Disinfection and Sterilization Issues and Controversies William A








 Hydrogen peroxide-HP (7. 5%) Peracetic")












 New Contraindications for OPA l l l Repeated exposure to OPA, following")













 l l Advantages n Very effective at killing microorganisms n Penetrates")

, linens and liquids cannot be")





")



 and continue")













: Disinfection and Sterilization Copyright © 2004 WA Rutala")

 u. No agent-specific nucleic acid")
 n Neurosurgical")











 in removing and/or")



- Slides: 82
Disinfection and Sterilization: Issues and Controversies William A. Rutala, Ph. D. , M. P. H. University of North Carolina (UNC) Health Care System and UNC at Chapel Hill, NC Copyright © 2004 WA Rutala
Disinfection and Sterilization: Issues and Controversies l Methods in Disinfection n Endoscopes/AERs, endocavitary probes, emerging pathogens l Methods in Sterilization n CJD l Issues and Controversies n Surface disinfection, CJD, glutaraldehyde exposure time (45 m/25 o. C vs 20 m/20 o. C), Copyright © 2004 WA Rutala endoscope rinse water
Disinfection and Sterilization in Healthcare Facilities WA Rutala, DJ Weber, and HICPAC, In press l Overview n Last CDC guideline in 1985 n 219 pages (>130 pages preamble, 20 pages recommendations, glossary of terms, tables, >900 references) n Evidence-based guideline (search of the literature using Medline) Copyright © 2004 WA Rutala
Efficacy of Disinfection/Sterilization Influencing Factors Cleaning of the object Organic and inorganic load present Type and level of microbial contamination Concentration of and exposure time to disinfectant/sterilant Nature of the object Temperature and relative humidity Copyright © 2004 WA Rutala
Decreasing Order of Resistance of Microorganisms to Disinfectants/Sterilants Prions Spores Mycobacteria Non-Enveloped Viruses Fungi Bacteria Enveloped Viruses Copyright © 2004 WA Rutala
Disinfection and Sterilization EH Spaulding believed that how an object will be disinfected depended on the object’s intended use. CRITICAL - objects which enter normally sterile tissue or the vascular system or through which blood flows should be sterile. SEMICRITICAL - objects that touch mucous membranes or skin that is not intact require a disinfection process (high-level disinfection[HLD]) that kills all microorganisms but high numbers of bacterial spores. NONCRITICAL -objects that touch only intact skin require low-level disinfection. Copyright © 2004 WA Rutala
Processing “Critical” Patient Care Objects Classification: Critical objects enter normally sterile tissue or vascular system, or through which blood flows. Object: Sterility. Level germicidal action: Kill all microorganisms, including bacterial spores. Examples: Surgical instruments and devices; cardiac catheters; implants; etc. Method: Steam, gas, hydrogen peroxide plasma or chemical sterilization. Copyright © 2004 WA Rutala
Critical Objects l Surgical instruments l Cardiac catheters l Implants Copyright © 2004 WA Rutala
Chemical Sterilization of “Critical Objects” Glutaraldehyde (> 2. 0%) Hydrogen peroxide-HP (7. 5%) Peracetic acid-PA (0. 2%) HP (1. 0%) and PA (0. 08%) HP (7. 5%) and PA (0. 23%) Glut (1. 12%) and Phenol/phenate (1. 93%) _______________________ __ Exposure time per manufacturers’ recommendations. Copyright © 2004 WA Rutala
Copyright © 2004 WA Rutala
Processing “Semicritical” Patient Care Objects Classification: Semicritical objects come in contact with mucous membranes or skin that is not intact. Object: Free of all microorganisms except high numbers of bacterial spores. Level germicidal action: Kills all microorganisms except high numbers of bacterial spores. Examples: Respiratory therapy and anesthesia equipment, GI endoscopes, thermometer, etc. Method: High-level disinfection Copyright © 2004 WA Rutala
Semicritical Items l Endoscopes l Respiratory therapy equipment l Anesthesia equipment l Endocavitary probes l Tonometers l Diaphragm fitting rings Copyright © 2004 WA Rutala
High Level Disinfection of “Semicritical Objects” Exposure Time > 12 m-30 m, 20 o. C Germicide Concentration_____ Glutaraldehyde Ortho-phthalaldehyde (12 m) Hydrogen peroxide* Hydrogen peroxide and peracetic acid* 1. 0%/0. 08% Hydrogen peroxide and peracetic acid* 7. 5%/0. 23% Hypochorite (free chlorine)* ppm > 2. 0% 0. 55% 7. 5% 650 -675 Copyright © 2004 WA Rutala
Processing “Noncritical” Patient Care Objects Classification: Noncritical objects will not come in contact with mucous membranes or skin that is not intact. Object: Can be expected to be contaminated with some microorganisms. Level germicidal action: Kill vegetative bacteria, fungi and lipid viruses. Examples: Bedpans; crutches; bed rails; EKG leads; bedside tables; walls, floors and furniture. Method: Low-level disinfection Copyright © 2004 WA Rutala
Low-Level Disinfection for “Noncritical” Objects Exposure time > 1 min Germicide Use Concentration Ethyl or isopropyl alcohol 70 -90% Chlorine 100 ppm (1: 500 dilution) Phenolic UD Iodophor UD Quaternary ammonium UD ___________________ UD=Manufacturer’s recommended use dilution Copyright © 2004 WA Rutala
Disinfectants for Surface Disinfection Controversy l Noncritical Surfaces n Medical equipment surfaces (BP cuff, stethoscopes) u. May frequently become contaminated with patient material u. Repeatedly touched by health care personnel u. Disinfectant/detergent should be used n Housekeeping surfaces (bed rails, bedside tables) u. May play a theoretical but less significant role in diseases transmission u. Disinfectants/detergents may be used (II) and detergents (non-patient care areas) Copyright © 2004 WA Rutala
New Methods in Disinfection Copyright © 2004 WA Rutala
New FDA-Cleared Sterilants l “Old” n l New n n n l > 2% Glut, 7. 5% HP, 1. 0% HP and 0. 08% PA 1. 21% glut and 1. 93% phenol/phenate (HLD-20 m at 25 o. C) 0. 55% ortho-phthalaldehyde (HLD-12 m) 7. 35% HP and 0. 23% PA (HLD-15 m) 2. 5% Glut (HLD-5 m at 35 o. C) Hypochlorite (650 -675 ppm free chlorine) Ensure antimicrobial activity and material compatibility Copyright © 2004 WA Rutala
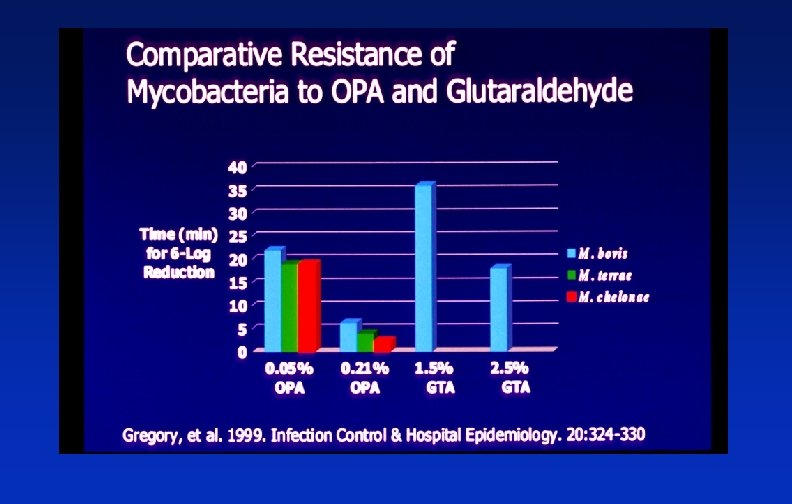
Glutaraldehyde l l Advantages n Numerous use studies published n Relatively inexpensive n Excellent materials compatibility Disadvantages n Respiratory irritation from vapor n Pungent and irritating odor n Relatively slow mycobactericidal activity n Coagulate blood and fix tissues to surfaces n Allergic contact dermatitis Copyright © 2004 WA Rutala
Ortho-phthalaldehyde Advantages Disadvantages l Fast acting HLD l Stains protein gray l No activation l Cost ($30/gal); but lower reprocessing costs-soak l Excellent materials time, devices per gal) compatibility l Slow sporicidal activity l Not a known irritant to eyes and nasal passages l Eye irritation with contact l Weak odor Copyright © 2004 WA Rutala
Comparison of Glutaraldehyde and OPA >2. 0% Glutaraldehyde l HLD: 45 min at 25 o. C l Needs activator l 14 day use life l 2 year shelf life l ACGIH ceiling limit, 0. 05 ppm l Strong odor l MEC, 1. 5% l Cost - $10/gallon 0. 55% Orthophthalaldehyde l HLD: 12 min at 20 o. C l No activator needed l 14 day use life l 2 year shelf life l No ACGIH or OSHA limit l Weak odor l MEC, 0. 3% l Cost - $30/gallon Copyright © 2004 WA Rutala
Ortho-phthalaldehyde (OPA) New Contraindications for OPA l l l Repeated exposure to OPA, following manual reprocessing of urological instruments, may have resulted in hypersensitivity in some patients with a history of bladder cancer undergoing repeated cystoscopy. Out of approximately 1 million urological procedures, there have been reports of 24 patients who have experience ‘anaphylaxis-like’ reactions after repeated cystoscopy (typically after 4 -9 treatments). Risk control measures: residues of OPA minimized; and contraindicated for reprocessing of urological Copyright © 2004 WA Rutala instruments used on patients with history of bladder
Disinfection and Sterilization of Emerging Pathogens Copyright © 2004 WA Rutala
Disinfection and Sterilization of Emerging Pathogens Hepatitis C virus l Clostridium difficile l Cryptosporidium l Helicobacter pylori l E. coli 0157: H 7 l Antibiotic-resistant microbes (MDR-TB, VRE, MRSA) l SARS Coronavirus Copyright © 2004 WA Rutala l Bioterrorism agents (anthrax, plague, smallpox) l
Disinfection and Sterilization of Emerging Pathogens Standard disinfection and sterilization procedures for patient care equipment are adequate to sterilize or disinfect instruments or devices contaminated with blood and other body fluids from persons infected with emerging pathogens Copyright © 2004 WA Rutala
Endoscopes/AERS Copyright © 2004 WA Rutala
TRANSMISSION OF INFECTION l Gastrointestinal endoscopy >300 infections transmitted n 70% agents Salmonella sp. and P. aeruginosa n Clinical spectrum ranged from colonization to death (~4%) n l Bronchoscopy 90 infections transmitted n M. tuberculosis, atypical Mycobacteria, P. aeruginosa Copyright © 2004 WA Rutala n
Copyright © 2004 WA Rutala
ENDOSCOPE DISINFECTION l l CLEAN-mechanically cleaned with water and enzymatic cleaner HLD/STERILIZE-immerse scope and perfuse HLD/sterilant through all channels for at least 12 min RINSE-scope and channels rinsed with sterile water, filtered water, or tap water followed by alcohol DRY-use forced air to dry insertion tube and Copyright © 2004 WA Rutala channels
Rinse Water for HLD Endoscopes-After HLD, rinse endoscopes and flush channels with sterile water, filtered water, or tapwater followed by a rinse with 70 -90% ethyl or isopropyl alcohol l Other Semicritical Devices-After HLD, use sterile water, filtered water, or tapwater followed by an alcohol rinse for devices that contact upper respiratory tract (II). l n No recommendation for sterile or filtered water Copyright © 2004 WA Rutala
Endocavitary Probes-Transesophageal echocardiography probes, vaginal/rectal probes used in sonographic scanning l Probes with contact with mucous membranes are semicritical l Guideline recommends that a new condom/probe cover should be used to cover the probe for each patient and since covers Copyright © 2004 WA Rutala may fail (1 -80%), HLD (semicritical probes) l
New Methods in Sterilization Copyright © 2004 WA Rutala
Sterilization The complete elimination or destruction of all forms of microbial life and is accomplished in healthcare facilities by either physical or chemical processes Copyright © 2004 WA Rutala
Steam Sterilization l l Advantages n Non-toxic n Cycle easy to control and monitor n Inexpensive n Rapidly microbicidal n Least affected by organic/inorganic soils n Rapid cycle time n Penetrates medical packing, device lumens Disadvantages n Deleterious for heat labile instruments n Potential for burns Copyright © 2004 WA Rutala
New Trends in Sterilization of Patient Equipment Alternatives to ETO-CFC ETO-CO 2, ETO-HCFC, 100% ETO l New Low Temperature Sterilization Technology Hydrogen Peroxide Gas Plasma Peracetic Acid l Copyright © 2004 WA Rutala
Ethylene Oxide (ETO) l l Advantages n Very effective at killing microorganisms n Penetrates medical packaging and many plastics n Compatible with most medical materials n Cycle easy to control and monitor Disadvantages n Some states (CA, NY, TX) require ETO emission reduction of 90 -99. 9% n CFC (inert gas that eliminates explosion hazard) banned after 1995 n Potential hazard to patients and staff n Lengthy cycle/aeration time Copyright © 2004 WA Rutala
Hydrogen Peroxide Gas Plasma Sterilization Advantages l Safe for the environment and health care worker; it leaves no toxic residuals l Fast - cycle time is 45 -73 min and no aeration necessary l Used for heat and moisture sensitive items since process temperature 50 o. C l Simple to operate, install, and monitor l Compatible with most medical devices Copyright © 2004 WA Rutala
Hydrogen Peroxide Gas Plasma Sterilization Disadvantages l Cellulose (paper), linens and liquids cannot be processed l Sterilization chamber is small, about 3. 5 ft 3 to 7. 3 ft 3 l Endoscopes or medical devices restrictions based on lumen internal diameter and length (see manufacturer’s recommendations) l Requires synthetic packaging (polypropylene) Copyright © 2004 WA Rutala and special container tray
Conclusions All sterilization processes effective in killing spores l Cleaning removes salts and proteins and must precede sterilization l Failure to clean or ensure exposure of microorganisms to sterilant (e. g. connectors) could affect effectiveness of sterilization process l Copyright © 2004 WA Rutala
Recommendations Methods of Sterilization Steam is preferred for critical items not damaged by heat l Follow the operating parameters recommended by the manufacturer l Use low temperature sterilization technologies for reprocessing critical items damaged by heat l Use immediately critical items that have been sterilized by peracetic acid immersion process Copyright © 2004 WA Rutala (no long term storage) l
Sterilization Practices Copyright © 2004 WA Rutala
Sterilization Monitoring Sterilization monitored routinely by combination of mechanical, chemical, and biological parameters l Physical - cycle time, temperature, pressure l Chemical - heat or chemical sensitive inks that change color when germicidal-related parameters present l Biological - Bacillus spores that directly Copyright © 2004 WA Rutala measure sterilization
Biological Monitors Steam - Geobacillus stearothermophilus l Dry heat - B. atrophaeus (formerly B. subtilis) l ETO - B. atrophaeus l New low temperature sterilization technologies Plasma sterilization (Sterrad) - G. stearothermophilus Peracetic acid - G. stearothermophilus l Copyright © 2004 WA Rutala
Recommendations Monitoring of Sterilizers Monitor each load with mechanical and chemical (internal and external) indicators. l Use biological indicators to monitor effectiveness of sterilizers at least weekly with spores intended for the type of sterilizer. l Use biological indicators for every load containing implantable items l Copyright © 2004 WA Rutala
Recommendations Storage of Sterile Items Sterile storage area should be well-ventilated area that provides protection against dust, moisture, and temperature and humidity extremes. l Sterile items should be stored so that packaging is not compromised l Sterilized items should be labeled with a load number that indicates the sterilizer used, the Copyright © 2004 WA Rutala cycle or load number, the date of sterilization, l
Reuse of Single Use Devices Copyright © 2004 WA Rutala
FDA Developments August 2000, FDA issued final SUD Enforcement Guidance. Hospitals and TPR regulated the same as original equipment manufacturer (OEM). l A device labeled for single-use only that is reprocessed is considered as a new device. Hospital is considered the manufacturer. l As a new device, all federal controls Copyright © 2004 WA regarding the manufacture and marketing of. Rutala l
Hospital’s Options: USA Option 1 -Comply with enforcement guidance (August 14, 2000) and continue to reprocess SUDs l Option 2 -Use Third Party Reprocessor (premarket requirements new for TPR as they have been using non-premarket requirements) l Option 3 -avoid reuse of SUDs l Copyright © 2004 WA Rutala
Recommendations Quality Control Provide comprehensive and intensive training for all staff assigned to reprocess medical/surgical instruments l To achieve and maintain competency, staff should: l hands-on training n all work supervised until competency is documented n competency testing should be conducted at commencement of employment and regularly Copyright © 2004 WA Rutala n
Disinfection and Sterilization: Issues and Controversies l Methods in Disinfection n Endoscopes/AERs, endocavitary probes, emerging pathogens l Methods in Sterilization n CJD l Issues and Controversies n Surface disinfection, CJD, glutaraldehyde exposure time (45 m/25 o. C vs 20 m/20 o. C), Copyright © 2004 WA Rutala endoscope rinse water
Issue/Controversy Detergents or Disinfectants for Surface Disinfection? Copyright © 2004 WA Rutala
Detergents or Disinfectants for Environmental Cleaning l Introduction n Use of noncritical items or contact with noncritical surfaces carries little risk of transmitting pathogens to patients Thus, the routine use of disinfectants to disinfect hospital floors and other surfaces (e. g. , bedside tables) is controversial However, while noncritical surfaces have not been directly implicated in disease transmission, they may potentially contribute to cross-transmission by acquisition of transient hand carriage by HCW due to contact with a contaminated surface, or patient contact with contaminated surfaces or medical equipment Copyright © 2004 WA Rutala
Detergents or Disinfectants for Environmental Cleaning l Noncritical Surfaces n Housekeeping surfaces (floors, walls, bedside tables) u. May play a theoretical but less significant role in diseases transmission u. Disinfectants/detergents or detergents may be used n Medical equipment surfaces (BP cuff, stethoscopes) u. May frequently become contaminated with patient material u. Repeatedly touched by health care personnel u. Disinfectant/detergent may be used Copyright © 2004 WA Rutala
Detergents or Disinfectants for Surface Disinfection l Justification for Using a Detergent on Floors Surfaces minor contribution to endemic HAIs n No difference in HAI rates when floors cleaned with detergent n No disinfectant disposal issues n No occupational exposures issues n Costs n Use of disinfectants could select for antibioticresistant bacteria Copyright © 2004 WA Rutala n
HAIs: Disinfectants vs Detergents l Dharan et al, 1999 n l Danforth et al, 1987 n l No change in incidence of HAIs during 4 mo trial compared to preceding 12 mo; but detergents associated with increase in bacterial counts. NI rate did not differ between disinfectant (8. 0/100 patients) and detergent (7. 1/100 patients); 8 acute care units; 3 mo periods; phenol. Daschner et al, 1980 No difference in NI rate in ICU over 6 mo (15. 6% vs 15. 5%). Comment: Studies are small, short duration and suffer from low statistical power since the outcome (HAI) is one of low frequency. Copyright © 2004 WA Rutala Requirement for reducing HAI stringent, not met by most n
Surface Disinfection: Should We Do It? l Justification for Using a Disinfectant n n n Surfaces may contribute to transmission of epidemiologically important microbes (e. g. , VRE, MRSA, C. difficile) Needed for surfaces contaminated by blood and OPIM Disinfectants are more effective in reducing microbial load Detergents become contaminated and result in seeding the patients environment with bacteria CDC recommends disinfection of noncritical equipment and surfaces for patients on isolation precautions One product for decontamination of noncritical surfaces (that is, floors and equipment) Copyright © 2004 WA Rutala
Microbial Contamination of Mop Water Copyright © 2004 WA Rutala
Cleaning and Disinfection of Floors Copyright © 2004 WA Rutala
Surfaces in the Spread of Infections l In experimental settings, treatment of surfaces with germicide has been found to interrupt transmission n n l Prevention of surface-to-human rotavirus transmission by treatment with disinfectant spray (J Clin Microbiol 1991; 29: 1991) Interrupts transfer of rhinovirus from environmental surfaces to hands (Appl Environ Microbiol 1993; 59: 1579) Studies demonstrating reduced transmission with improved disinfection n n Marked reduction in C. difficile-associated diarrhea rates in BMTU during bleach use Aggressive environmental disinfection credited with eradicating VRE Copyright © 2004 WA Rutala from Burn Center
Detergents or Disinfectants for Surface Disinfection Process noncritical patient-care equipment with a EPA-registered disinfectant or disinfectant/detergent at the proper use dilution and a contact time of at least 1 min. l Use disinfectant for housekeeping purposes when uncertain if cleaning personnel not able to: distinguish soiled areas containing blood from dirt; or determine when MDROs are likely in the environment. Copyright © 2004 WA Rutala l
Issue/Controversy Recommendations for reprocessing CJD contaminated instruments based on WHO consensus or science-based? Copyright © 2004 WA Rutala
Creutzfeldt Jakob Disease (CJD): Disinfection and Sterilization Copyright © 2004 WA Rutala
CJD Copyright © 2004 WA Rutala
Prion Diseases l Etiology n Prions (proteinaceous infectious agent) u. No agent-specific nucleic acid u. Host protein (Pr. Pc) converts to pathologic isoform (Pr. Psc); Pr. P gene resides on chromosome 20 u. Mutation in this gene may trigger transformation u. Accumulates in neural cells, disrupts function, cell death u. Resistant to conventional D/S procedures Copyright © 2004 WA Rutala
Iatrogenic Transmission of CJD Contaminated medical instruments n Electrodes in brain (2) n Neurosurgical instruments in brain (4? ) l Implantation of contaminated grafts l Dura mater grafts (114) n Corneal grafts (2) n l Use of human growth hormone (139) and gonadotropin (4) Copyright © 2004 WA Rutala
CJD and Medical Devices Six cases of CJD associated with medical devices n 2 confirmed cases-depth electrodes; reprocessed by benzene, alcohol and formaldehyde vapor n 4 cases-CJD following brain surgery, index CJD identified-1, suspect neurosurgical instruments l Cases occurred before 1980 in Europe Copyright © 2004 WA Rutala l
CJD : potential for secondary spread through contaminated surgical instruments
CJD and Medical Devices l World Health Organization, 2000 When instruments contact high infectivity tissue, single-use instruments recommended. n If single-use instruments not available, maximum safety attained by destruction of re-usable instruments. n Where destruction is not practical, reusable instruments must be decontaminated by immerse in 1 N Na. OH and autoclaved (121 o. C/30 m), cleaned, rinsed and steam sterilized. Copyright © 2004 WA Rutala n After decontamination by steam and Na. OH, n
CJD: Recommendations for Disinfection and Sterilization High risk patient, high risk tissue, critical/semicritical device-special prion reprocessing l High risk patient, low/no risk tissue, critical/semicritical device-conventional D/S or special prion reprocessing l Low risk patient, high risk tissue, critical/semicritical device-conventional D/S Copyright © 2004 WA Rutala l High risk patient, high risk tissue, noncritical l
CJD: Disinfection and Sterilization Conclusions l Critical/SC-cleaning with special prion reprocessing Na. OH and steam sterilization (e. g. , 1 N Na. OH 1 h, 121 o. C 30 m) n 134 o. C for 18 m (prevacuum) n 132 o. C for 60 m (gravity) n No low temperature sterilization technology effective Copyright © 2004 WA Rutala l Noncritical-four disinfectants (e. g. , chlorine) l
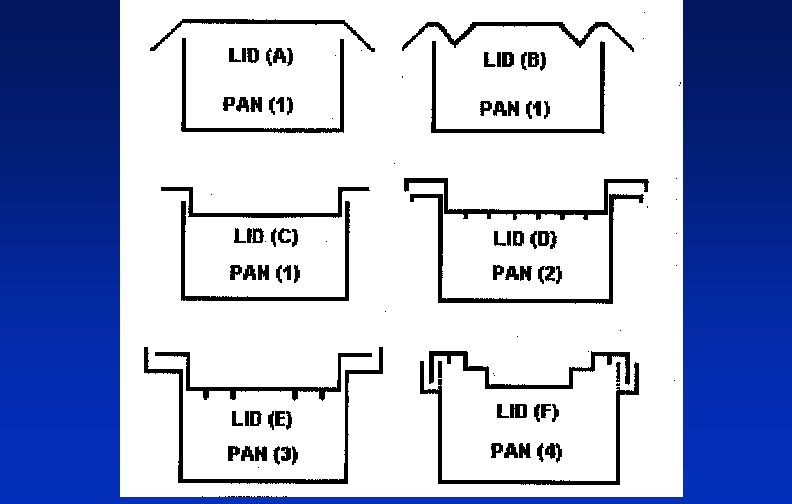
CJD: Instrument Reprocessing l Special prion reprocessing by combination of Na. OH and steam sterilization n n l l Immerse in 1 N Na. OH for 1 hour; remove and rinse in water, then transfer to an open pan and autoclave for 1 hour Immerse in 1 N Na. OH for 1 hour and heat in a gravity displacement sterilizer at 121 o. C for 30 minutes Combined use of autoclaving in sodium hydroxide has raised concerns of possible damage to autoclaves, and hazards to operators due to the caustic vapors. Risk can be minimized by the use of polypropylene containment pans and lids. Copyright © 2004 WA Rutala
CJD: Instrument Reprocessing l l l Special prion reprocessing by combination of Na. OH and steam sterilization n Immerse in 1 N Na. OH for 1 hour; remove and rinse in water, then transfer to an open pan and autoclave for 1 hour n Immerse in 1 N Na. OH for 1 hour and heat in a gravity displacement sterilizer at 121 o. C for 30 minutes Combined use of autoclaving in sodium hydroxide has raised concerns of possible damage to autoclaves, and hazards to operators due to the caustic fumes. Risk can be minimized by the use of polypropylene containment pans and lids (AJIC 2003; 31: 257 -60). Copyright © 2004 WA Rutala
Issue/Controversy “Science-based” guideline versus “policy-based” guideline Copyright © 2004 WA Rutala
“Science-based” or “Policy-based” Guideline Science-based-recommendations based of peer -reviewed scientific studies l Policy-based-recommendations based on EPA and FDA regulations and registration claims l High-level disinfection with glutaraldehyde for 20/20 (at least 33 studies support 20/20) vs 45/25; n Low-level disinfection for at least 30 -60 sec (at least 14 studies support 30 -60 sec) vs 10 min. Copyright © 2004 WA Rutala n
“Science-based” or “Policy-based” Guideline l l l FDA registration protocol does not allow cleaning Must kill 105 -106 Mtb, dried on scope, in presence of 2% horse serum, and in absence of cleaning. All professional organization guidelines, 10 -20 min glutaraldehyde When guidelines followed, no evidence of disease transmission Unresolved, but “science-based’ recommendation with recognition of FDA/EPA policies. Copyright © 2004 WA Rutala
BONUS Disinfection of Computer Keyboards Increased use of computers in patient areas has led to contamination of keyboards as reservoirs of pathogens l Study performed to l Examine the efficacy of different disinfectants on the computer keyboard n Determine if there were cosmetic (key lettering removed) or functional changes after 300 wipes n Copyright © 2004 WA Rutala
BONUS Disinfection of Computer Keyboards All tested products were effective (>95%) in removing and/or inactivating the test pathogens (MRSA, P. aeruginosa). No functional/cosmetic damage. l Disinfectants included: 3 quaternary ammonium compounds, 70% isopropyl alcohol, phenolic, chlorine (80 ppm) l At present, recommend that keyboards be © 2004 WA Rutala disinfected daily (for 5 sec) and when. Copyright visibly l
Disinfection and Sterilization: Issues and Controversies l Methods in Disinfection n Endoscopes/AERs, endocavitary probes, emerging pathogens l Methods in Sterilization n CJD l Issues and Controversies n Surface disinfection, CJD, glutaraldehyde exposure time (45 m/25 o. C vs 20 m/20 o. C), Copyright © 2004 WA Rutala endoscope rinse water
Thank you Copyright © 2004 WA Rutala
References Rutala WA, Weber DJ. CJD: Recommendations for disinfection and sterilization. Clin Inf Dis 2001; 32: 1348 l Rutala WA, Weber DJ. New disinfection and sterilization methods. Emerg Inf Dis 2001; 7: 348 l Rutala WA, Weber DJ, HICPAC. CDC guideline for disinfection and sterilization in healthcare facilities. In press. l Rutala WA. APIC guideline for selection and use Copyright © 2004 WA Rutala of disinfectants. Am J Infect Control 1996; 24: 313 l