NonSurgical Treatment By Dr Omar Alkaradsheh Treatment of

Non-Surgical Treatment By Dr. Omar Alkaradsheh

Treatment of periodontal disease

Outline �Non-surgical therapy � Rationale � Goals 1. 2. 3. 4. 5. 6. 7. � � Plaque control Scaling & root planing Antiinfective therapy Host modulation Occlusal evaluation and therapy Adjunctive role of orthodontic treatment Re-evaluation: Healing Results

Non-Surgical Therapy � Synonyms: � Phase I therapy � Initial therapy � Cause-related therapy � Etiotropic phase of therapy. � Refer to the procedures performed to treat gingival and periodontal infections, up to and including tissue reevaluation, which is the point at which the course of ongoing care is determined.

Rationale � Achieve: � comprehensive daily plaque control regimen � thorough removal of calculus and microbial plaque � correction of defective restorations � treatment of carious lesions � phase I therapy provides an opportunity for the dentist to evaluate tissue response and patient motivation about periodontal care, both of which are crucial elements to the overall success of treatment. � The long-term success of periodontal treatment depends predominantly on maintaining the results achieved with phase I therapy and much less on any specific surgical procedures.

Goals Ø Decrease the quantity of organisms below a critical mass and alter the composition of the remaining bacterial flora to one associated with health. Ø Reach an Equilibrium between the remaining bacterial plaque and host response. Ø halt the progression of disease. Ø Restore gingival and periodontal health.
 � Plaque control and patient education: � Daily plaque")
Nonsurgical Phase (Phase I Therapy) � Plaque control and patient education: � Daily plaque control regimen � Diet control (in patients with rampant caries) � Smoking cessation � Removal of plaque and calculus and local factors: � � � � Removal of calculus and root planing Correction of restorative and prosthetic irritational factors Excavation of caries and restoration (temporary or final) Antimicrobial therapy (local or systemic) Extraction of hopeless teeth Occlusal therapy Minor orthodontic movement Provisional splinting and prosthesis � Evaluation of response to nonsurgical Phase

� In many cases, phase I therapy will be the only set of procedures required to restore periodontal health

Non-Surgical Treatment 1. Education & Plaque Control 4. Treat/temporize carious lesions 2. Scaling & Root planing 5. Adjunctive aids 3. Remove local factors 6. Re-evaluation

Step. 1 Patient Education &Plaque Control

Step 1: Plaque Control Instruction �Plaque control is the essential component to successful periodontal therapy � Should begin in the first treatment appointment. � “Targeted oral hygiene” emphasizes thorough plaque removal around the periodontal tissues.

Rationale � The cause and effect relationship between supragingival plaque and gingivitis was demonstrated by Loe and his colleagues in 1965. � When plaque was allowed to accumulate, gingivitis developed within 21 days. When plaque control was initiated, the gingivitis was reversed (by means of efficient plaque control, i. e. , brushing and flossing) to clinical gingival health � The removal of microbial plaque leads to cessation of gingival inflammation, and cessation of plaque control measure leads to recurrence of inflammation

� The removal of plaque also decreased the rate of formation of calculus. ( Sanders , 1962) � Thus eliminating the plaque is the key to prevent the occurrence of periodontal disease or halting the progression of the disease. � Masses of plaque first develop in Molar , Premolar areas , followed by proximal surfaces of the anterior teeth , and the facial surfaces of the molar and premolar( Lang, 1973)

Plaque Control methods Mechanical Chemical

q Chemical Plaque Control � Antibiotics � enzymes � Metal ions � Fluorides � Natural products � Bisguanides antiseptics � Oxygenating agents � Amine Alchohols � Phenols and essential oils � Mouth rinse � Irrigation � Gel � Slow releasing device

Plaque Control Methods Mechanical methods Toothbrush • Manual • Powered Dentifrices Interdental Aids • dental floss • toothpick • interproximal brush Oral Irrigation supragingival subgingival

Irrigation q Work by directing a pulsating stream of water through a nozzle to the tooth surface v Supragingival Irrigation: � irrigators clean nonadherent bacteria and debris from the oral cavity more effectively than toothbrushes and mouth rinses. � They are particularly helpful for removing debris from inaccessible areas around orthodontic appliances and fixed prostheses. � When used as adjuncts to toothbrushing, these devices can have a beneficial effect on periodontal health by: � reducing the accumulation of microbial plaque and calculus � decreasing inflammation and pocket depth

Subgingival Irrigation � Home irrigation is performed by aiming or placing the irrigation tip into the periodontal pocket, attempting to insert the tip at least 3 mm, using a soft rubber, each pocket flushed for a few seconds. � Dental office: lavage or flushing of the periodontal pocket, as a one-time treatment after scaling and root planing, has not been shown to improve clinical healing, and data do not support its use in improving therapeutic results. � Used to deliver antimicrobial agents, mouthrinses into the periodontal pockets. � chlorhexidine diluted to one-third strength and performed regularly at home and after scaling, root planing, and in-office irrigation therapy has produced significant gingival improvement compared with controls. � Subgingival irrigation has been shown to disrupt more than half the subgingival plaque and reach about half the depth of pockets, up to 7 mm, much further apically than a toothbrush or floss can reach. � These data suggest that patients can benefit from daily subgingival irrigation, particularly in difficult sites such as furcations and residual pockets

Oral Irrigation � Pulsation creates two zones of hydrokinetic activity: the impact zone and the flushing zone.

Subgingival Irrigation

Recommendations �Supragingival irrigation reduces gingival inflammation and is easier for some patients than using mechanical interdental aids. �Subgingival irrigation with specialized tips for deep pockets and furcation areas is effective when used daily as part of the home care routine. �Patients requiring antibiotic premedication for dental procedures should use supragingival techniques.

Non-Surgical Treatment 1. Education & Plaque Control 4. Treat/temporize carious lesions 2. Supra & subgingival calculus removal 5. Adjunctive aids 3. Remove local factors 6. Re-evaluation

Step 2. Removal of Supragingival and Subgingival Calculus

Outline � Introduction, � Detection and removal of dental calculus, � Methods used for non-surgical root surface debridement � Scaling & root planing Ø Ø Ø Hand instrumentation Sonic and ultrasonic scalers, Side effects � Ablative laser therapy, � Photodynamic therapy � Evidence-based choice of debridement method � Outcome of S/RP: � Clinical and microbioligical � Implication of furcation involvement, � Healing following successful phase I therapy

q All periodontal treatment is based on successful initial NSPT. q S/RP is the most common used method to remove supra and subgingival calculus. q Periodontitis is strongly associated with the presence of dental calculus on root surfaces q The rough surface of calculus does not in itself induce inflammation but that the deleterious effect of calculus relates to its ability to provide an ideal surface for microbial colonization (Waerhaug 1952)

1 - visual examination. 2 - tactile exploration.

�Scaling is the process by which plaque and calculus are removed from both supragingval and subgingival tooth surfaces. �Root planning : The process by which residual embedded calculus and portion of cementum are removed from the roots to produce a smooth , hard and clean surface.

Rationale o Epithlelial adherence to subgingival calculus can occur following its disinfection with chlorhexidine (Lisgarten & Ellegaard 1973) Ø LPS were thought to be present within calculus and underlying cementum. For this reason it was thought necessary to remove not only calculus but also underlying cementum. However later evidence suggested that removal of tooth substance was not necessary. Ø On no occasion was LPS seen penetrating into sub-surface cementum (Hughes & Smales 1986) Ø Animal and human studies which demonstrated that removal of superficial plaque on subgingival calculus resulted in the healing of periodontal lesions and the maintenance of health, provided supragingival hygiene was meticulous (Nyman et al. 1986, 1988; Mombelli et al. 1995)

Rationale �Root debridement: removal of plaque and/or calculus from the root surface without the intentional removal of tooth structure. Claffey et al. 2004 �A rationale for the removal of calculus relates to eliminating, as far as possible, surface irregularities harbouring pathogenic bacteria.

Calculus Removal q. Factors that may influence calculus removal include : I. III. IV. The extent of disease, Anatomic factors, Skill of the operator, Instruments used.

Methods used for non-surgical root surface scaling and root planing/ debridement a. Hand Instruments c. Laser b. Powered Instruments d. Photodynamic therapy

�Access to the Root surface The root surface are not easy to access because Limitation of penetration of instruments. q. In subgingival access. scaling and root planing skills is needed. qin deep pockets. open procedure may be needed.

�Supra gingival scaling technique: Sickles , curettes , and ultrasonic and sonic instrument are most commonly used for removal of supragingival calculus. �Sub gingival scaling and Root planning technique: The curette is preferred by most clinicians because of the advantages afforded by its design.

Manual Instruments

Supragingival Scaling Sickle Hoe File

Principles Ø Subgingival instrumentation should preferably be performed under local anesthesia. Ø Modified pen grasp

Principles Ø Finger rest �As close as possible to the site of instrumentation �to facilitate controlled use of the instrument � Provides: (1) stable fulcrum, (2) permit optimal angulation of the blade, (3) enable the use of wrist–forearm motion.

Principles Ø The optimal angle between the cutting edge and the tooth is approximately 80º : � Too obtuse an angle, will result in cratering and consequent roughening of the root surface. � Too acute an angle, will result in ineffective removal and burnishing of subgingival calculus deposits.

Cutting position: The shank of the curette held parallel to the long axis of the tooth during instrumentation of a posterior site. Activation: ü The grasp of the instrument is tightened somewhat, the force between the cutting edge and the root surface is increased, and the blade is moved in a coronal direction. ü Strokes must be made in different directions to cover all aspects of the root surface (crosswise, back and forth) but, as stated above, strokes should always start from an apical position and be guided in a coronal direction.

Principles �Sharpening

Powered Instruments q Sonic scalers: § Use air pressure § The frequencies of vibration ranging from 2000– 6000 Hz.

Powered Instruments q Ultrasonic scalers: � convert electrical current to mechanical energy in the form of high-frequency vibrations at the instrument tip; � The vibration frequencies ranging from 18 000– 45 000 Hz. Ø Piezoelectric scalers � Alternating electrical current � Pattern of vibration is linear Ø Magnetostrictive scalers � Electrical current magnetic field in the handpiece the insert to vibrate. � The pattern of vibration at the tip is elliptical.

�Ultrasonic scaling: Ultrasonic instrument have been used as a valuable adjunct to conventional hand instrumentation . �Uses of Ultrasonic scaling devices : 1 - Scaling and gingival curettage. 2 -Removal of stains. 3 - Remove overhangs and excess cement

�Contraindications of ultrasonic scaling: q. Patient with cardiac pacemaker. q. Patients with Known communicable diseases. q. Chronic pulmonary problems. q. Porcelain bounded restoration. q. Patient with Titanium implant ( plastic-tipped ultrasonic and sonic insert and Teflon-coated sonic scaler tips are available)
")
�Meticulous and requires more experienced operator. �Time consuming(× 2 the time needed for surgery) �Less predictable in deep pockets , furcations and interproximal groove. �Ineffective as mono therapy in the treatment of aggressive periodontitis.

Ø Pain Ø Dentine hypersensitivity § The extent of the sensitivity can be diminished through good plaque removal. § Higher in pre-existing sensitivity, intensity decrease with time Ø Gingival recession v Warning patients about these potential outcomes at the beginning of the treatment sequence will avoid surprise if these changes occur. v Unexpected and possibly uncomfortable consequences to treatment may result in distrust and loss of motivation to continue therapy.

�From a clinical standpoint, minimizing the total volume of dental calculus present seems to be desirable. However, aggressive tooth substance removal does not seem warranted. (Claffey et al. 2004) �There was no difference between hand powered instrumentation in deposits removal and improved clinical parameters. (Badersten et al. 1981, loos et al. 1987, Laurell et al. 1988) �There was no difference between hand powered instruments in the treatment of class I furcation involved areas , while powered instruments were more effective than hand instruments in class II and III furcation due to smaller tip size (Matia et al. 1986 , Leon &Vogel 1987)

�Endotoxins are superficially attached to the root surface and can be removed by brushing (Moore et al. 1986), polishing (Nyman et al. 1988) or light overlapping strokes with ultrasonic scalers (smart et al. 1990) �The critical probing depth for scaling and root planing is 2. 9 mm ± 0. 4 and for periodontal surgery is 4. 2 mm ± 0. 2 (Lindhe et al. 1982 ) �Scaling and root planing did not result in total removal of subgingival calculus particularly in deep pockets ( Rabbani et al. 1981)

Ablative Laser therapy �Carbon dioxide lasers �Er: YAG lasers �Nd: YAG lasers

Ablative laser therapy q. Advantages: �It has bacteriocidal and detoxification effects. �Can remove the epithelium lining and granulation tissue within the periodontal pocket which may potentially improve healing. �Removing plaque and calculus with extremely low mechanical stress and no formation of a smear layer on root surfaces. �May allow access to sites that conventional mechanical instruments cannot reach.

Ablative Laser therapy q Carbon dioxide lasers o when used with relatively low energy output in a pulsed and/or defocused mode o have root conditioning, detoxification, and bacteriocidal effects on contaminated root surfaces. o However, at low energy outputs they are unable to remove calculus. q Er: YAG lasers o Are capable of effectively removing calculus from the root surface. o Energy is absorbed by water and organic components of the biological tissues which causes their evaporation resulting in heat generation, water vapour production, and thus an increase in internal pressure within the calculus deposits. The resulting expansion within the calculus causes its separation from the root surface

Er: YAG

Ablative laser therapy Ø Use of lasers produces results comparable to scaling and root planing. Ø Benefit of the use of lasers over scaling and root planing alone has been demonstrated. (Schwarz et al. 2003; Ambrosini et al. 2005) Ø Currently there is minimal evidence to support use of a laser for the purpose of subgingival debridement either as monotherapy or adjunt to S/RP.

q Precautions: �Inadvertent irradiation and reflection from shiny metal surfaces may cause damage to patient’s eyes, throat, and oral tissues other than the targeted area. �Risk of excessive tissue destruction by direct ablation and thermal side effects. �Also the high cost of the laser apparatus is a drawback for many
")
Photodynamic therapy (PDT)
, No. 1, Poster 587")
PDT principle Int Poster J Dent Oral Med 14 (2012), No. 1, Poster 587
 q Advantages: �PDT is non-invasive local therapy, �PDT offers thorough irrigation")
Photodynamic therapy (PDT) q Advantages: �PDT is non-invasive local therapy, �PDT offers thorough irrigation and elimination of pathogens in inaccessible areas of periodontal pocket within short span of time, thus beneficial to both operator and the patient. �The risk of bacteraemia after periodontal debridement can be minimized. �There is no need to prescribe antibiotics, therefore the possibility of side effects is avoided. �There is no need to anaesthetize the area and destruction of bacteria is achieved in a very short period (<, 60 seconds).
 �Antimicrobial photodynamic therapy acts as a beneficial adjunct to SRP in")
Photodynamic therapy (PDT) �Antimicrobial photodynamic therapy acts as a beneficial adjunct to SRP in non-surgical treatment and management of chronic periodontitis in short-term. �Further studies are required to assess the long-term effectiveness of a PDT. (Sgolastra et al. 2013, Betsy et al. 2014)

Choice of method used q In contrast to hand instrumentation, the use of sonic and ultrasonic scalers is less technique sensitive, requires less time to complete, and removes less root surface cementum. It has been shown to provide better access to deep pockets and furcation areas. (Kocher et al. 1998; Beuchat et al. 2001). q In addition the flushing action of water used in sonic and ultrasonic scalers removes, to a certain extent, debris and bacteria from the pocket area. However, tactile sensation is reduced, and there is production of contaminated aerosols (Harrel et al. 1998; Barnes et al. 1998; Rivera-Hidalgo et al. 1999; Timmerman et al. 2004). q Some patients may find the vibration, sound, and water spray uncomfortable.

Conclusions �Removal of calculus is accomplished using scalers, curettes, ultrasonic instrumentation, or combinations of these devices during one or more appointments. �Evidence suggests that the treatment results for chronic periodontitis are similar for all instruments, and some dentists now incorporate laser technology into periodontal therapy, including phase I therapy.

Non-Surgical Treatment 1. Education & Plaque Control 4. Treat/temporize carious lesions 2. Supra & subgingival calculus removal 5. Adjunctive aids 3. Remove local factors 6. Re-evaluation

Step 3. Recontouring Defective Restorations and Crowns § Corrections for restorative defects, which are plaque traps, may be made by smoothing surfaces and overhangs with burs or hand instruments or by replacing restorations. § These procedures can be completed concurrently with other phase I procedures.


EVA SYSTEM �Most efficient and least traumatic instruments for correcting overhangs or overcontoured proximal alloy or resin �These files are made of Aluminum in the shape of a wedge protruding from a shaft. �Reciprocating handpiece.

EVA system

Non-Surgical Treatment 1. Education & Plaque Control 4. Treat/temporize carious lesions 2. Supra & subgingival calculus removal 5. Adjunctive aids 3. Remove local factors 6. Re-evaluation

Step 4. Management of Carious Lesions �Removal of the carious tissue and placement with either temporary or permanent restorations is indicated in phase I therapy because of the infectious nature of the caries process. � Healing of the periodontal tissues will be maximized by removing the reservoir of bacteria in these lesions so that they cannot repopulate the microbial plaque.

Caries Control � Dental caries, particularly root caries, is a problem for periodontal patients because of attachment loss associated with the disease process and periodontal therapeutic procedures � Fluoride works primarily by topical effects to prevent and reverse the caries process, whether in enamel, cementum, or dentin. � Low concentrations of topical fluoride inhibit demineralization, enhance remineralization, and inhibit the enzyme activity in bacteria by acidifying the cells � All periodontal patients should be encouraged to use a fluoride-containing toothpaste daily, 1000 to 1100 ppm, to reduce demineralization and enhance remineralization of tooth surfaces. � Patients at high risk for caries, including those with a history of root lesions or who have active lesions, should use higher-concentration fluoride toothpaste or gels, 5000 ppm, daily until the risk for caries is controlled, then maintain with the lower concentration toothpastes and mouthrinses. � Other considerations in caries control, such as diet and reduced salivary flow, should be evaluated as with all dental patients.

Non-Surgical Treatment 1. Education & Plaque Control 4. Treat/temporize carious lesions 2. Supra & subgingival calculus removal 5. Adjunctive aids 3. Remove local factors 6. Re-evaluation

Adjunctive aids to scaling and root planing �Anti-infective therapy: systemic & local �Host modulation therapy �Orthodontic treatment

Anti-infective agents �An anti-infective agent is a chemotherapeutic agent that acts by reducing the number of bacteria present �Antibiotics, antimicrobials, antiseptics, disinfectants �Locally, orally or systemically

Systemic Antibiotics q An ideal antibiotic for use in prevention and treatment of periodontal diseases should be: I. specific for periodontal pathogens, II. allogenic and nontoxic, III. substantive, IV. not in general use for treatment of other diseases, V. inexpensive. q Currently, an ideal antibiotic for the treatment of periodontal diseases does not exist. q Although oral bacteria are susceptible to many antibiotics, no single antibiotic at concentrations achieved in body fluids inhibits all putative periodontal pathogens. q Indeed, a combination of antibiotics may be necessary to eliminate all putative pathogens from some periodontal pockets

Background and Rationale �The treatment of periodontal diseases is based on the infectious nature of these diseases. �Ideally, the causative microorganism(s) should be identified and the most effective agent should be selected using antibiotic-sensitivity tests. �Although this appears simple, the difficulty lies primarily in identifying specific etiologic microorganism(s) rather than microorganisms simply associated with various periodontal disorders.

Rationale �Systemic antibiotics aims to reinforce mechanical treatment and to support host defences in ovcercoming periodontal infections by killing subgingival pathogens remaining after periodontal instrumentation �Pathogens may escape the effect of mechanical debridement because of their ability to invade periodontal tissue, to reside in anatomical tooth structure inaccessable to instrumentation, or as a result of poor host defense ( position paper. J periodontol 2004; 75: 1553 -1565)
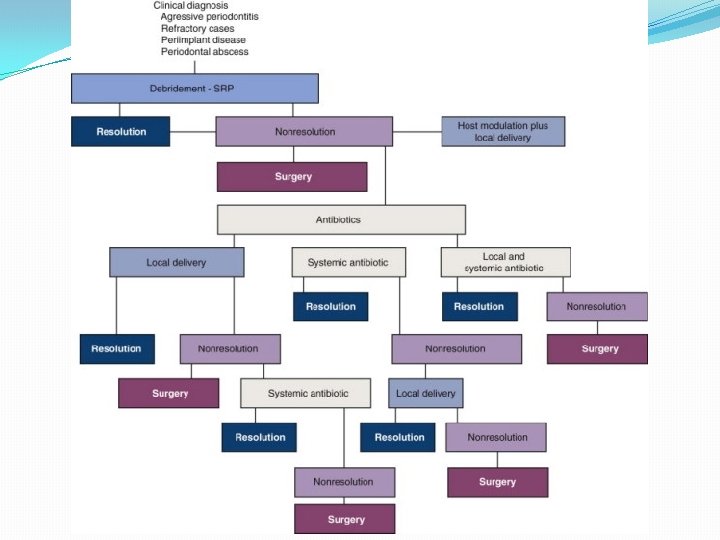

TABLE 47 -2 -- Common Antibiotic Regimens Used to Treat Periodontal Diseases* Systemic antibiotics Regimen Dosage/Duration Amoxicillin 500 mg Three times daily for 8 days Azithromycin 500 mg Once daily for 4– 7 days Ciprofloxacin 500 mg Twice daily for 8 days Clindamycin 300 mg Three times daily 10 days Doxycycline or minocycline 100– 200 mg Once daily for 21 days Metronidazole 500 mg Three times daily for 8 days 250 mg of each Three times daily for 8 days Single Agent Combination Therapy Metronidazole + amoxicillin Metronidazole + ciprofloxacin 500 mg of each Twice daily for 8 days

Locally delivered agents A. B. C. D. E. Subgingival Chlorhexidine Tetracycline-Containing Fibers Subgingival Doxycycline Subgingival Minocycline Subgingival Metronidazole

Tetracyclin- containing fibers
 containing")
Tetracyclin- containing fibers � An ethylene/vinyl acetate copolymer fiber (diameter, 0. 5 mm) containing tetracycline. � When packed into a periodontal pocket, it was well tolerated by oral tissues, and for 10 days it sustained tetracycline concentrations exceeding 1300 µg/ml, well beyond the 32 to 64 µg/ml required to inhibit the growth of pathogens isolated from periodontal pockets. � In contrast, GCF concentrations of only 4 to 8 µg/ml were reported after systemic tetracycline administration, 250 mg qid for 10 days. � tetracycline fibers applied with or without scaling and root planing reduced probing depth, bleeding on probing, and periodontal pathogens and provided gains in clinical attachment level. � Such effects were significantly better than those attained with scaling and root planing alone or with placebo fibers. � No change in antibiotic resistance to tetracycline was found after tetracycline fiber therapy among the tested putative periodontal pathogens. � However, these fibers are no longer commercially available.
 �Resistance? 10%")
Doxycyclin gel �A gel system using a syringe with 10% doxycycline (Atridox) �Resistance? 10% doxycycline (Atridox) gel.
 � It is applied in viscous consistency to the pocket, where")
Metronidazole (Elyzol 25%) � It is applied in viscous consistency to the pocket, where it is liquidized by the body heat and then hardens again, forming crystals in contact with water. As a precursor, the preparation contains metronidazolebenzoate, which is converted into the active substance by esterases in GCF. � Two 25% gel applications at a 1 -week interval have been used. � metronidazole gel is equivalent to scaling and root planing but have not shown adjunctive benefits with scaling and root planing.

Minocycline microspheres � The 2% minocycline is encapsulated into bioresorbable microspheres in a gel carrier. � Sustained release � This product is available in the US and a number of other countries. � When compared to controls (scaling and root planing with nonactive vehicle as subgingival irrigant), there was a statistically significant increase in clinical attachment levels in patients who presented with pockets of 6 mm or greater probing depth minocycline microspheres (Arestin).

Chlorhexidine chip � Perio. Chip is a small chip (4. 0 × 5. 0 × 0. 35 mm) composed of a biodegradable hydrolyzed gelatin matrix. � 2. 5 mg CHX incorporated � This delivery system releases chlorhexidine and maintains drug concentrations in the GCF greater than 100 µg/ml for at least 7 days, concentrations well above the tolerance of most oral bacteria. � Because the chip biodegrades in 7 to 10 days, a second appointment for removal is not needed chlorhexidine gluconate chip (Perio. Chip)

Local Delivery Agents � Adjuncts to scaling and root planing � A recent systematic review concluded “adjunctive local therapy generally reduced probing depth levels. Differences between treatment and SRP-only groups in the baseline to follow up period typically favored treatment groups but usually only modestly (e. g. , from about 0. 1 mm to nearly 0. 5 mm). Effects for clinical attachment level gains were smaller (Bonito 2005) � American Academy of Periodontology stated: ü “the clinician's decision to use locally delivered agents (LDA) should be based upon a consideration of clinical findings, the patient's dental and medical history, scientific evidence, patient preferences and advantages and disadvantages of alternative therapies. ” ü The report also stated that use of LDAs may be of value when probing depths greater than 5 mm with inflammation are still present after conventional therapy. However if multiple sites are present in the same quadrant, therapy other than LDAs should be considered.

Adjunctive aids to scaling and root planing �Anti-infective therapy: systemic & local �Host modulation therapy �Orthodontic treatment
 q“there are compelling data from studies in animals and human")
Host Modulation Therapy (HMT) q“there are compelling data from studies in animals and human trials indicating that pharmacologic agents that modulate the host responses believed to be involved in the pathogenesis of periodontal destruction may be efficacious in slowing the progression of periodontitis” q Locally (Topical NSAIDs) or systemically applied (NSAIDs, Bisphonates, Subantimicrobial dose doxycyclin)

Host modulation and comprehensive periodontal management

Rationale
 � SDD is currently the only FDA-approved (Periostat) , systemically")
Sub-Antimicrobial dose. Doxycycline (SDD) � SDD is currently the only FDA-approved (Periostat) , systemically administered HMT indicated specifically in the treatment of periodontitis. � MOA: in addition to its antibiotic properties, doxycycline has the ability to downregulate MMPs, a family of zinc-dependent enzymes that are capable of degrading extracellular matrix molecules, including collagen. � The rationale for using SDD as a HMT in the treatment of periodontitis is that doxycycline downregulates the activity of MMPs by a variety of synergistic mechanisms, including reductions in cytokine levels, and stimulates osteoblastic activity and new bone formation by upregulating collagen production � SDD is used as an adjunct to SRP and must not be used as a stand-alone therapy (monotherapy) � 20 mg capsules twice daily

Adjunctive use of orthodontic treatment Orthodontic therapy can provide several benefits to the adult periodontal patient. The following six factors should be considered: 1. Aligning crowded or malposed maxillary or mandibular anterior teeth permits the adult patient better access to clean all surfaces of their teeth adequately. This could be a tremendous advantage for patients who are susceptible to periodontal bone loss or do not have the dexterity to maintain their oral hygiene. 2. Vertical orthodontic tooth repositioning can improve certain types of osseous defects in periodontal patients. Often, the tooth movement eliminates the need for resective osseous surgery. 3. Orthodontic treatment can improve the aesthetic relationship of the maxillary gingival margin levels before restorative dentistry. Aligning the gingival margins orthodontically avoids gingival recontouring, which could require bone removal and exposure of the roots of the teeth. 4. Orthodontic therapy also benefits the patient with a severe fracture of a maxillary anterior tooth that requires forced eruption to permit adequate restoration of the root. Erupting the root allows the crown preparation to have sufficient resistance form and retention for the final restoration. 5. Orthodontic treatment allows open gingival embrasures to be corrected to regain lost papilla. If these open gingival embrasures are located in the maxillary anterior region, they can be unesthetic. In most patients, these areas can be corrected with a combination of orthodontic root movement, tooth reshaping, and restoration. 6. Orthodontic treatment could improve adjacent tooth position before implant placement or tooth replacement. This is especially true for the patient who has been missing teeth for several years and has drifting and tipping of the adjacent dentition.

Adjunctive Role of Orthodontic Therapy This patient was missing the mandibular left second premolar, and the first molar had tipped mesially (A). Pretreatment periapical radiograph (B)revealed a significant hemiseptal osseous defect on the mesial side of the molar. To eliminate the defect, the molar was erupted, and the occlusal surface was equilibrated (C). The eruption was stopped when the bone defect was levelled (D). The posttreatment intraoral photograph (E) and periapical radiograph (F) show that the periodontal health had been improved by correcting the hemiseptal defect orthodontically.

Orthodontic Treatment of Gingival Discrepancies This patient initially had triangular-shaped central incisors (A and B), which produced an open gingival embrasure after orthodontic alignment (C). Because the roots of the central incisors were parallel with one another, the appropriate solution for the open gingival embrasure was to recontour the mesial surfaces of the central incisors (D). As the diastema was closed (E), the tooth contact moved gingivally and the papilla moved incisally, resulting in the elimination of the open gingival embrasure (F).

Non-Surgical Treatment 1. Education & Plaque Control 4. Treat/temporize carious lesions 2. Supra & subgingival calculus removal 5. Adjunctive aids 3. Remove local factors 6. Re-evaluation

Step 6. Re-evaluation � Healing following non-surgical therapy is almost complete at 3 months. � Patients also need the opportunity to improve their plaque control skills to both reduce inflammation and adopt new habits. � At re-evaluation the effectiveness of treatment previously carried out is evaluated and the nature of furtherapy, if needed, is established. � Measurements are made at baseline and again at 3 months as a method of evaluation of periodontal status, effectiveness of therapy and to estimate prognosis. � Measurements include: § § § § plaque scores, bleeding on probing, suppuration on probing, probing pocket depth, recession, clinical attachment level, assessment of mobility.

Healing � Healing of the gingival epithelium consists of the formation of a long junctional epithelium rather than new connective tissue attachment to the root surfaces. � The attachment epithelium reappears 1 to 2 weeks after therapy. Gradual reductions in inflammatory cell population, crevicular fluid flow, and repair of connective tissue result in decreased clinical signs of inflammation, including less redness and swelling. � One or two millimeters of recession is often apparent as the result of tissue shrinkage � Transient root sensitivity frequently accompanies the healing process. Although evidence suggests that relatively few teeth in a few patients become highly sensitive, this development is common and can be disconcerting to patients.
 in improvements")
Average changes after non-surgical treatment Mean changes generally observed in studies a) in improvements in plaque and bleeding scores for sites of different initial probing depths b) in probing depth, probing attachment levels, and gingival recession after a single episode of supra- and subgingival instrumentation

Interpretation of probing measurements at re-evaluation � On average the change in pocket depth seen following treatment for deeper pockets is a combination of recession at the gingival margin due to resolution of inflammation and a tightening of the junctional epithelium at the base of the pocket. � Moreover the reduced bleeding on probing scores found after treatment may reflect the increased resistance to probe penetration into the connective

Effects of non-surgical treatment on microbiology �A re-emergence of species of the red and orange complex 3– 12 months post debridement may be associated with ongoing attachment loss at these sites (Haffajee et al. 2006). �In the absence of appropriate home care, the reestablishment of the pretreatment microflora as well as the rebound of clinical improvements due to treatment will occur in a matter of weeks (Magnusson et al. 1984; Loos et al. 1988; Sbordone et al. 1990). �In the absence of professional maintenance an increase in the prevalence and counts of periodontopathogens is to be expected (Renvert et al. 1990; Shiloah & Patters 1994).

Re-evaluation q Many patients can have their periodontal disease controlled with phase I therapy and not require further surgical intervention. q In patients who do need surgical treatment, phase I therapy is advantageous in that it also provides tissue with reduced inflammatory infiltration, thus improving the surgical management of the tissue and improving the healing response. q In the re-evaluation visit , consider surgery if: � Patients with 5 mm or more of attachment loss and with pockets present after phase I treatment. � Those patients who do not demonstrate the ability to have 20% or less of tooth surfaces free of plaque are poor candidates for successful surgical outcomes and should be closely monitored on a recall maintenance program until plaque control is established.
 consider:")
Re-evaluation q If no response to conventional non-surgical therapy (scaling and root planing/debridement) consider: �Antibiotics/antimicrobials �Repeat periodontal debridement �Periodontal surgery


Staged Vs. Full mouth disinfection � Traditionally non-surgical treatment of periodontitis involves a series of appointments separated by perhaps a week or more. Each appointment typically involves root debridement of a quadrant depending on disease severity. � In 1995 Quirynen et al. introduced the concept of total mouth disinfection as a new treatment strategy. It involved: § Full-mouth scaling and root debridement within a 24 -hour treatment period, § Subgingival irrigation (repeated three times within 10 minutes) with 1% chlorhexidine gel, § Tongue brushing with 1% chlorhexidine gel, § Mouth rinsing with 0. 2% chlorhexidine.

Staged Vs. Full mouth disinfection � This full mouth disinfection protocol aimed to reduce the bacterial load in pockets and intraoral niches to minimize the risk of reinfection of the treated pockets from areas harbouring pathogenic bacteria. � Recent studies suggested both the one appointment and staged or multiple appointment treatment strategies work well, microbial parameters were not significantly different after 8 months, regardless of treatment modality and the risk of recurrence of periodontal pockets was no greater for either modality. � Staged therapy permits the advantage of evaluating and reinforcing oral hygiene care, and the one or two appointment therapies can be more efficient in reducing the number of office visits the patient is required to attend.

Response of Furcation sites to nonsurgical treatment � Patient-performed home care and professionally performed subgingival debridement become more difficult. � Sheltered anatomic site for anaerobic and virulent microbes. � Sites with furcation involvement consistently demonstrated higher microbial counts and greater proportions of suspected periodontopathogens. � Generally clinical improvement was found to be less pronounced in furcation sites than in other locations (Loos et al. 1989) � Consequently, teeth with furcation involvement may be viewed with some caution with respect to long-term prognosis.

When to refer? � The rationale behind the 5 -mm standard is that the typical root length is about 13 mm and the crest of the alveolar bone is at a level approximately 2 mm apical to the bottom of the pocket. When there is 5 mm of clinical attachment loss the crest of bone is about 7 mm apical to the cementoenamel junction, therefore only about half the bony support for the tooth remains.

When to refer? �Specialist care can help preserve teeth in these cases by eliminating deep pockets and regenerating support for the tooth. � the treatment of periodontal diseases is generally successful in patients with 6 - to 8 -mm probe depths. Success rates diminish when probing depths are 9 mm or greater, so early referral of advanced cases is likely to provide the best results.

Reasons for referral q In addition to the 5 -mm standard and evaluation of probe depths, the following factors must also be considered in the decision to refer: I. Extent of disease and generalized or localized deep involvement. Extensive bone loss, even in localized areas suggest the need for specialized reconstructive techniques. II. Root length. Short roots are more seriously jeopardized by 5 mm of clinical attachment loss than long roots. III. Hypermobility. Excessive tooth mobility suggests contributing factors and a more guarded prognosis. IV. Difficulty of scaling and root planing. The presence of deep pockets and furcations makes instrumentation much more difficult and results can often be improved with surgical access. V. Restorability and importance of particular teeth for reconstruction. Long-term prognosis of each tooth is important when considering extensive restorative work VI. Age of the patient. Younger patients with extensive attachment loss are more likely to have aggressive forms of disease that require extensive therapy. VII. Lack of resolution of inflammation after scaling and planing. If inflammation persists, furtherapy is often necessary to gain the most positive results.


�S/RP is an essential part of non-surgical periodontal therapy , yet dose not result in complete removal of calculus. �Patient motivation and cooperation is important in success treatment outcomes. �Self performed OH should be applied regularly and modified if needed. �Re-evaluation provides a check for treatment success and patient’s level of cooperation.

Thank you
- Slides: 110