DEFENSE MECHANISM OF GINGIVA CONTENTS n INTRODUCTION n




























")












 CIANCIO (1976) q METRONIDAZOLE")










 2. Composition, method")

- Slides: 59
DEFENSE MECHANISM OF GINGIVA
CONTENTS n INTRODUCTION n SALIVA Composition Functions Antibacterial factors n GCF Methods of collection Measurement of volume Composition Drugs secreted in GCF n Clinical Significance n Rationale for use of GCF as a diagnostic kit
INTRODUCTION n Defense mechanisms can be roughly divided into n INNATE DEFENSE MECHANISMS n ACQUIRED DEFENSE MECHANISMS.
n INNATE DEFENSE n First line, present from birth, genetic constitutional n Not enhanced by prior exposure to an infectious agent n Lacks immunological memory n and Antigenic specificity n ACQUIRED DEFENSE n Not present from birth, specific in nature-against microorganisms. n Natural/artificial and active/passive
The gingival tissue is constantly subjected to mechanical and bacterial aggressions. The Epithelial Surface, Saliva and the Gingival Crevicular Fluid provide resistance to these actions.
NON SPECIFIC HOST DEFENSE MECHANISM Epithelial barrier n Mechanical barrier to bacterial penetration n Protects against mechanical damages like mastication and brushing. n Basement membrane barrier to bacterial penetration
Keratinization n The protection afforded by the epithelium depend to a great extent on keratinization. n Keratin are a group of fibrous protein resistant to hydrolysis and enzymic action. Epithelial renewal n High rate of tissue turnover. n Constant renewal contribute to self cleansing tendency of the sulcular area. n Superficial injuries are repaired by the rapidity of cell turn-over.
SALIVA n Saliva has been defined as “the fluid secreted by the salivary glands that begins the digestion of foods”.
COMPOSITION OF SALIVA saliva n INORGANIC Ions like Na, k, ph, bicarbonates, fluorides, gases like co 2 ORGANIC
n n n n n n n COMPOSITION OF SALIVA Proteins Albmin Amylase B-glucuronidase Carbohydrates Cystatins Epidermal growth factor Esterases Fibronectin Gustin Histatins Immunoglobulin A Immunoglobulin G Immunoglobulin M Kallikrein Lactoferrin Lipase Lactic acid dehydrogenase Lysosyme Mucins Nerve growth factor Parotid aggregins Peptidases Phosphatases Proline rich proteins Ribonucleases Small Organic molecules Amino acids Creatinine Glucose Lipids Nitrogen Sialic acid Urea Uric acid Electrolytes Ammonia Bicarbonate Calcium Chloride Fluoride Iodine Magnesium Phosphates Potassium Sodium Sulphates Thiocyanate
Function Salivary Components - LUBRICATION Glycoproteins, Mucoids -PHYSICAL -do. PROTECTION -CLEANSING Physical Flow -BUFFERING Bicarbonate , Phosphate TOOTH INTEGRITY MAINTENANCE Minerals Probable Mechanism Coating similar to gastric mucin -do. Clearance of debris and bacteria Antacids Maturation, Remineralisation • Control of bacterial -ANTIBACTERIAL ACTION Ig. A Lysozyme Lacto Peroxidase. colonization • Breaks bacterial cell walls • Oxidation of susceptible bacteria
SALIVA Salivary Flow: n Depends on location of salivary gland&their ducts. n Higher salivary flow caries incidence. 2. Salivary Buffer n Prevent bacteria colonizing n Plaque microorganism produce acid from sugar if not buffered cause demineralization of enamel. n Bicarbonates and phosphate ions –buffering, n protein has a role in buffering n Urea serves as generated buffer 1.
n 3. Salivary p. H: 5. 6 to 7. 0 Avg-6. 7 n p. H falls during sleep, n enhanced during increased salivary flow rate. n 4. Salivary glycoprotein n Mucin n A. protection against dessication &environment insults like acids and degradative enzymes. n B. lubrication of covered surface. n C. antimicrobial effect.
n 5. Salivary antibacterial factors n Inorganic &organic factors influence colonization of bacteria. n A. Lysozyme: hydrolytic enzyme cleaves linkage b/w glycopeptide muramic acid. n Works on both gram +/-. n B. Lactoperoxidase thiocyanate: bactericidal prevents accumulation of lysine&glutamic acid which are essential for bacterial growth. n C. Lactoferrin: bacteriostatic property. depletes iron need for bacterial growth. n D. Myeloperoxidase: bacteriocidal for actinomyces.
n 6. Salivary antibodies n Ig. A is predominant in saliva, Ig. M. n Ig. G is predominant in GCF n 7. Salivary Enzymes n Hyaluronidase, lipase, beta-glucornidase, chondrotin sulphatase, catalases, peroxidase&collagenase n Increased in periodontal disease n 8. Coagulation factors n Factor viii, ix, x, xii n Blood coagulation&protect wound from bacterial invasion
Gingival Crevicular Fluid n Known since 19 th century. Waerhaug , Brill And Krasse in 1950. n GCF considered as Transudate or a Inflammatory Exudate n In healthy sulcus – less n During inflammation- increases n Passes from CT- EPI- GINGIVAL SULCUS
Gingival sulcus n It’s the shallow Crevice or space around the tooth bounded by surface of the tooth on one side and epithelial lining the margin of the gingiva on the other n V- shaped n Under absolute normal conditions, depth is 0 n - Histological – 1. 8 mm 1. 5 mm 0. 69 mm n Healthy gingiva- clinical depth is 2 -3 mm
Gingival sulcus/ crevice } FREE GINGIVA ATTACHED GINGIVA
GCF FUNCTIONS OF GCF • Cleanse material from the sulcus • Contains plasma protein • Possess antimicrobial property • Defense through antibody formation
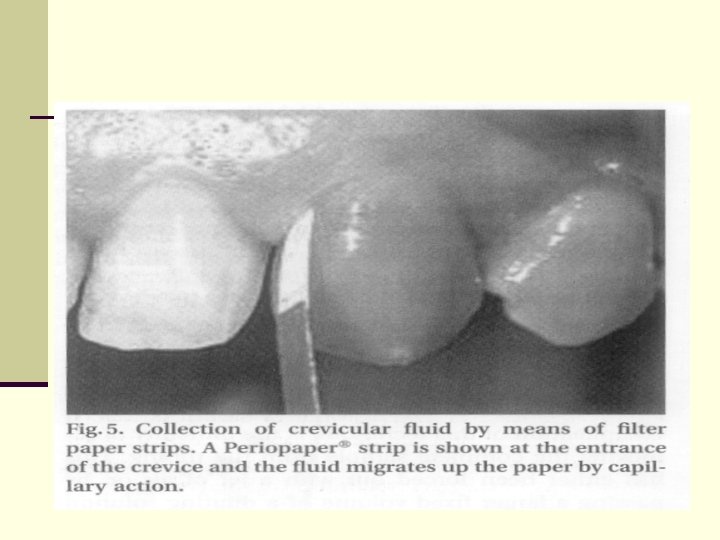
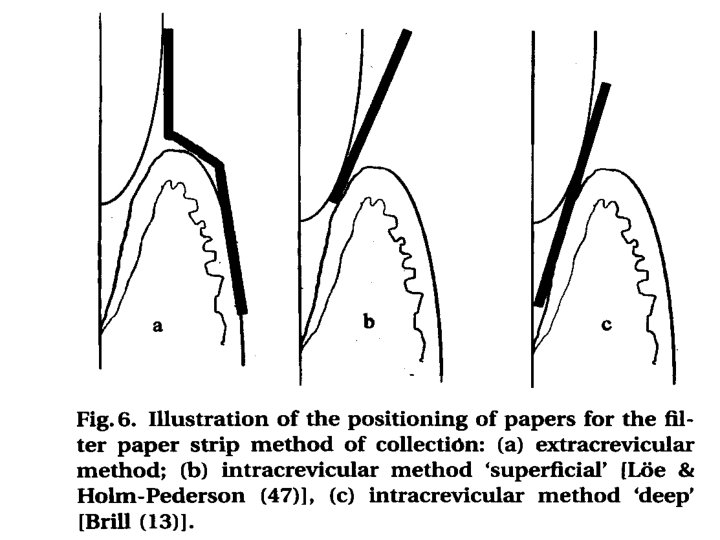
Method of collection n SAMPLING OF CREVICULAR FLUID BY MEANS OF ABSORBING PAPER STRIPS n TWISTED THREADS n SAMPLING OF GCF BY MEANS OF MICROPIPETTES n GINGIVAL WASHINGS
CAPILLARY TUBE
Gingival washings
MEASUREMENT OF THE VOLUME OF GCF STAINING o WEIGHING o PERIOTRON o
OTHER METHODS Various instruments have been used to obtain samples from crevicular area n PLASTIC STRIPS n TRANSPARENT STRIPS n PLATINUM LOOPS n MICROSPATULES
Methods of estimating the volume collected Appreciation by Direct Viewing or Staining n The amount of GCF collected on a strip was assessed by the distance the fluid had migrated up the strip. n This was often taken as a simple linear measurement, but a more accurate value was achieved by assessing the area of filter paper wetted by the GCF sample. n Further accuracy was achieved by staining the strips with ninhydrin to produce a purple color in the area where GCF had accumulated.
Weighing The Strip n This method involves the weighing of strips before and after sample collection. n This is a successful method but requires a very sensitive balance to estimate the very small amounts of fluid which may be collected from a healthy crevice. n Weinstein et al. (1967) use preweighed twisted thread into the gingival crevice around the tooth and determined the amount of fluid collected.
The Use of Periotron n The introduction of this measuring device, has allowed accurate determination of the GCF volume and subsequent laboratory investigation of the sample composition. n The instrument measures the affect on the electrical current flow of the wetted paper strips. n It has two metal 'jaws' which act as the plates of an electrical condenser.
n If a dry strip is placed between the 'jaws', the capacitance is translated via the electrical circuit and registers 'zero' on the digital readout. n A wet strip will increase the capacitance in proportion to the volume of fluid and this can be measured as an increased value in the readout. n The technique is rapid and has no discernible affect upon the GCF sample.
n Three models of Periotron have been produced (The 600, 6000 And Now 8000) and each one has been shown to be an efficient means of measuring the volume of fluid collected on filter paper strips. n One of the limitations of the Periotron has been its inability to measure volumes of GCF less than 1. 0 µl. n The newer Periotron 8000 has a wider range, particularly if the 'Sialo scale' is used, this being usually reserved for its role as a sialometer.
Problems with GCF collection and data interpretation Contamination n The major sources of contamination of GCF samples would be blood, saliva, or plaque. n The presence of dental plaque on filter paper strips used for collecting GCF has been shown to have a marked effect on the volume recorded. n Careful isolation should be performed in an effort to minimize the potential for saliva contamination.
Sampling time n The filter paper strips should be left in place for 5 seconds. n Alternative technique included leaving the strip in place for a longer period or the use of a sequence of repeated strips, with possible recovery periods in between. n This approach has sometimes resulted in collection times of 20 -30 min.
n The problem with prolonged collection times is that the nature of the GCF sample collected is likely to change with the protein concentration of the initial GCF collected comparable to interstitial fluid. n Whereas prolonged sampling at the site resulted in protein concentrations approaching those of serum.
Fluid Flow n Variation in fluid flow with time during the collection procedure greatly affect any quantitative observations on gingival fluid. n Depending upon collection procedure the amount of fluid production change in minutes following the contact of the paper strip with marginal region. n Fluid flow increase during interacrevicular as compared to extracrevicular method.
Volume determination n Evaporation is considered to be a significant problem in accurate volume determination of GCF samples. n This is particularly the case as the total volumes collected are usually less than 1µl and more often than not are less than 0. 5 µl. n Concerns are also expressed regarding the accuracy of the calibration graph produced for the Periotron, particularly with respect to small volumes
n Both these factors will result in small errors of volume determination, because the total sample of GCF collected is small the percentage of error is considered to be of more major significance.
Recovery from strips n Significant differences in the percentage recovery of proteins from filter papers is seen, which were dependent on both the type of paper and the concentration of the original protein sample. n Indeed, this may be a reason for conflicting results described between different research groups, possibly because of entrapment within, or binding of GCF proteins to the filter papers.
PERIOTRON
Volume of GCF n As Volume of GCF is low in healthy sites (0. 5 ml in 30 sec ) ,
Composition 1. Cellular elements n Bacteria n Desquamated epithelial cells n Leukocytes – PMN’s n Lymphocytes n Monocytes / Macrophages. 2. Electrolytes n Potassium n Sodium n calcium
3. Organic compounds n Carbohydrates Glucose hexosamine Hexuronic acid Glucose conc. is 3 -4 times greater than serum n Proteins protein content is less than serum Lipids n Metabolic and bacterial product Lactic acid, urea, endotoxins, h 2 s n
Enzyme and Enzyme inhibitors n n n n 1. Acid Phosphatase 2. Alkaline phosphatase 3. Pyrophosphatase 4. β-glycoronidase 5. Lysozyme 6. Hyaluronidase 7. Proteolytic enzymes Neutrophil elastase Cathepsin G Plasminogen activitor Collagenase Cathepsin D
DRUGS IN GCF q TETRACYCLINE BADER AND GOLDHABER (1966) CIANCIO (1976) q METRONIDAZOLE
CLINICAL SIGNIFICANCE CIRCADIAN PERIODICITY SEX HORMONES MECHANICAL STIMULATION SMOKING PERIODONTAL THERAPY
CLINICAL SIGNIFICANCE GENERAL HEALTH AND GINGIVAL FLUID 1. Circadian periodicity n Acc to intracrevicular technique flow is more in evening as compared to morning n But with orifice technique no difference in flow was found
2. GCF FLOW AND SEX HARMONES n Clinical investigations have shown an exacerbation of gingivitis during pregnancy, during menstural cycle and at puberty. n Increased in tooth mobility and pocket depth have also been reported during pregnancy. n Estrogen and progesterone cause increase in GCF flow
DRUG IN GCF n GCF is a characteristic feature of gingival inflammation. n It is expected that drugs given to a patient is carried from general circulation to the gingival sulcus or pockets by flow of GCF. n Bader and Goldhaber (1966) said that a major pathway of entrance into oral cavity of systemically administered drug is the gingival sulcus.
n The concentration of tetracyclines in GCF is 2 to 10 times that in serum. n Several studies have demonstrated that tetracyclines at a low GCF concentration (2 -4 µg/ml) are very effective against many periodontal pathogens. n TOLGA F. et al in their clinical study show that ciprofloxacin is found in GCF and its concentration in GCF is significantly higher than that in serum.
PERIODONTAL THERAPY AND CREVICULAR FLUID n The effect of repeated prophylaxis on plaque accumulation and gingival fluid flow were studied by Gwinnett et al. (1978). n They found that fluid flow decreases 1 week after the first prophylaxis and slowly returned to pretreatment value. n After second prophylaxis the lower levels of fluid were sustained for longer periods of time.
n 1 week after gingivectomy there is striking increase in GCF because of inflammation. n With restoration of gingival integrity, there is gradual drop seen in GCF after 5 weeks.
Leukocytes in the dentogingival area n The major site of entrance of leukocytes into the oral cavity is the gingival sulcus n Gingival fluid as well as neutrophilic granulocytes originate form the vessels of the gingival plexus. Upon leaving the plexus, they pass through the extra vascular connective tissue to enter the junctional epithelium via the external basal lamina. n In response to chemotactic gradients, they move by active locomotion through the inter- cellular spaces until they reach the sulcus bottom
n In the sulcus, the differential leukocytes countsn - 97% Neutrophils 1 - 2% Lymphocytes n 2 - 3% Monocytes n In the mononuclear leukocyte, the following % composition – n T-lymphocytes – 24% n B-lymphocytes – 58%. n Mean T cell to B cell ratio being 1 : 3. n
RATIONALE FOR THE USE OF GCF AS A DIAGNOSTIC TEST n GCF is easily and non-invasively collected and contains products of host, plaque and their interactions n site specific, small quantity is enough for diagnosis n more than 65 GCF constituents have been evaluated as potential diagnostic markers of periodontal disease progression n as GCF is derived from the periodontal tissues, analysis of its constituents may provide an early indicator of changes in the tissue.
Most Frequently Asked Questions 1. Defense mechanisms of gingiva (20 marks) 2. Composition, method of collection, functions, 3. 4. 5. 6. 7. clinical significance of GCF(20 marks) Saliva(5 marks) GCF(5 marks) Clinical significance of GCF(3 marks) Composition of saliva/GCF(3/5 marks) Functions of saliva/GCF(3/5 marks)