Congenital Cyanotic Heart Disease Ghada ElShahed MD Assistant




")
 o Clubbing ( > 1 year)")



 o Ejection systolic murmur (upper")


")




















- Slides: 39
Congenital Cyanotic Heart Disease Ghada El-Shahed, MD Assistant Professor of Cardiology
Cyonosis o It occurs when there is > 3 mg/dl reduced hemoglobin. o Central vs. peripheral cyanosis o Congenital Cyanotic Heart Disease >>> central cyanosis
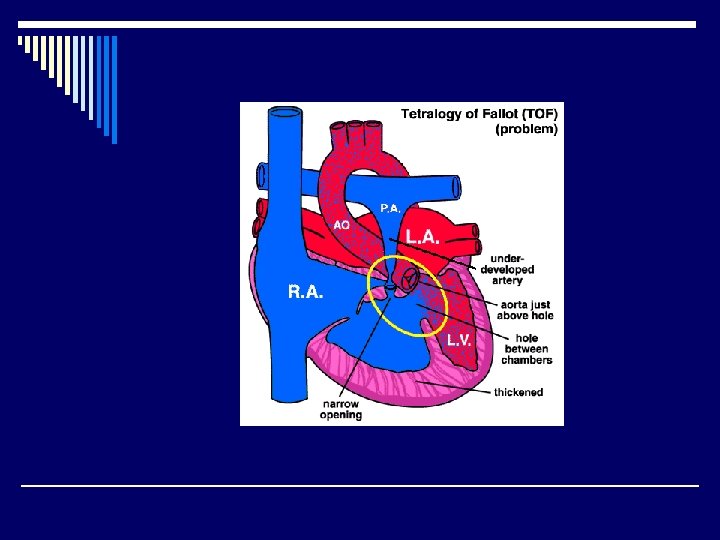
Tetralogy of Fallot o 10 % of all CHD o. The commonest Congenital Cyanotic Heart Disease
PATHOLOGY
This malformation has 4 components: o VSD o Obstruction to RV outflow (Infundibular, valvular) o Overriding of the aorta o RV hypertrophy
Clinical Picture o Cyanosis (onset < 1 year) o Clubbing ( > 1 year) o Effort intolerance o Squatting o Failure to thrive and delayed milestones o Cyanotic spells (hypoxic sells)
Physical signs General o Delayed development o Central cyanosis o Clubbing o Squatting position
clubbing
Physical signs Local o Quiet precordium with no bulge o RV impulse : Lt. sternal border o Systolic thrill
auscultation o Loud single S 2 (aortic in origin) o Ejection systolic murmur (upper LSB) (intensity is inversely proportional to severity of obstruction) Very faint or absent during cyanotic spell o Continuous murmur: PDA or collaterals
Complications o Cyanotic spells o Polycythemia, coagulation disorders o Infective endocarditis o Paradoxical embolization o Brain abscess or infarction
: ECG o RV hypertrophy
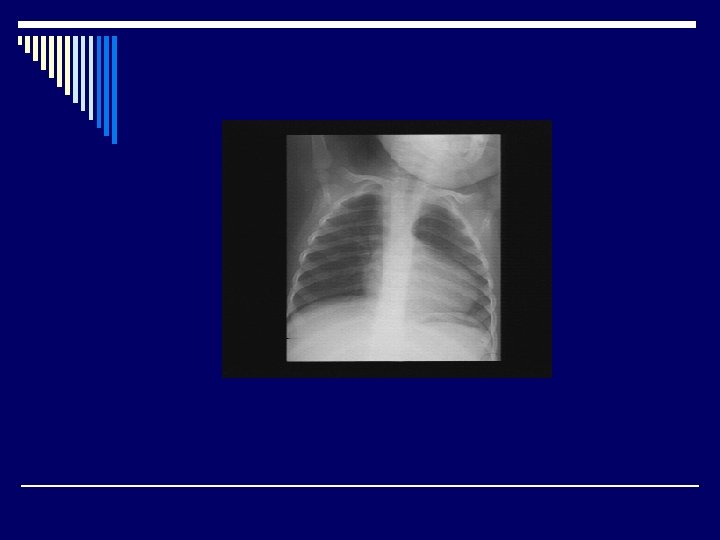
Chest X-ray o. Normal-sized boot shaped heart ( RV prominence + concavity at PA) o. Decreased pulmonary vascular markings o. Right-sided aortic arch
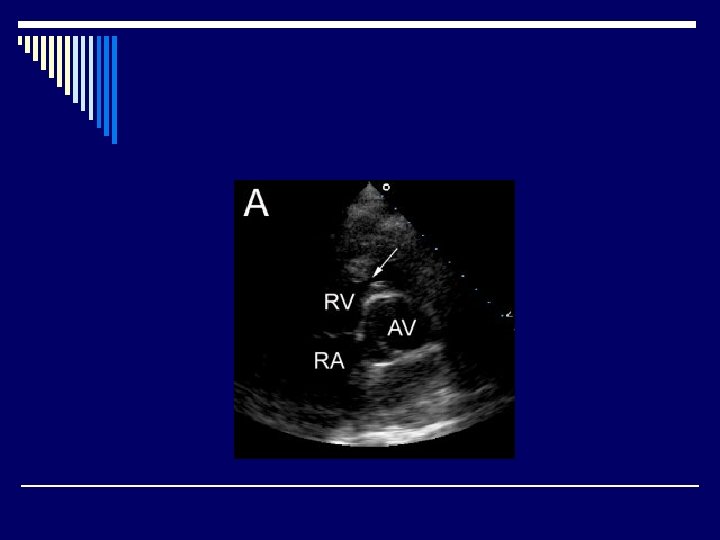
Echocardiography o. Diagnosis o. Decision-making o. Pre-and post-operative evaluation
TOF
Cardiac catheterization o PA sizes o Coronary anatomy (to exclude coronary anomalies as abnormal origin or abnormal course) o Collaterals
Managemement
o Medical: --Infective endocarditis prophylaxis and treatment -- Treatment of cyanotic spell * Oxygen * Knee-chest position * Morphia * Correct acid-base balance * Fluids, vasopressors * Ventilation * Prevention of recurrence
Surgical treatment o Palliative: Shunt surgery o Corrective: VSD closure, Infundibular resection to relieve RVOT obstruction, trans-annular patch. o Choice: RVOT anatomy and PA sizes are the most important factors
VSD patch closure
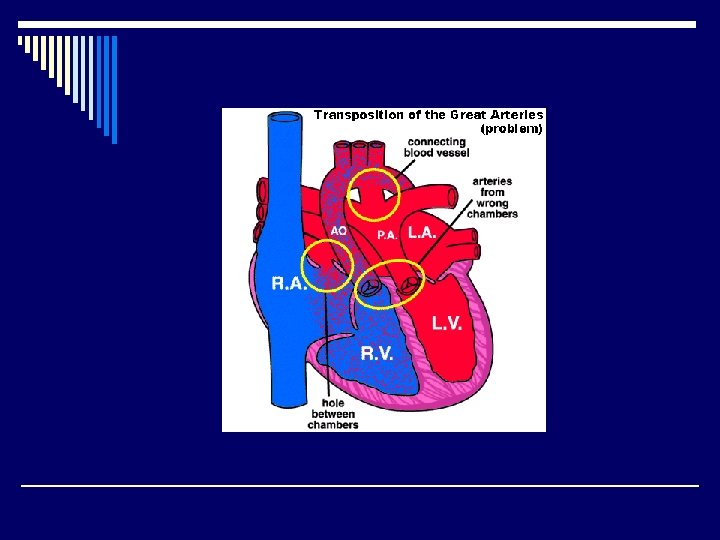
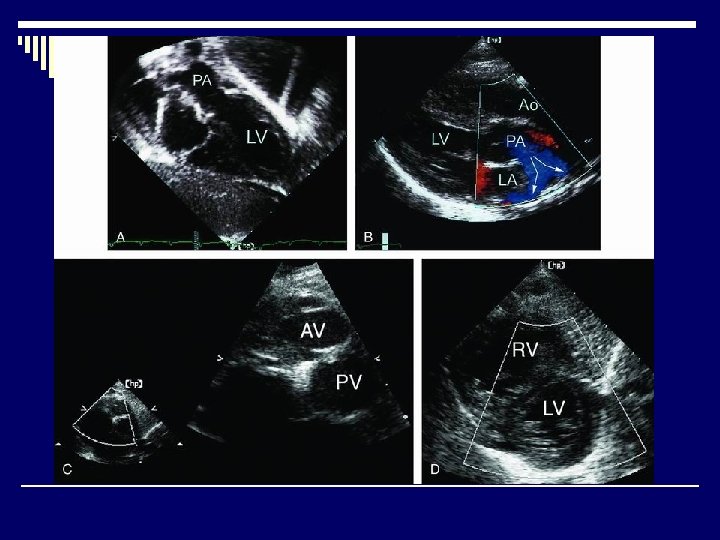
Transposition of the (great arteries (TGA
Eisenminger Syndrome ( (reversed shunt
o Cyanosis developing in a patient who originally had a congenital acyanotic heart disease with left to right shunt o Left to right shunting >> increased pulmonary blood flow >> pulmonary vascular damage >> increased PA pressure >> increased pressure in rightsided cardiac chambers >> bidirectional shunt >> right to left shunt
VSD with reversed shunt o Decreased signs of hyperdynamic LV (due to decrease of shunt) o Diminished murmur >> absent o Signs of RV pressure overload o Cyanosis with effort >> at rest o Clubbing
o ECG: RV hypertrophy o Echo: RV enlargement Markedly increased RV pressure VSD flow is mainly right to left o Cardiac catheterization: Increased pulmonary vascular resistance o Corrective surgery is contra-indicated
Questions
The most common congenital : cyanotic heart disease is o TGA o Tetralogy of Fallot o Tricuspid atresia o Eisenminger disease
The most important investigation to diagnose Tetralogy of Fallot is o Cardiac catheterization o Echocardiography o ECG o Chest X-ray
Cyanosis in Tetralogy of Fallot is o Always present since birth o Never present since birth o Usually appears after birth
The second heart sound in Tetralogy of Fallot is o Widely split o Narrowly split o Very faint o Usually single
The treatment of Eisenminger disease is o. Urgent surgical defect closure o. Urgent defect closure by cardiac cathterization o. Medical treatment
o Discuss the clinical picture and the treatment options for a patient with Tetralogy of Fallot o Discuss the complications of uncorrected Tetralogy of Fallot and the detailed management of one of them