Transfusion Medicine Blood transfusion is like marriage it

Transfusion Medicine

�“Blood transfusion is like marriage: it should not be entered upon lightly, unadvisedly or wantonly or more often than is absolutely necessary. ” –Robert Beal, past director of International Federation of Red Cross

� 1660 s: First experiments in blood transfusion, transfused dog blood to humans. Patient died and experiments were banned. � 1818: James Blundell, British OBGYN, inspired after seeing women bleed to death from uterine losses. Successfully did human transfusions. Mortality up to 50% likely due to ABO incompatibility. � 1900: Karl Landsteiner discovered ABO blood groups. � 1940: Red Cross established to help supply blood products during WWII. Transfusions: History
 “On the transfusion of blood by the syringe. ” Source: Blood")
Blundnell’s gravitator (1818) “On the transfusion of blood by the syringe. ” Source: Blood Journal
 �Fresh frozen plasma (FFP) �Cryoprecipitated AHF �Platelets �Granulocytes")
�Whole blood �Red blood cells (PRBCs) �Fresh frozen plasma (FFP) �Cryoprecipitated AHF �Platelets �Granulocytes Blood components & products

Blood Collection: whole blood
")
Blood collection: apheresis (“a taking away”)

Red Blood Cells

Red blood cells

� Indications for transfusion ◦ Symptomatic anemia ◦ Red blood cell exchange � Action ◦ Increases oxygen carrying capacity by increasing circulating red cell mass � Dosing ◦ Each unit contains enough Hgb to increase by about 1 g/d. L ◦ Each unit contains 250 mg of iron � Administration ◦ Must be ABO compatible ◦ ABO/Rh typing, Ab screen, crossmatch ◦ Initial portion of each unit transfused slowly to look for reactions, then infusion can be as rapid as tolerated ◦ Finish transfusion within 4 hours (do not leave at room temp > 4 hrs) Red blood cell transfusion

�Collections and Storage of p. RBCs �Half Life of stores platelets is somewhat shorted than normal expected RBC lifespan (120 days) �Lifespan of transfused red cells closer to 50 -60 days ◦ Thought 2/2 to depletion of 2, 3 DPG ◦ Stores of ATP are diminished in stored RBCs Transfusion of Blood Products

�First described by Karl Landsteiner in 1900 �Won the Nobel Prize in Medicine for his work �First successful, “matched” blood transfusion was done by Dr. Reuben Ottenberg at Mt. Sinai Hospital in 1907. Blood Groups - ABO

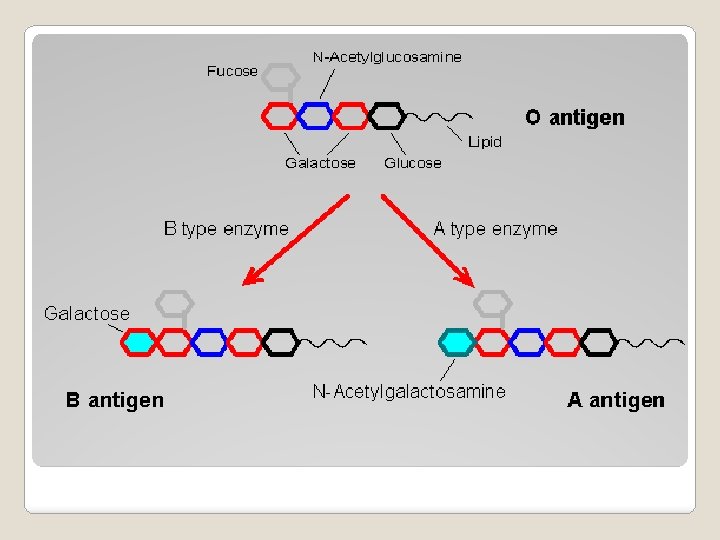
�Carbohydrate antigens in which the alleles are determined by the end moiety �Addition of n-acetylgalactomine to the base structure yields blood group A �Addition of galactose to the base structure (a galactose moiety) yields blood group B �Lack of any additional moieties yields blood group O Blood Groups - ABO

Minor Antigen Groups

�RH Blood Group ◦ 2 nd most important after ABO ◦ Consists of 50 antigens ◦ D, C, c, E, e are most important ◦ RH positive vs negative refers to the presence of absence of the D antigen ◦ Part of the routine Type and Screen and Crossmatch antigens that we test for Rh Blood Groups

�Most clinically relevant in hemolytic disease of the newborn �An Rh negative mother with an Rh positive father can result in an Rh positive child �Exposure of fetal cells to mother creates anti. D Abs �Use of Rho. GAM has reduced the incidence from close to 16% down to less than 1% �Given at week 28 -30 and again within 72 hrs postoperatively RH Blood Group

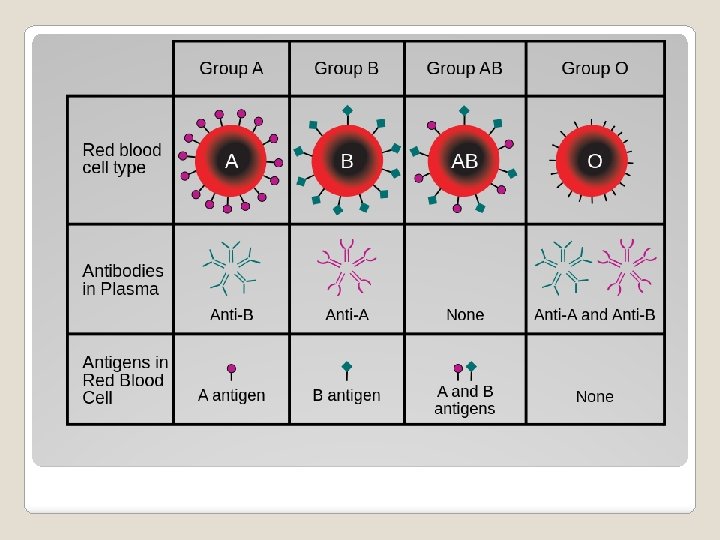
�Type and Screen ◦ Front type: what antigens are on the patient’s RBCs ◦ Back type: identify Ab in the patient’s serum A antigen Type A only anti-B Type A B antigen Type B only anti-A Type B anti-A and anti- Type O B A and B Type antigen AB Neither A or B Type O Blood Groups neither anti-A or Type AB anti-B

�Screen ◦ Look for red cell alloantibodies that may have formed in pregnancy or after prior transfusions ◦ If screen is positive, need to identify the Ab

�Type and Cross ◦ Crossmatching involves actually taking donor red cells and mixing with a portion of the patient’s serum to look for a reaction ◦ At least 2 units of PRBCs are crossmatched for the patient and reserved for the patient – these units cannot be used by anyone else Blood Groups

�So why are these important in transfusion medicine? Blood Groups - ABO

�Complications of RBC transfusion ◦ Acute hemolytic transfusion reaction ◦ Febrile nonhemolytic transfusion reaction ◦ Allergic reaction ◦ Anaphylactic reaction ◦ Transfusion related acute lung injury (TRALI) ◦ TACO ◦ Iron overload

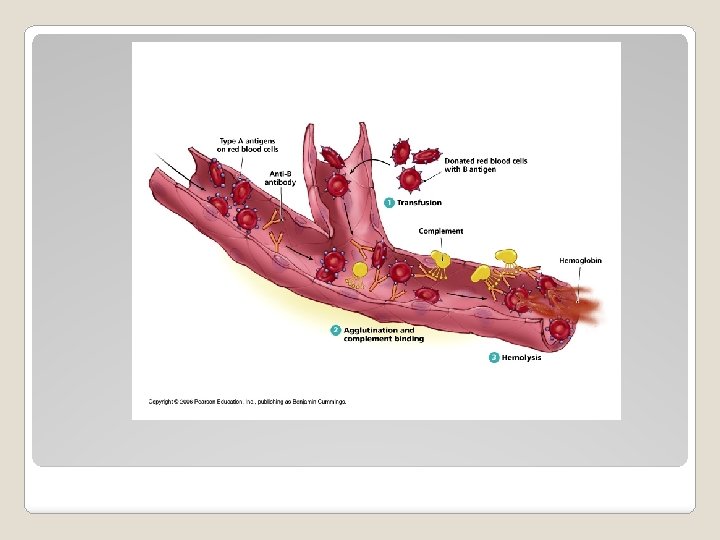
�Acute Hemolytic Transfusion Reaction ◦ Due to ABO incompatibility ◦ Usually due to human ID errors (mislabeling) �Symptoms ◦ Classic Triad: Fevers/Chills, Flank Pain and Red Urine ◦ Also dyspnea, chest/back pain, shock ◦ If patient is in surgery under anesthesia: red urine, hypotension, DIC Blood Groups - ABO

�Lab findings: ◦ Hemoglobinuria ◦ Elevated bilirubin ◦ Positive DAT/Direct Coomb’s �Treatment: supportive ◦ Stop transfusion immediately ◦ Notify blood bank to review ◦ Send blood sample from patient along with implicated unit ◦ Maintain/correct BP ◦ Correct coagulopathy, if present ◦ Promote and maintain urine flow

�Delayed transfusion reaction ◦ Occur in patients who are previously alloimmunized ◦ Antigens on transfused cells provoke antibody production ◦ Usually occurs 2 -14 days after transfusion ◦ Signs/symptoms: fever, positive DAT, decrease in H&H, elevated LDH and bili ◦ Most times this is benign and requires no treatment
 ◦ Due to")
�Febrile nonhemolytic transfusion reaction ◦ Fever shortly after transfusion (without infection) ◦ Due to cytokines or Abs against WBCs in the transfused blood ◦ More likely to occur if alloimmunized during pregnancy or previous transfusion ◦ Reduce occurrence by using leukocyte reduced RBCs or platelets ◦ Incidence: in less than 1% of LR-RBCs and less than 5% of LR-platelets Transfusion

�Anaphylactic reactions ◦ Reported in Ig. A deficient patients who develop Abs to Ig. A ◦ Symptoms: hypotension, tachycardia, N/V, diarrhea, bronchospasm, laryngospasm ◦ Use epinephrine, supportive care ◦ Reduce incidence: use washed cellular components

�TRALI ◦ Thought to be caused by WBC Abs in donors or inflammatory molecules in blood product ◦ Stimulate an inflammatory response in a “primed” donor ◦ Cause injury to alveolar capillary membrane, increased permeability, pulmonary edema ◦ Symptoms: acute onset of hypoxia and noncardiogenic pulmonary edema within 6 hrs of a transfusion ◦ Treatment: Aggressive supportive care ◦ Reduce occurrence by leukoreducing blood products and preferentially using plasma donated by males.

�TACO ◦ Circulatory overload leading to pulmonary edema ◦ Occurs after transfusing high volumes or at very rapid rates ◦ Higher risk in people with underlying cardiopulmonary or renal disease, very young or elderly, and people with chronic anemia who have low red cell mass and high plasma volume ◦ Treat: supportive, reduce pulmonary edema

�Bacterial sepsis ◦ Due to gram negative or positive organisms in the transfused product, often skin contaminants ◦ Symptoms: high fever, hypotension, shock during or shortly after transfusion ◦ Treat: stop transfusion, give abx and pressors prn. Send blood cxs from patient and culture specimens from container and blood administration set, report to blood bank. ◦ Occurs more often with platelets (stored at room temp). Most platelets are routinely tested for bacterial contamination.
")
�Infection transmission ◦ Blood products are all tested for: �HIV (1 in 1, 000) �HTLV I and II (1 in 2, 000) �Hepatitis B (1 in 200, 000) �Hepatitis C (1 in 1, 000) �Syphilis (treponema pallidum) �West Nile Virus �Chagas (trypanosome cruzi) ◦ Other risks: CMV, malaria, bacteria, Lyme, Dengue, Babesiosis, Creutzfeld-Jakob Infectious risks
 �Fresh frozen plasma (FFP) �Cryoprecipitated AHF �Platelets �Granulocytes")
�Whole blood �Red blood cells (PRBCs) �Fresh frozen plasma (FFP) �Cryoprecipitated AHF �Platelets �Granulocytes Blood components & products

� Plasma: FFP ◦ Contains all plasma proteins including all coagulation factors � 10 -15 m. L/kg raises factors ~25% ◦ Ready to use after thawing, must be discarded after 24 hrs or stored as thawed plasma ◦ Indications for use �Preop or bleeding patients who need replacement of multiple factors (liver disease, DIC) �Patients taking warfarin who need transient reversal of warfarin before Vit K would take effect �TTP (transfuse or plasma exchange) �Patients with plasma protein or factor deficiencies, if no specific factor concentrate or recombinant product is available Fresh Frozen Plasma

�FFP precautions ◦ One unit is about 250 m. L (can be up to 600 m. L if apheresis derived). High risk for volume overload. ◦ Plasma must be ABO compatible with the patient’s red cells. ◦ Average INR of FFP is 1. 5. Will not correct INR below this value. Fresh Frozen Plasma
 ◦ Allergic reactions ◦ Febrile reactions ◦ TACO")
�FFP: complications/hazards ◦ Infection (bacterial, viral) ◦ Allergic reactions ◦ Febrile reactions ◦ TACO ◦ TRALI Fresh Frozen Plasma
 �Fresh frozen plasma (FFP) �Cryoprecipitated AHF �Platelets �Granulocytes")
�Whole blood �Red blood cells (PRBCs) �Fresh frozen plasma (FFP) �Cryoprecipitated AHF �Platelets �Granulocytes Blood components & products

�Cryoprecipitated anti-hemophilic ◦ That FFP recover the precipitate ◦ Contains: �Fibrinogen �Factor VIII �Factor XIII �v. WF �Fibronectin factor ◦ Each unit contains 80 IU Factor VIII and 150 mg fibrinogen in 5 -20 m. L plasma Cryoprecipitate

�Indications: ◦ Control bleeding due to low fibrinogen ◦ Treat Factor VIII deficiency when recombinant proteins not available ◦ Second line therapy for v. WD and hemophilia A ◦ ABO compatible preferred ◦ Dose: 1 bag per 10 kg of body weight will raise fibrinogen by 50 -75 mg/d. L Cryoprecipitate
 �Fresh frozen plasma (FFP) �Cryoprecipitated AHF �Platelets �Granulocytes")
�Whole blood �Red blood cells (PRBCs) �Fresh frozen plasma (FFP) �Cryoprecipitated AHF �Platelets �Granulocytes Blood components & products

�Platelets needed for normal hemostasis �Platelets are collected from a single donor (separated from whole blood) or pheresed and pooled from different donors (1 unit = 4 -6 single donor units) Platelet Transfusions

�Indications for transfusion: ◦ Thrombocytopenia ◦ Dysfunctional platelet bleeding ◦ Active platelet related bleeding ◦ Prophylactic use for high risk of bleed ◦ Hematologic conditions ◦ Patients on ECMO or cardiopulmonary bypass �Do not use: ◦ In HIT, TTP, or ITP, unless patient has significant bleeding Platelet Transfusions

�Compatibility necessary testing not routinely �Therapeutic dose: ◦ 1 unit apheresis platelets ◦ 4 -6 units of whole blood derived platelets ◦ Should raise platelets by 5 -10 k �Transfused 3 -5 days platelets have a short lifespan! Platelet Transfusions

� Platelet alloimmunization ◦ Platelets have HLA and platelet specific antigens on their surface ◦ Patients who get transfusions often develop HLA antibodies and may become refractory to platelets ◦ Check CBC 10 -60 minutes post transfusion if Abs present, will not see response ◦ If poor response is due to splenomegaly, sepsis, fever, or DIC, will usually see early response to transfusion but reduced 24 hr survival ◦ Can do tests to look for presence of Ab against platelet antigens Platelet Transfusions
 �Contains Vitamin K dependent factors (II, VII, IX, X) �Used")
�Prothrombin Complex Concentrate (PCC) �Contains Vitamin K dependent factors (II, VII, IX, X) �Used to reverse the effects of Vitamin K antagonists Factor Concentrates
 ◦ Transfuse RBCs, platelets, plasma in 1:")
� Massive transfusion for severe hemorrhage (trauma) ◦ Transfuse RBCs, platelets, plasma in 1: 1: 1 ratio ◦ Need FFP otherwise clotting factors will be diluted and worsen coagulopathy � Blood is anticoagulated with sodium citrate and citric acid. ◦ In massive transfusion, can get metabolic alkalosis and hypocalcemia from excessive citrate. � Hypothermia can develop when transfusing more than 3 units use a blood warmer. Special scenarios
- Slides: 47