIZING RADIATION q Total dose absorbed from mammography, normal breast in two planes , about 2 m. Gy (=0. 2 rad) q Radiation sensitivity of breast is greatest in women <30 yrs and negligible ≥ 40 years. q Carcinogenicity depends on absorbed dose, which in turn depends on THICKNESS and DENSITY of breast q “. . . risk of dying from breast cancer induced by mammography. . . is approximately equivalent to the risk of dying of lung cancer from smoking three cigarettes. . ” (Heywang-Kobrunner 2001) q Negligible for breast cancer causation but not for other possible radiation-induced cancers. Cancer is stochastic hazard, no dose is safe.

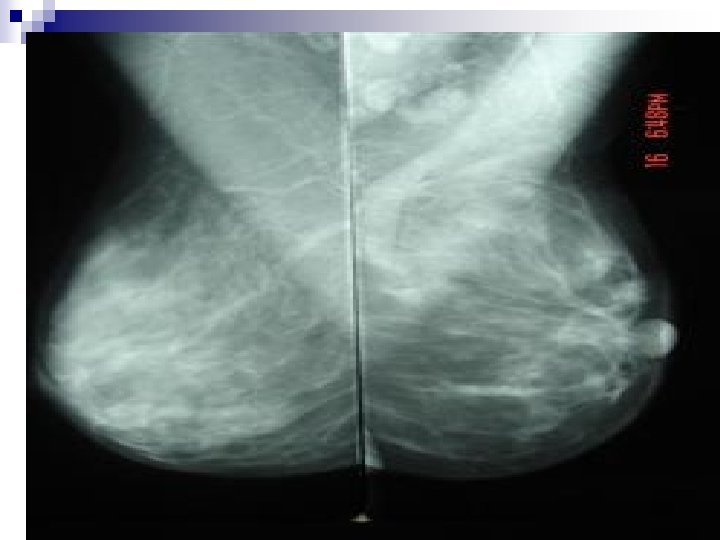
+++++Mammography. . . PROJECTIONS q CC, Craniocaudal q MLO, Mediolateral Oblique q ML, Mediolateral q LM, Lateromedial q MAGNIF, Magnification q XCC exaggerated CC, CV cleavage, AT axillary tail, TAN, RL rolled laterally, RM rolled medially


++++++Mammography. . . RADIOLOGICAL VALUE q 10 – 15% of clinically detected cancers cannot be detected by mammography q About 1/3 rd of breast Ca seen on mammography will not be detected clinically q False positive reports average 25% q Negative X-ray report should not delay biopsy of clinically suspicious area. q Major value of mammography is detection of non-palpable cancer.
,")
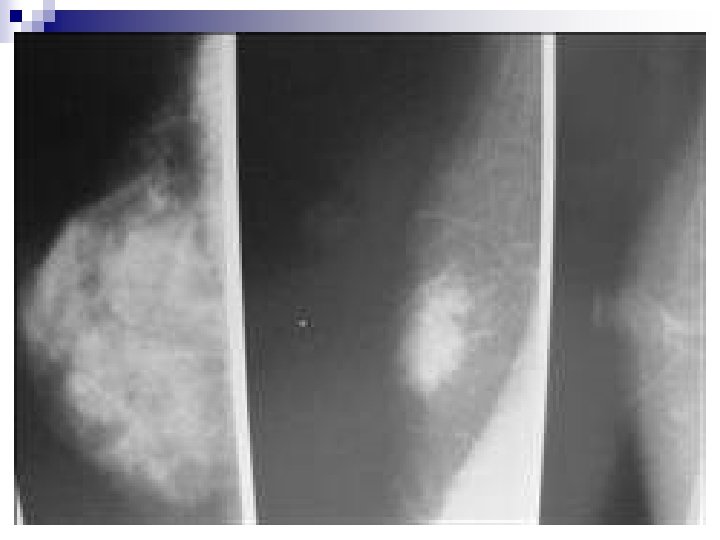
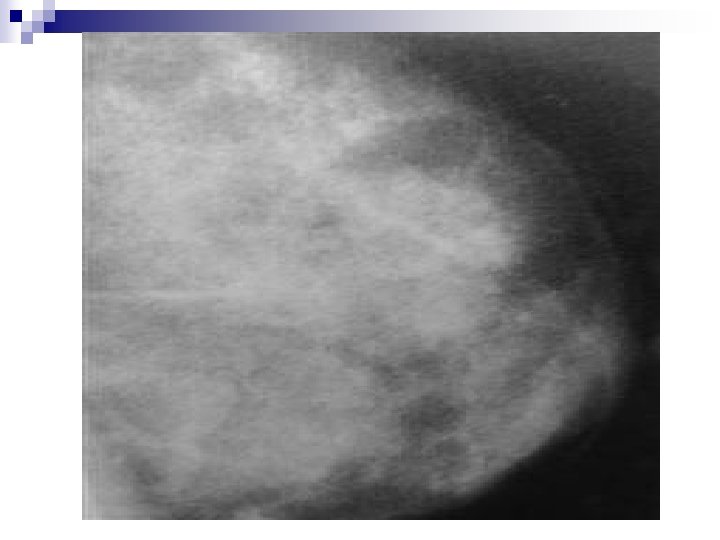
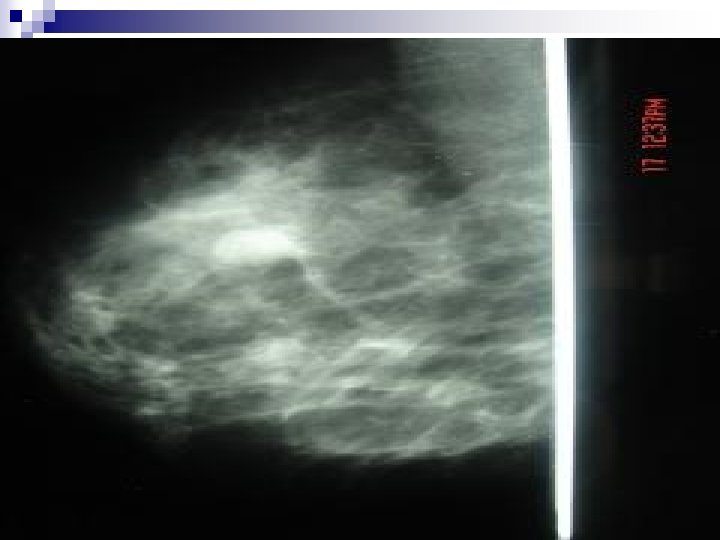
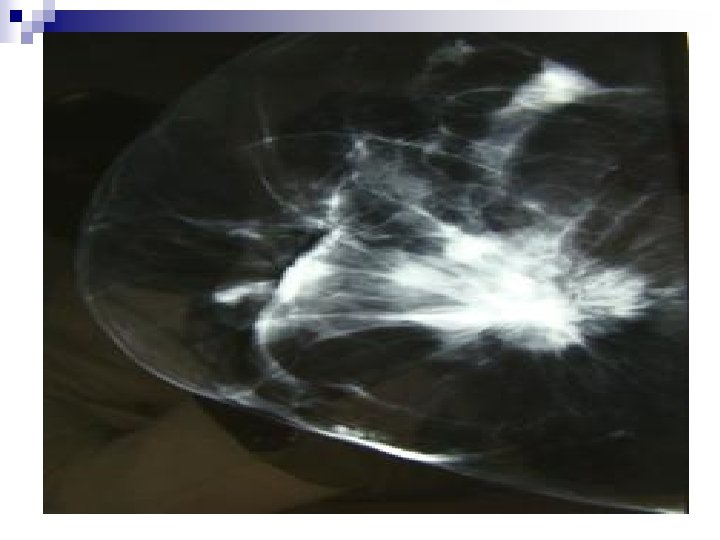
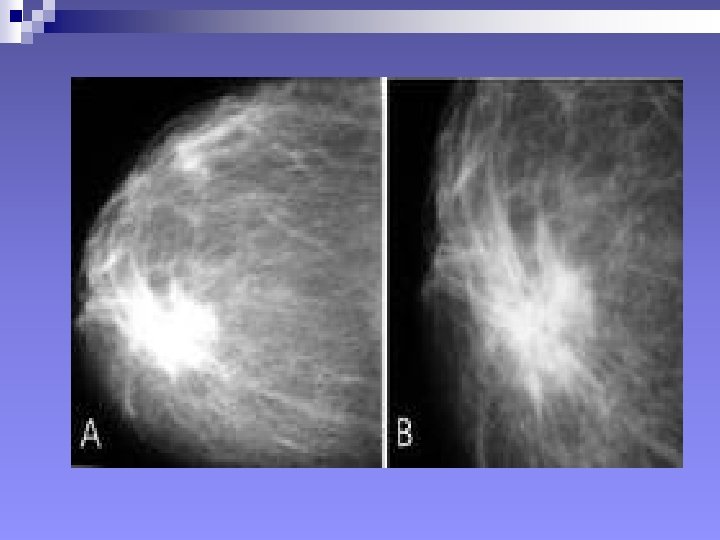
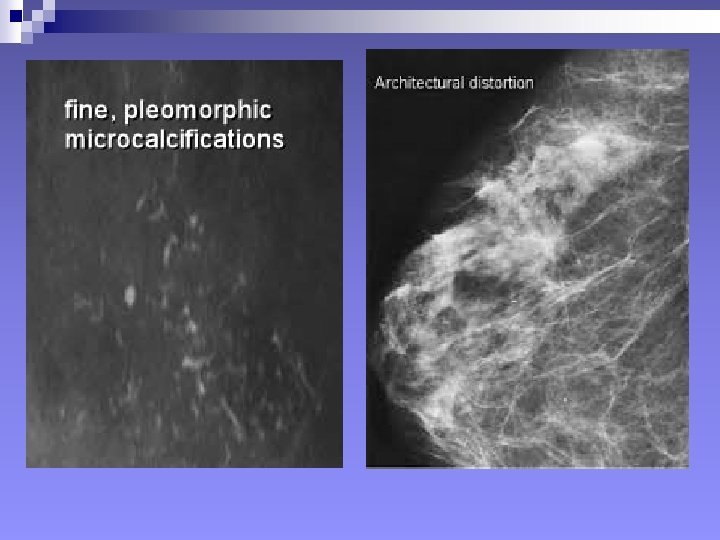
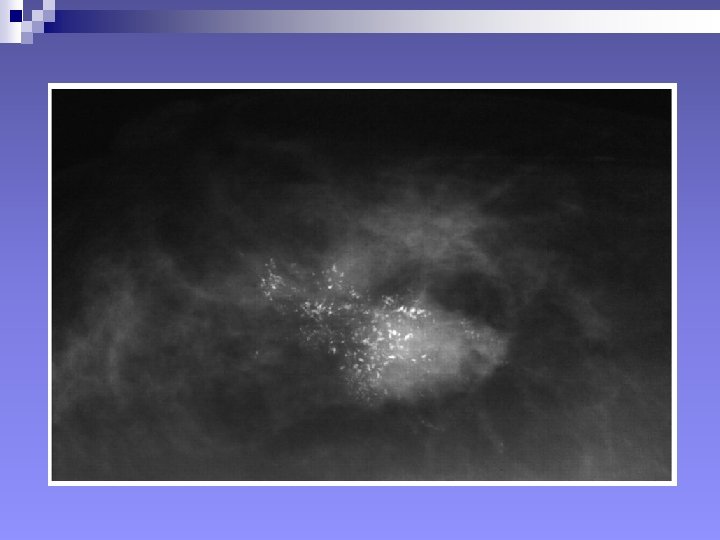
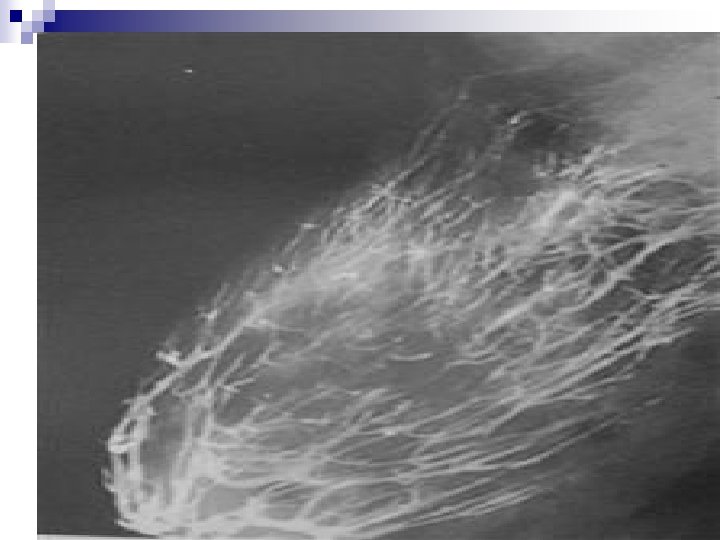
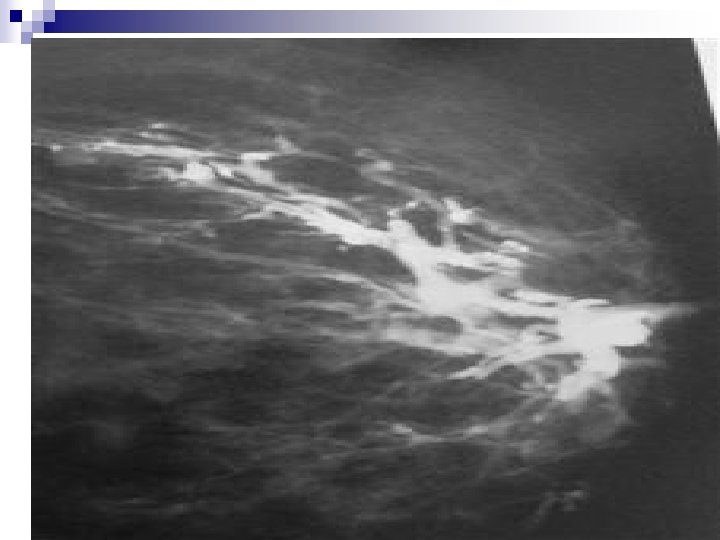
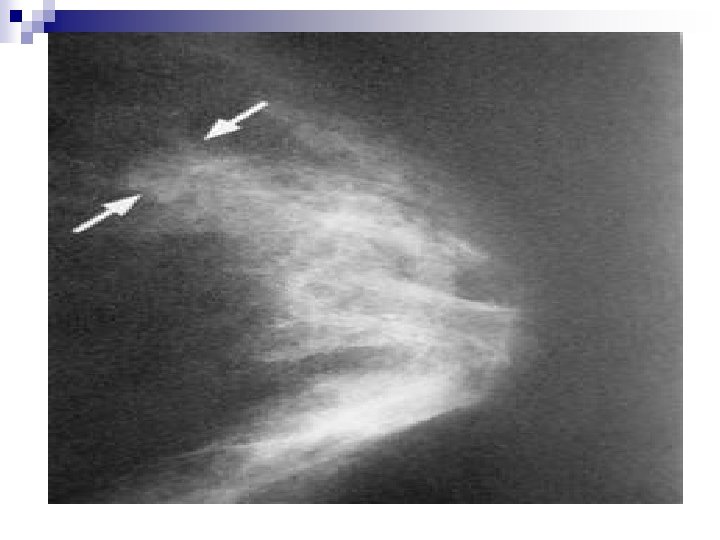
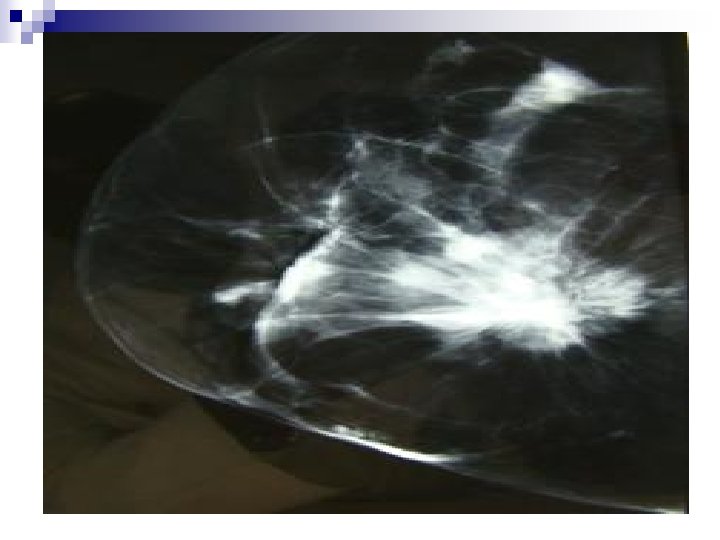
+++++++Mammography: SIGNS Mammary architecture: Preserved, Distorted n MASS: Size, Shape, Density (presence of fat), Margins, Microcalcifications. n n Shape: Round/Oval, Likely benign n Lobular, suspicious n Irregular, highly suspicious of malignancy n

+Signs in mammography, mass n Density: Quite fatty and low density, likely benign n Isodense, suspicious n High density, highly suspicious of malignancy. n n Margins: Well-defined, likely benign n Obscured/75%hidden or more, suspicious n Micrololulated, suspicious n Indistinct and ill-defined: suspicious and highly suspicious n Spiculated: Highly suspicious of malignancy n

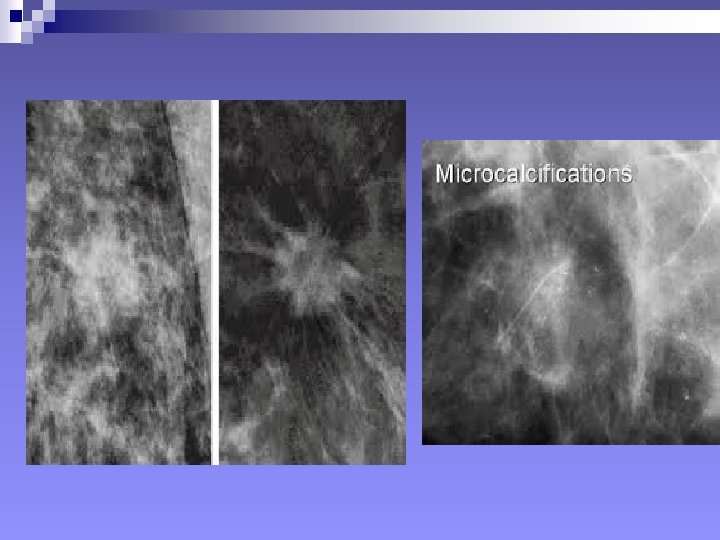
++Signs in mammography n Other signs: Fatty vs Glandular breast n Coarse Calcifications vs Microcalcifications n Skin thickness n Axillary adenopathy: size, number, configuration n Changes compared with previous mammograms n


H. OTHER IMAGING MODALITIES q GALACTOGRAPHY q Mammography after introduction of contrast medium into lactiferous ducts q Indicated for work-up of pathological discharge (spontaneous: clear serous, bloody, green. Not expressed under pressure) q Not indicated in galactorrhea q Contraindicated in presence of inflammation or known hypersensitivity to contrast medium

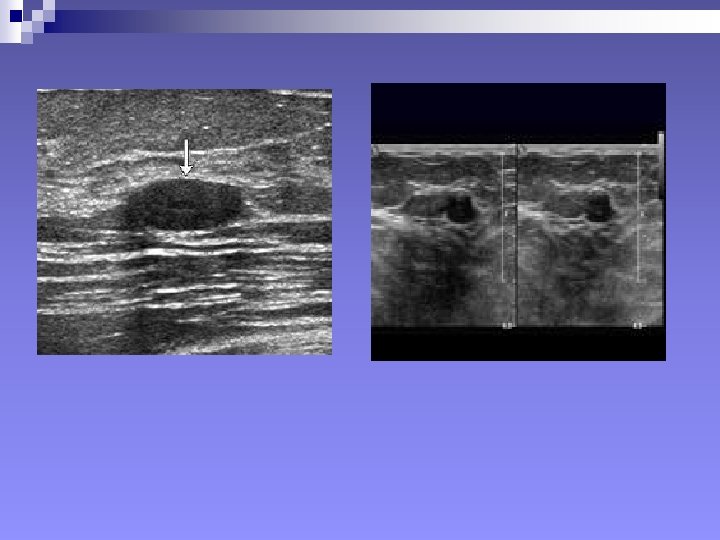
++Other Imaging Modalities. . . q SONOGRAPHY After mammography, ultrasound imaging is the second most important imaging modality for the breast. Major Roles q Diagnosis of cysts q Characterizing masses not fully assessed by mammography q Palpable masses obscured by dense tissues during mammography q Imaging guidance for percutaneous biopsy and localization q First imaging modality for young women ≤ 30 yrs.

+++Other Imaging Modalities. . . sonography Equipment: -Linear transducer, 7. 5 MHz or above -Tissue Harmonic Imaging software (THI) -Stand-off pad for better near-field view. Pitfalls: -Limited sensitivity in detection of small carcinomas -High false positive rate (recommendation for biopsy of lesions which are benign) -Inability to reliably image microcalcifications. N. B. Sonography is not a proven tool for breast-cancer screening

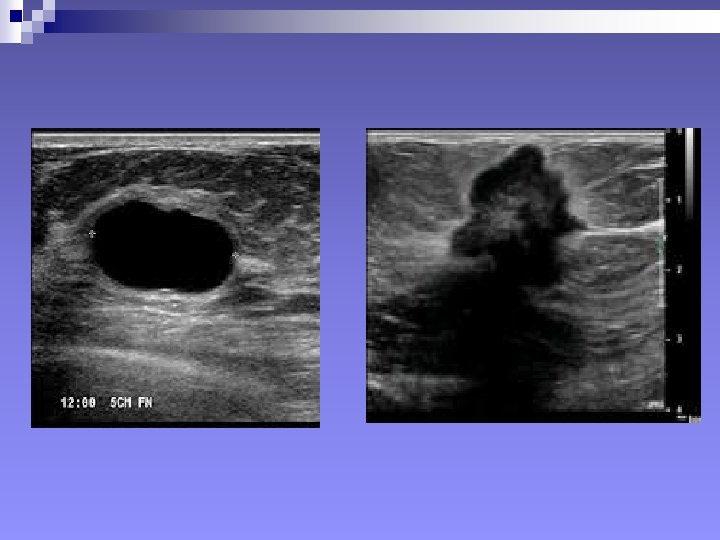
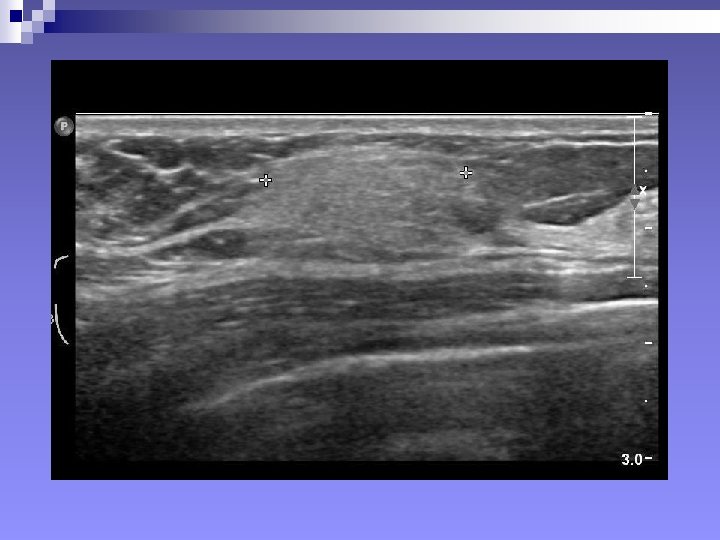
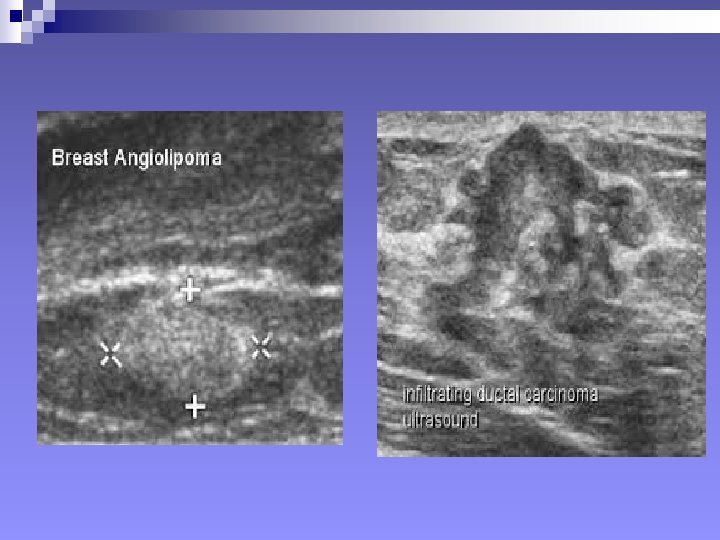
+Ultrasonography: SIGNS n Mass, Benign signs: ¨ Well-circumscribed ¨ More wide than deep ¨ Gently curving smooth lobulations ¨ Thin echogenic pseudocapsule (in a wider than deep nodule)
, when it contains")
++Signs in Ultrasonography “…A mass will considered malignant (until proven otherwise), when it contains any single malignant feature found on ultrasound…” n Mass, Malignant signs (Stavros et al 1995) ¨ Sonographic spiculation ¨ Deeper/taller than wide ¨ Microlobulations (small lobulations 1 -2 mm on the surface. Risk of malignancy rises with numbers) ¨ Thick hyper-echoic halo ¨ Angular margins ¨ Markedly hypo-echoic nodule ¨ Posterior acoustic shadowing Each of the above has positive predictive value of 70% or above.

+++Other Signs in ultrasonography Positive predictive value 30% or less n Mass, Malignant ¨ Branching pattern ¨ Punctate calcifications (do not shadow) ¨ Duct extension ¨ Heterogenous echo-texture ¨ Compressibility: Benign lesions compress with u/s pressure. Malignant lesions displace breast tissues without changing height



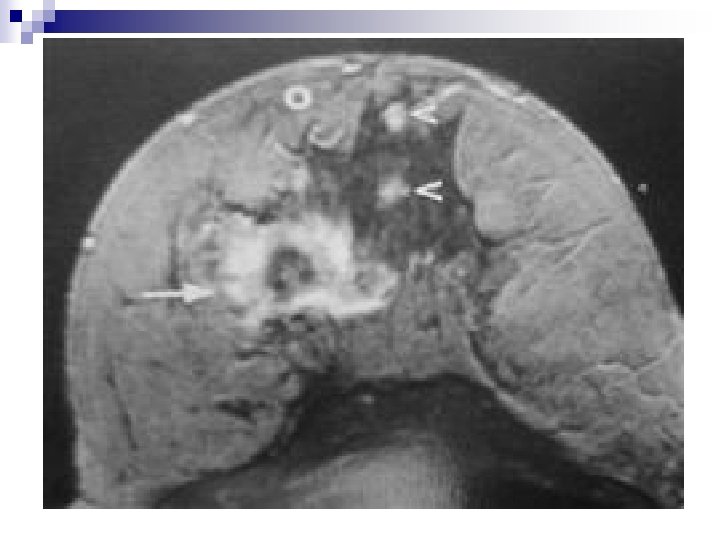
 Contrast-enhanced MRI")
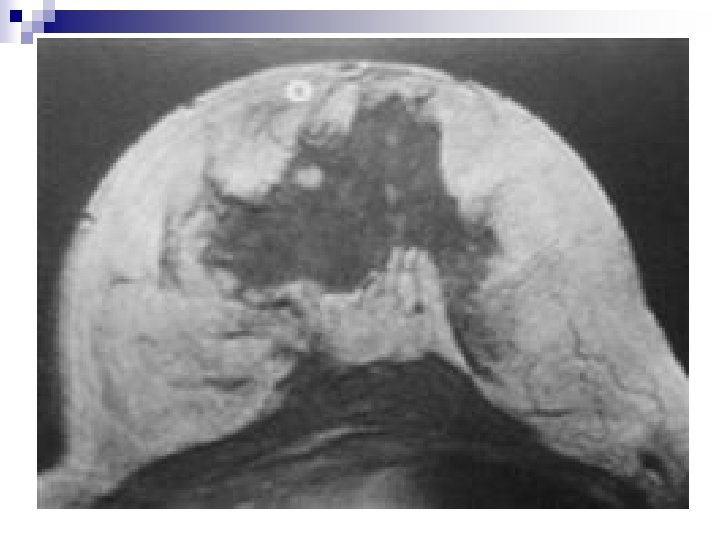
J. OTHER IMAGING MODALITIES. . . MRI q “NUCLEAR” MAGNETIC RESONANCE (MRI) Contrast-enhanced MRI is the most sensitive additional imaging modality supplementing mammography Equipment: -At least 0. 5 Tesla magnet -Dedicated breast coil -Slices ≤ 4 mm -Paramagnetic contrast medium , Gd-DTPA N. B. Using contrast-enhanced MRI as the sole imaging modality or interpreting contrast-enhanced MRI without mammography does not represent sound diagnostic practice

+++Other Imaging Modalities. . . q SCINTIMAMMOGRAPHY Imaging the breast following injection of a radiopharmaceutical, using Gamma camera or Rectilinear Scanner n Tc-99 m Sestamibi is a lipophilic compound, able to penetrate cells, then bound to cytosol and membranes of mitochondria. n Sestamibi accumulates preferentially in tumour cells n Sensitivity for palpable lesions: 83 – 97% n For lesions 1 cm, sensitivity is about 50% n Unreliable for Ca in situ.

++++Other Imaging Modalities. . . q POSITRON EMISSION TOMOGRAHY Breast imaging using compounds which produce single photon energy, of positron annihilation, as a tracer. n Fluoro-oestradiol (FES) is one such compound which is specific for oesrogen receptors expressed by some cancers. n Best for predicting response to anti-oestrogen, in patient with metastases. n Fluorodeoxyglucose (FDG) is another tracer, assesses response to cancer treatment. Sensitivity 90%

K. BI-RADS MAMMARY ASSESSMENT CATEGORIES 0. =Inconclusive 1. =Benign findings 2. =Negative 3. =Probably benign 4. =Suspicious abnormality 5. =Highly suggestive of malignancy 6. =Known biopsy, proven malignancy

RISK OF MALIGNANCY AND CARE PLAN BY BI-RADS SCREENING CATEGORY FINDINGS APPROXIMATE FOLLOW UP PROBALILITY RECOMMENDAOF TION MALIGNANCY 0 Evaluation incomplete. Needs additional Imaging 1 Negative 0 Mammogram at normal interval 2 Benign 0 -ditto- 3 Probably benign Less than 2% Shortened interval mammogram 4 Suspicious abnormalities Ranges from 3 – Consider biopsy 95%

+++RISK OF MALIGNANCY AND CARE PLAN BY BIRADS BI-RADS CATEGORY SCREENING FINDINGS APPROXIMATE PROBALILITY OF MALIGNANCY FOLLOW UP RECOMMENDATION 4 a Suspicious abnormalities 3 – 10% Biopsy 4 b -ditto- 10 – 50% Biopsy 4 c -ditto- 50 – 95% Biopsy 5 Highly suggestive of malignancy 95% or more Appropriate confirmation and staging procedures 6 Malignancy proven 100% Staging procedures and therapies

THANK YOU
- Slides: 79