Common Allergy Symptoms Among Toddler CME for NURSES





 (IMMUNE SYSTEM) IMMEDIATE TYPE (Ig. E) NON –Ig. E Atopic")

































 • The most valuable diagnostic tool for confirming suspected")






- Slides: 48
Common Allergy Symptoms Among Toddler CME for NURSES Dr Intan Hakimah Ismail Consultant Paediatrician Paediatric Allergist and Immunologist Universiti Putra Malaysia
Overview – allergic disease • Prevalence • Definition • Clinical manifestations • Diagnosis
Allergic disease • Affects 30 -40% of people worldwide 1 • The 5 th leading chronic disease among all ages • The 3 rd common chronic disease among children under 18 years old; up to one child in three is affected • The prevalence is increasing in all regions of the world undergoing industrial development and westernization 1 WAO White Book on Allergy 2011/12
• Allergies affect people from the early stages of their life and continue until their late adult ages • A major global health issue
Asthma Food allergy Eczema Allergic rhinitis
HYPERSENSITIVITY ALLERGY “INTOLERANCE” (NON-IMMUNE) (IMMUNE SYSTEM) IMMEDIATE TYPE (Ig. E) NON –Ig. E Atopic Eczema Asthma Rhinitis
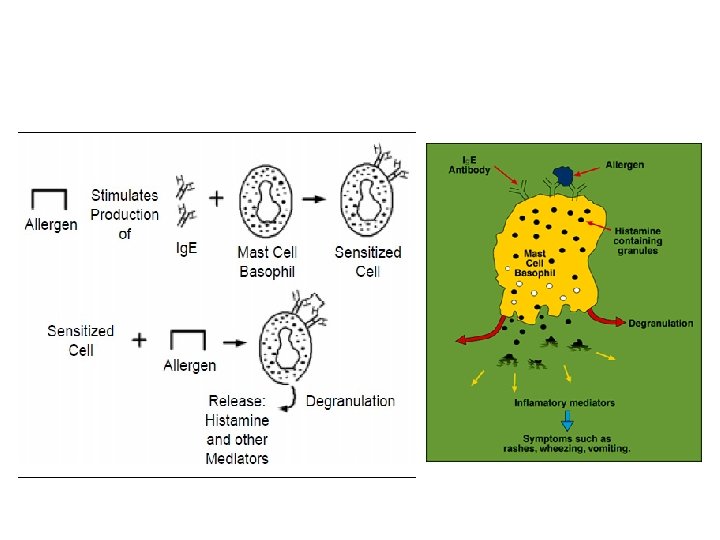
What causes allergic reactions? • Overactive immune system • Body believes a substance is harmful • Body wants to protect itself by fighting that substance off • Immune system releases chemicals and histamine, triggering the reaction
Why are allergic diseases on the rise?
The allergic reaction Allergic immune response
Allergic reactions
Allergic march The phenomenon of switching from one clinical expression of allergy to another in progressive stages of life
Identifying“At “at risk” Identifying Risk”infants Infants One parent or sibling with history of AD, urticaria, allergic rhinitis (hay fever) or asthma = “At Risk” by Family History Risk by Parental Hx. * Percentage of newborns Likelihood of developing allergy symptoms *Approximate numbers in developed countries. Adapted from 1. Bousquet J. et al. J Allergy Clin Immunol 1986; 78: 1019 -1022 2. Halken S et al. Allergy 2000; 55: 793 -802 3. Kjellman N. et al. Acta Paediatr Scan 1977; 66: 565 -71 4. Exl BM, Nutr Res 2001; 21: 355 -79 Low Medium High
Predicting. Pediatric pediatric allergy Predicting Allergy Risk by Parental Hx. * Percentage of newborns Likelihood of developing allergy symptoms Actual # of children/100 who will develop allergies *Approximate numbers in developed countries Low Medium High
Predicting. Pediatric pediatric allergy Predicting Allergy Risk by Parental Hx. * Low Medium Percentage of newborns Likelihood of developing allergy symptoms Actual # of children/100 who will develop allergies There is no good public health mechanism to predict all children who will develop allergy. At least half of infants who go on to develop allergy *Approximate numbers in developed countries could not have been predicted High
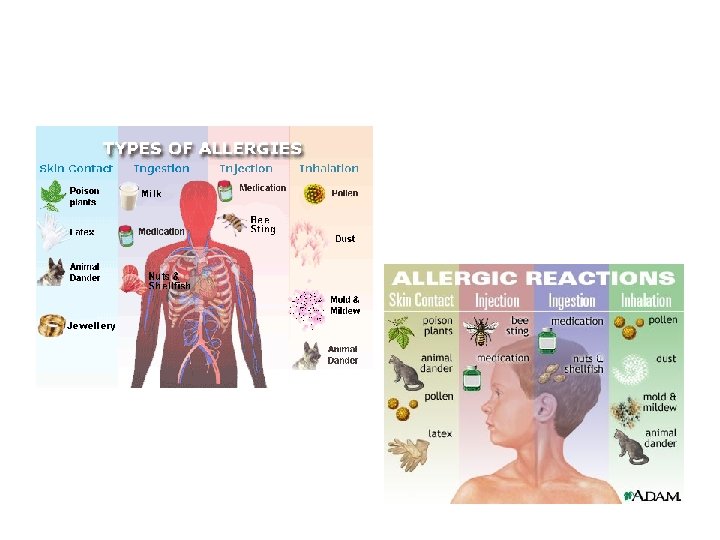
Allergyisisaasystemic disorder Allergy disorder Nose Oesophagus Food allergy Pharynx Allergic rhinitis Asthma Lungs Stomach Skin Eczema Urticaria Allergic dermatitis “Global diseases” – due to the large spectrum of symptoms affecting the whole body
Food allergy…fact or fiction? • Lactase deficiency • Galactosemia • Pancreatic insufficiency • Bacterial food poisoning • Scromboid fish poisoning • Caffeine • Tyramine • Histamine
Adverse reactions to food NON-TOXIC Immunemediated Allergy Non-Ig. E-mediated Adverse Reactions to Food: Position Paper. Allergy 1995; 50: 623 -635 Non-immune mediated Intolerance Enzymatic Pharmacologic Undefined
A food allergy is not: • The inability to digest a food • An aversion to a food (disliking a food) • Food poisoning • A reaction to a food additive
The“Big Eight”: The Eight”
Causes 90%of of food allergies Causes of of 90% Food Allergies In children In adults Milk Eggs Peanuts (groundnuts) Tree nuts (almonds , hazelnuts and walnuts) • Soy • Wheat • Peanuts (groundnuts) • Tree nuts (almonds , hazelnuts and walnuts) • Fish • Shellfish (mussels, crab, lobster and shrimps) • •
Some food allergies may be “outgrown” Sometimes “outgrown” • Egg • Milk • Soy Usually not “outgrown” • Peanuts • Tree nuts • Fish • Shellfish
The essential components of allergy diagnosis Medical history and physical examination Diagnostic confirmatory test Skin test or Blood test Elimination Diet Challenge test
Food allergy: symptoms
Food allergy: clinical manifestations
Ig. E-mediated food allergy Within minutes of ingestions • Anaplyhlaxis o skin and mucosa o respiratory/GI symptoms o fall in blood pressure o organ dysfunction symptoms o shock
Ig. E-mediated food allergy Within minutes of ingestions • Anaplyhlaxis o skin and mucosa o respiratory/GI symptoms o fall in blood pressure o organ dysfunction symptoms o shock • Skin (50 -60%): o angio-oedema o urticaria o pruritis
Ig. E-mediated food allergy Within minutes of ingestions • Anaplyhlaxis o skin and mucosa o respiratory/GI symptoms o fall in blood pressure o organ dysfunction symptoms o shock • Skin (50 -60%): o angio-oedema o urticaria o pruritis • Gastrointestinal (50 -60%): o nausea/vomiting o colicky abdominal pain • Respiratory (20 -30%): o acute rhinoconjunctivitis o laryngeal oedema o acute bronchospasm / wheezing
Ig. E-mediated food allergy Within minutes of ingestions • Anaplyhlaxis o skin and mucosa o respiratory/GI symptoms o fall in blood pressure o organ dysfunction symptoms o shock • Skin (50 -60%): o angio-oedema o urticaria o pruritis Respiratory (20 -30%): o acute rhinoconjunctivitis o laryngeal oedema o acute bronchospasm / wheezing
Non-Ig. E mediated food allergy Within hours to days • Skin o atopic dermatitis o contact dermatitis o dermatitis herpetiformis • Respiratory o Heiner’s syndrome - chronic pulmonary disease - recurrent pulmonary infiltrates, anaemia, chronic cough, recurrent fever, tachypnoea, wheezing, FTT • Gastrointestinal o chronic diarrhoea o iron deficiency anaemia o colic o food refusal and poor growth o gastro-oesophageal reflux disease (GORD) o blood in stool o constipation o enterocolitis / proctocolitis / gastroenteritis o eosinophilic oesophagitis / gastroenteritis
Non-Ig. E mediated food allergy Within hours to days • Skin o atopic dermatitis o contact dermatitis o dermatitis herpetiformis • Respiratory o Heiner’s syndrome - chronic pulmonary disease - recurrent pulmonary infiltrates, anaemia, chronic cough, recurrent fever, tachypnoea, wheezing, FTT • Gastrointestinal o chronic diarrhoea o iron deficiency anaemia o colic o food refusal and poor growth o gastro-oesophageal reflux disease (GORD) o blood in stool o constipation o enterocolitis / proctocolitis / gastroenteritis o eosinophilic oesophagitis / gastroenteritis
Non-Ig. E mediated food allergy Within hours to days • Skin o atopic dermatitis o contact dermatitis o dermatitis herpetiformis • Respiratory o Heiner’s syndrome - chronic pulmonary disease - recurrent pulmonary infiltrates, anaemia, chronic cough, recurrent fever, tachypnoea, wheezing, FTT • Gastrointestinal o chronic diarrhoea o iron deficiency anaemia o abdominal colic o food refusal and poor growth o gastro-oesophageal reflux disease (GORD) o blood in stool o constipation o enterocolitis / proctocolitis / gastroenteritis o eosinophilic oesophagitis / gastroenteritis
Eczema
Triggers for Eczema Dander, HDM Eczema Triggers Foods
Typical sites eczema Common Sitesofof Eczema
Diagnosis: skin prick testing • For Ig. E-mediated • Only conduct in areas set up to deal with anaphylaxis • A positive response a wheal diameter ≥ 3 mm of negative control • Positive predictive accuracies < 50% • Negative predictive accuracies > 95%
Serum specific Ig. E • Fluorescence enzyme immunoassay – Immuno. CAP assay
Diagnosis: oral food challenge (OFC) • The most valuable diagnostic tool for confirming suspected food allergy • Types:
Oral milk challenge
Managing anaphylaxis Symptoms Mild Urticaria Severe Treatment None Antihistamine Mild Angioedema Steroids + Antihistamines Severe Laryngeal Oedema Respiratory Distress Hypotension Shock Cardiac Arrest ADRENALINE +Antihistamines + Steroids +/- IV Fluids +/- Oxygen +/- Inotropes +/- Intubation +/- CPR
Management of food allergy • Dietary elimination and avoidance of protein allergen regardless of the clinical type – oral, inhalant or contact route • Nutritionally safe and balanced diet • Education • Pharmacotherapy • Immunotherapy (future)
Self-injectableare adrenaline Medications Crucial v A previous severe allergic reaction v. To be given immediately for serious reaction v Fast acting, will revert symptoms of lifethreatening reactions
Eczema. Treatment treatment Eczema The goals are: • To control or prevent itching • To reduce or prevent inflammation • To prevent worsening of the condition • To clear secondary infection • To keep the skin well hydrated
Thank You