Discussion group 2 External fixation in nonunion infection























































 • Frame reassembling")



- Slides: 60
Discussion group 2 External fixation in nonunion, infection, and treatment of bone defects AO Trauma Online Masters Course—External Fixation
Case 1: Nonunion of tibia 2
• 42 -year-old man: 12 years status post open fracture • Previous intramedullary (IM) nail • No drainage, normal knee and ankle, pain with walking • Erythrocyte sedimentation rate: 32 3
• 42 -year-old man: 12 years s/p open fracture • Previous IM nail • No drainage, normal knee and ankle, pain with walking • Erythrocyte sedimentation rate: 32 • C-reactive protein < 1 • No infection suspected 4
Options for treatment? 1. Resection of nonunion with shortening, and lengthening at a more proximal location 2. Acute correction—IM nail then distraction 3. Gradual correction and distraction/deformity correction with ring fixator (hinge) 4. Gradual correction and distraction with hexapod frame 5. Gradual deformity correction at nonunion site and then lengthening at a proximal site 5
• Hexapod frame placed • Fibular osteotomy • Slow correction through nonunion (0. 25 mm/day) 6
Options? • Deformity corrected with difficulty and pain • Still 3 cm short 7
Options? 8 1. Continue distraction at 0. 25 mm/day? 2. Add proximal ring and continue lengthening via a new corticotomy (proximal)
Options? 9
10 • Proximal ring added—new corticotomy • 3 cm additional length obtained
11 • Proximal ring added—new corticotomy • 3 cm additional length obtained
Take-home messages • Hypertrophic nonunion can be distracted to correct deformity and create new bone • Consider separate location for lengthening if amount of bone is significant or difficulties arise 12
Case 2: Tibial defect 13
• • • Defect 10 cm Shortening 2 cm Varus Knee ROM 80/0/0 Ankle ROM 10/0/0 What next? 14
Preoperative planning 15
Preoperative planning • 2 -level corticotomy Corticotomy
Preoperative planning • 2 -level corticotomy Ring positions • Device: ring external fixator Corticotomy Ring positions
Preoperative planning • 2 levels corticotomy Ring positions • Device: ring external fixator • Method: 2 -level bone transportation (trifocal) Corticotomy Ring positions
Step 1: bone transport 19
Step 1: bone transport 20
Step 1: bone transport 21
Step 1: bone transport 22
Step 1: bone transport Next step? 23
Step 1: bone transport Next step? • 24 How to manage the docking site and deformity
Step 1: bone transport Next step? • 25 Fragments stabilization? How to manage the docking site and deformity
Step 1: bone transport Next step? • 26 Fragments stabilization? How to manage the docking site • Continue with ring? • Converse to nail? and deformity • Converse to plate?
Step 2: docking-site procedure with grafting Stable fixation for 5 months 27
Treatment period 8 months 28
Treatment period 8 months 4 years follow up 29
Take-home messages • In case of bone defects, malunion, deformities, and shortening—different types of surgical decisions are available • Ring fixator can correct bone defect; shortening malunion and deformities in one system • Multilevel corticotomy can be used for long bone defect • Bone graft at docking site is really useful to achieve union 30
Case 3: Distal tibial injury with infection 31
• • 48 -year-old man Industrial fall Open pilon Transferred 2 weeks after injury: wound still open • Serratia infection • Infected articular fragments in the wound • What are your thoughts? 32
• • 48 -year-old man Industrial fall Open pilon Transferred 2 weeks after injury: wound still open • Serratia infection • Infected articular fragments in the wound • What are your thoughts? 33
a. Antibiotic spacer and flap— plan for a Masquelet technique/ankle fusion using a hindfoot fusion nail b. Acute shortening to an ankle fusion—no need for softtissue coverage—proximal tibial lengthening c. Flap coverage and bifocal transport to an ankle fusion with a proximal corticotomy d. Other? 34
a. Antibiotic spacer and flap— plan for a Masquelet technique/ankle fusion using a hindfoot fusion nail b. Acute shortening to an ankle fusion—no need for softtissue coverage—proximal tibial lengthening c. Flap coverage and bifocal transport to an ankle fusion with a proximal corticotomy d. Other? 35
36
37
38
3. 5 cm 39
3. 5 cm • Final debridement in preparation for transport to ankle fusion 40
3. 5 cm • Final debridement in preparation for transport to ankle fusion • Rectus abdominus free flap 41
3. 5 cm • Final debridement in preparation for transport to ankle fusion • Rectus abdominus free flap • Ilizarov frame placed 3 days later 42
43
0. 75 mm/day transport rate 44
How should we manage the docking at the site of the ankle fusion? 0. 75 mm/day transport rate 45
• Rectus free flap was elevated • Iliac crest bone graft to docking site • Distal part of frame converted to hexapod to fine-tune position of the ankle fusion 46
• Rectus free flap was elevated • Iliac crest bone graft to docking site • Distal part of frame converted to hexapod to fine-tune position of the ankle fusion 47
• Rectus free flap was elevated • Iliac crest bone graft to docking site • Distal part of frame converted to hexapod to fine-tune position of the ankle fusion 48
Ankle fusion position verified on AP/lateral and a “heel view” 49
At 1 year 51
Take-home messages • When the joint is destroyed by trauma and infection, fusion is often a good option • Coverage with flap optimal to help clear infection • Bifocal treatment useful to maintain leg length • Fusion can be difficult, preparation of the docking site ± bone graft should be considered • Hexapod useful to allow optimal fusion position 52
Case 4: Pin tract infection and frame instability 53
• • 54 52 -year-old man Deep infection 17 cm tibia defect Frame for spacer stabilization after debridement
Frame examination shows signs of pin-tract infection • What are the causes? • How to prevent? • How to treat? 55
Frame examination: signs of instability • What are the causes? • How to prevent? • How to treat? 56
Frame examination: signs of instability • Frame removal? (next step? ) • Frame reassembling (why? how? ) • Other choices? 57
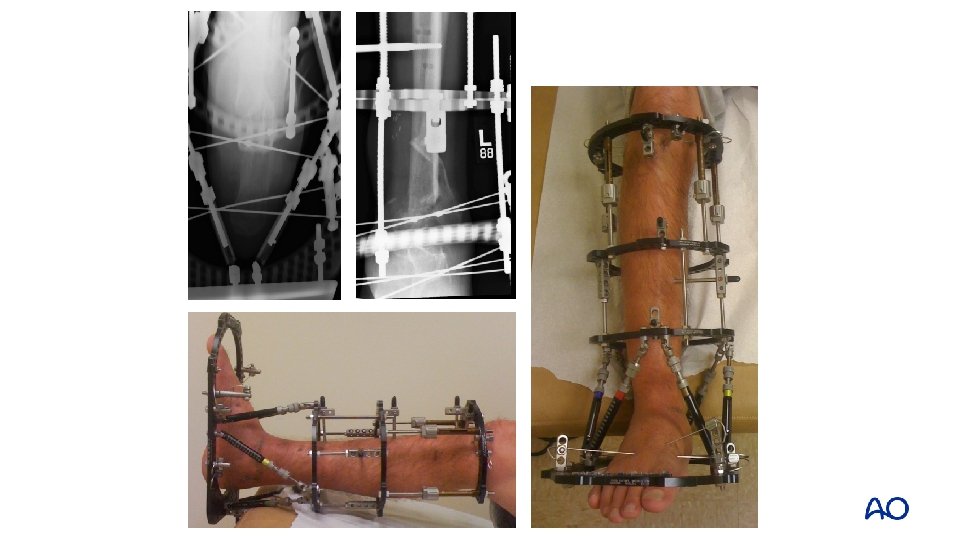
• Frame reassembling • Replacement of unstable wires • Wires tensioning 58
• Frame reassembling • Stabilizing half-pins insertion 59
Take-home messages • One of the causes of wire sites infection is unstable frame • Unstable frame will be infected frame soon (100%) • Needed level of stability depends on the purpose of using the frame (damage control orthopedics ≠ reconstructive surgery, needs more stability) • Proper level of stability must be provided with minimal number of wires, pins, and rings 60