Pathogenesis of periodontal disease Dr Enas Razzoqi B

Pathogenesis of periodontal disease Dr. Enas Razzoqi B. D. S. , M. Sc. , Ph. D in Periodontics

Endotoxins lipopolysaccharide {LPS} a constituent of the cell wall of G-ve bacteria Cell constituents of both G+ve and G-ve bacteria may also play a role in P. d. disease. The presence of G-ve bacteria within pockets in P. d. disease leads to high concentrations of endotoxin. Endotoxin is released when the cell dies and may also be released by bacteria in the form of vesicles, or blebs of membrane derived from viable cells.

Endotoxins are highly toxic substances, affecting tissues directly or through activation of host responses. Endotoxin has the following effects: • Production of leukopenia. • Activation of factor XII which affect the clotting system leading to intravascular coagulation. • Activation of complement system. • Toxic effect on cells such as fibroblasts. • Induce bone resorption.

Both G+ve and G-ve subgingival bacteria produce a variety of toxic end products that are also capable of tissue destruction. These include: fatty and organic acids such as butyric and propionic acids, amines, volatile sulfur compounds, ammonia, and glycans.

Enzymes: Plaque bacteria produce a variety of enzymes that contribute to the production of P. d. diseases. • Collagenas and Aa). degradation of collage (P. gingivalis Degradation of collagen is a central characteristic of P. d. destruction.

• Hyaluronidase found in higher concentrations in P. d. packets capable of increasing gingival permeability by widening the intercellular spaces.

Evasion of host responses: E Bacterial factors also help in evasion of host defenses by influencing both cellular and humoral immune responses. PMNs, for example, are influenced by leukotoxins and chemotactic inhibitors. Immunoglobulins are inactivated or destroyed by proteases.

In 1976, Page and Schroeder classified the progression of gingival and periodontal inflammation into four phases: initial, early, established and advanced stages or lesions.
 gingiva is of 2 types:")
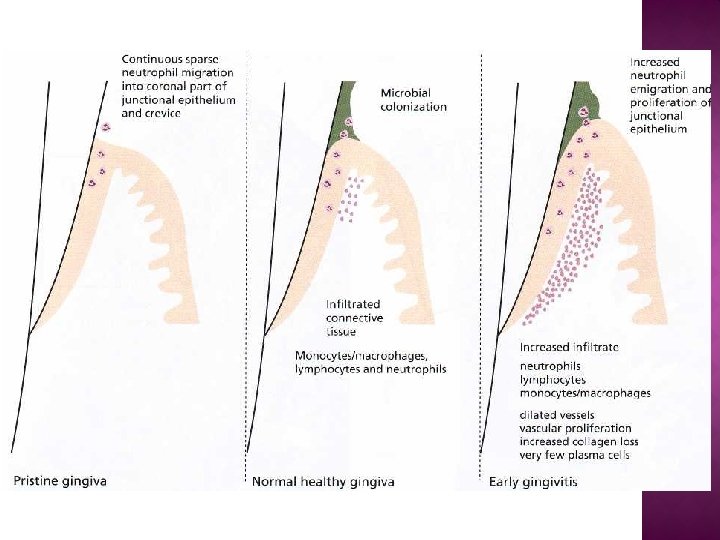
Clinical and histological features of the gingiva: normal (healthy) gingiva is of 2 types: super healthy or "pristine" state histologically has little or no inflammatory infiltrate certain leukocytes (neutrophils and macrophages), in the JE. clinically healthy" gingiva which looks similar clinically to pristine gingiva but histologically, features an inflammatory infiltrate. The normal healthy gingiva features an inflammatory cells infiltrate, predominantly neutrophils (JE) and lymphocytes (subjacent connective tissue).
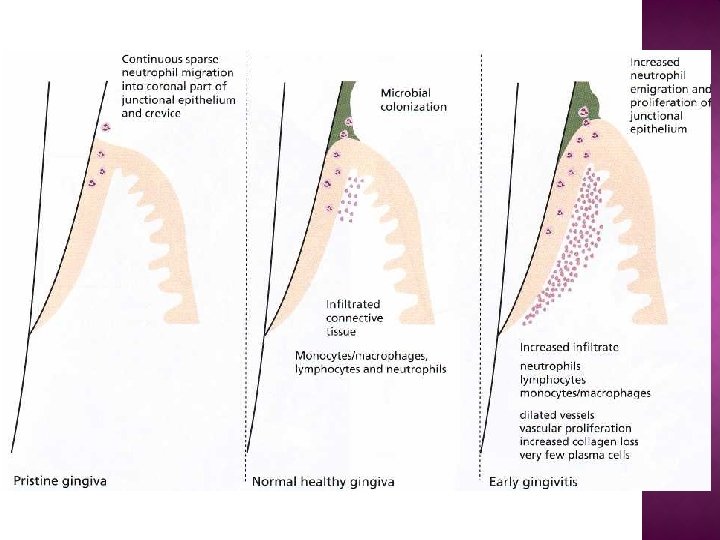

Normal gingiva clinically is characterized by: • pink color. • Firm consistency. • The gingival margin exhibits a scalloped outline. • The interdental papillae are firm and fill the space below the contact areas • Do not bleed on gentle probing. • The gingivae often exhibit a stippled appearance • There is a knife edge margin between tooth and soft tissue.

The histologic picture of developing plaque- related P. d. disease has been divided into 4 stages at the light microscope level: 1 - Initial lesion: • The first microscopically observable tissue changes occur after 2 -4 days of plaque accumulation, vascular changes have been observed beneath the junctional epithelium as: More blood is brought to the area. Dilation of the arterioles, capillaries and venules. An increase in the vascular permeability results so that fluids and proteins exude into the tissues. • There are small accumulations of polymorphonuclear leukocytes and mononuclear cells subjacent to the JE. • A decrease in perivascular collagen occurs in this area. • Gingival fluid can be detected clinically in the gingival sulcus. No more than 5 to 10% of the gingival connective tissue is involved during this stage.

Gingival inflammation: Within 10 -20 days of plaque accumulation, clinical signs of gingivitis are established in most individuals. This gingivitis appears as • Gingival redness. • Swelling • Increased tendency of soft tissue to bleed on gentle probing. Even at this stage, clinical signs are reversible following removal of microbial plaque by effective plaque control measures.

2 - Early lesion: Occurs after 4 -7 days of plaque accumulation Lymphocytes and PMNs are the predominant infiltrating leukocytes at this stage and very few plasma cells The inflammatory cell infiltrate may at this stage comprise as much as 15% of the connective tissue volume. The junctional and oral sulcular epithelium begin to from retepegs. • The collagen content is reduced approximately 70% in the areas of inflammation.

3 - Established lesion: • after 2 -3 weeks of plaque accumulation. • The plasma cell is now the predominant inflammatory cell type within the affected connective tissues. • The plasma cells produce immunoglobulins (antibodies), primarily of the Ig. G class. • The JE and OSE continue to proliferate and may now be considered pocket epithelium. • The epithelium shows areas of ulceration. • The collagen loss persists at the site of active disease, but areas distant from the lesion show foci of collagen formation. • The P. d. ligament and alveolar bone show no change at this stage.
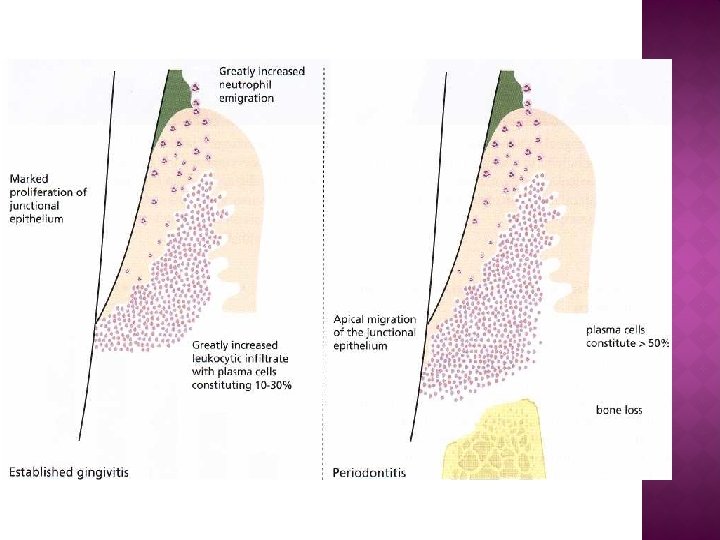

4 - Advanced lesion : • A varying amount of time elapses before the advanced lesion occurs. • There are many cases in which the advanced lesion never appears. The area of the lesion enlarges. • Strands of pocket epithelium penetrate deep into connective tissue. • There is extensive destruction of collagen fiber bundles of the gingiva. • The plasma cell continues to be the predominant cell type. • alveolar bone resorption occur
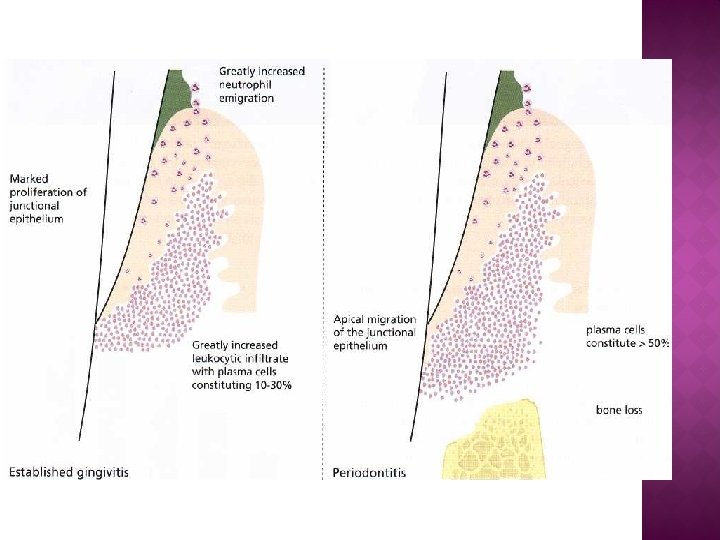

Clinical condition Histopathologic condition Pristine gingiva Histologic perfection Normal health gingiva Initial lesion of Page & Schroeder Early gingivitis Early lesion of Page & Schroeder (few plasma cells) Established gingivitis Established lesion with no bone loss nor apical epithelial migration (plasma cell density between 10% and 30% of leukocyte infiltrate) Periodontitis Established lesion with bone loss and apical epithelial migration from the Enamel to cemental junction (plasma cell density > 50%)
- Slides: 20