Approach to Radiculopathy David C Preston MD Professor







 • Weakness (mild or not")





 – Granulomatous tissue (e.")


























- Slides: 56
Approach to Radiculopathy David C Preston MD Professor of Neurology University Hospitals of Cleveland Case Western Reserve University
ra·dic·u·lop·a·thy : any pathological condition of the nerve roots
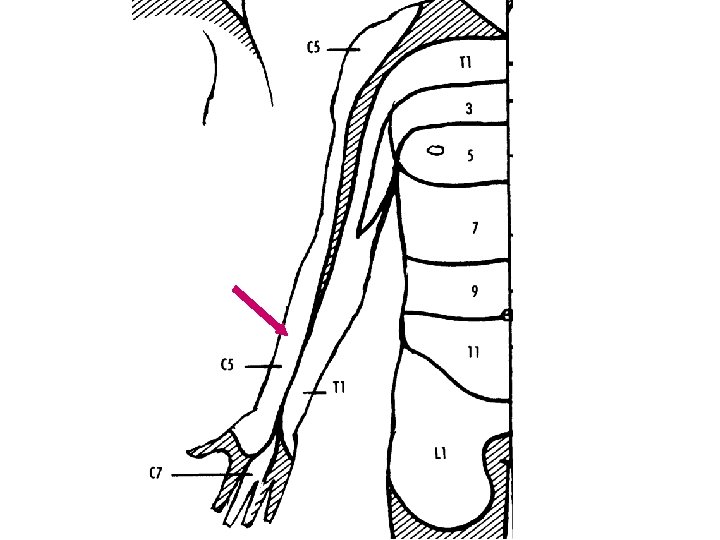
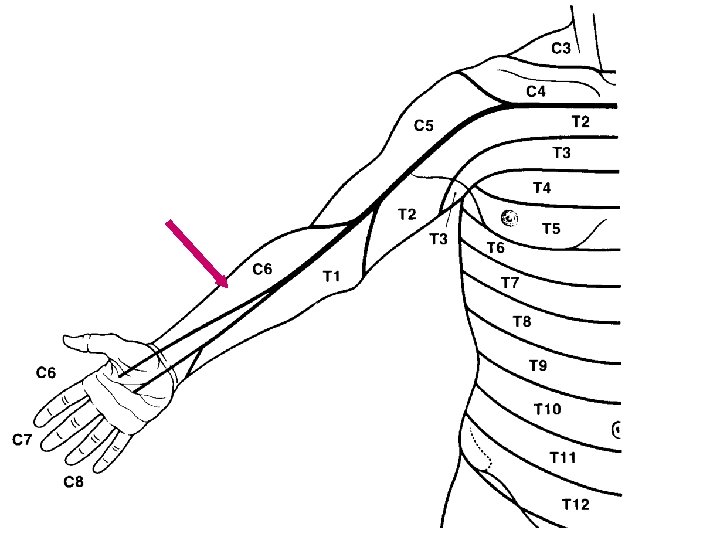
Dermatome Each nerve root supplies cutaneous sensation to a specific area of skin, known as a dermatome
Dermatome Each dermatome overlaps widely with adjacent dermatomes. Consequently, it is very unusual for a patient with an isolated radiculopathy to develop a severe or dense sensory disturbance. Dense numbness is usually more indicative of a peripheral nerve lesion than a radiculopathy. In a patient with radiculopathy, sensory loss is more often vague, poorly defined, or absent, despite the presence of paresthesias
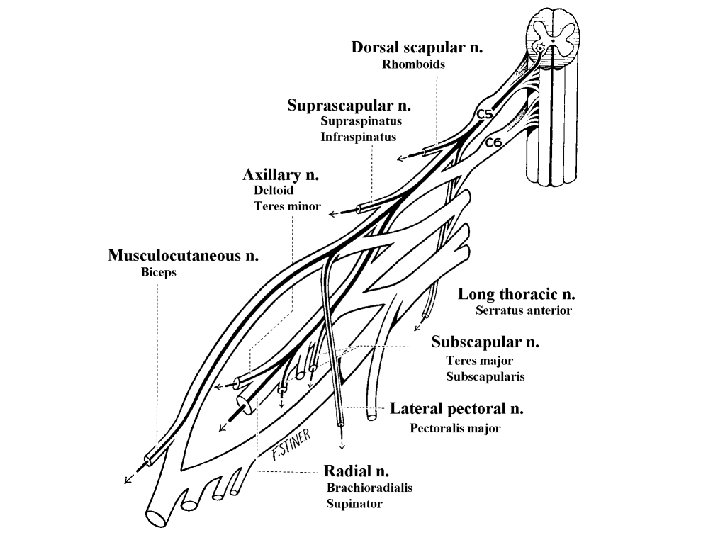
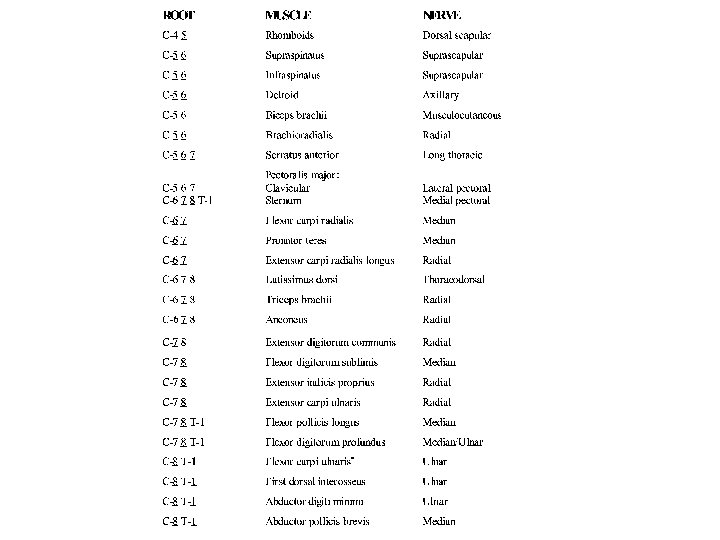
Myotome Each nerve root supplies motor innervation to certain muscles, known as a myotome
Myotome There is a wide overlap of myotomes. Indeed, nearly every muscle is innervated by at least two if not three myotomes (i. e. , nerve roots). For instance, the triceps brachii muscle, predominantly a C 7 -innervated muscle, also receives some innervation from the C 6 and C 8 nerve roots. Consequently, paralysis of a muscle is very unusual in an isolated radiculopathy. Even in the case of a severe or complete C 7 radiculopathy, the triceps brachii will become weak, but not paralyzed, retaining some strength from its partial C 6 and C 8 innervation.
Radiculopathy: Clinical • Pain and paresthesias radiating in the distribution of a nerve root, often associated with sensory loss and paraspinal muscle spasm
Radiculopathy: Clinical • Sensory loss (vague or ill defined) • Weakness (mild or not present) • Reflex Change – C 5/6 biceps/brachioradialis – C 7 triceps (also C 6>C 8) – L 3/4 knee – S 1 ankle
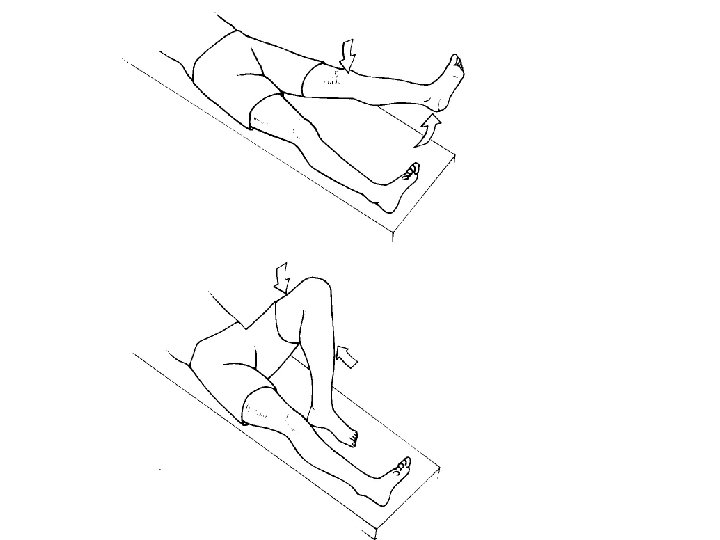
Radiculopathy: Provocative Maneuvers • Valsalva • Spurling’s Sign • Straight Leg Raising
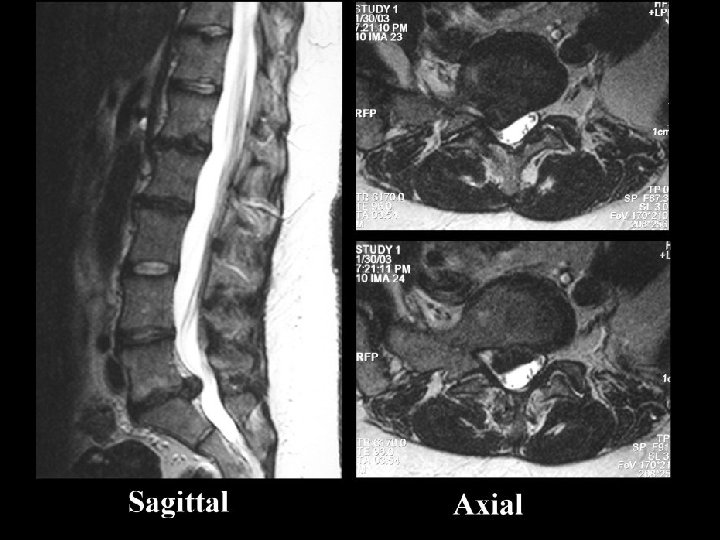
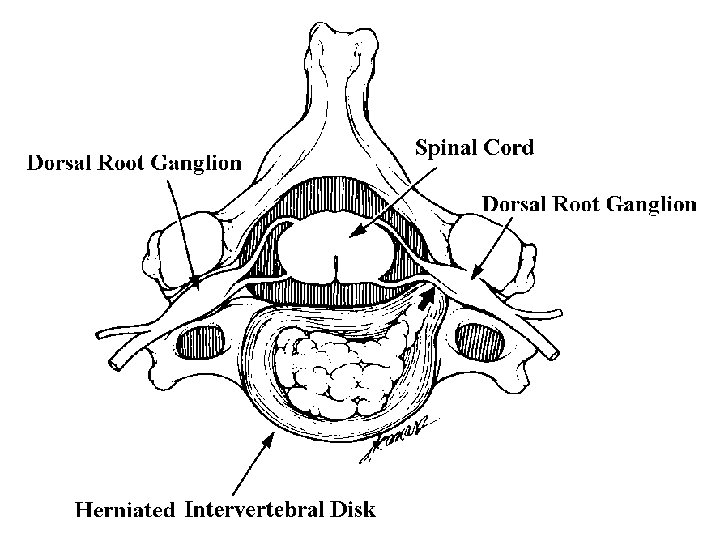
Radiculopathy: Etiology • Structural – Disk – Spondylosis – Tumor – Abscess – Hematoma
Radiculopathy: Etiology • Non-Structural – Tumor (carcinomatous or lymphomatous meningitis) – Granulomatous tissue (e. g. , sarcoid) – Infection (e. g. , Lyme disease, herpes zoster, cytomegalovirus, herpes simplex). – Acquired demyelinating neuropathy – Infarction • Vasculitic neuropathy • Diabetic polyradiculopathy
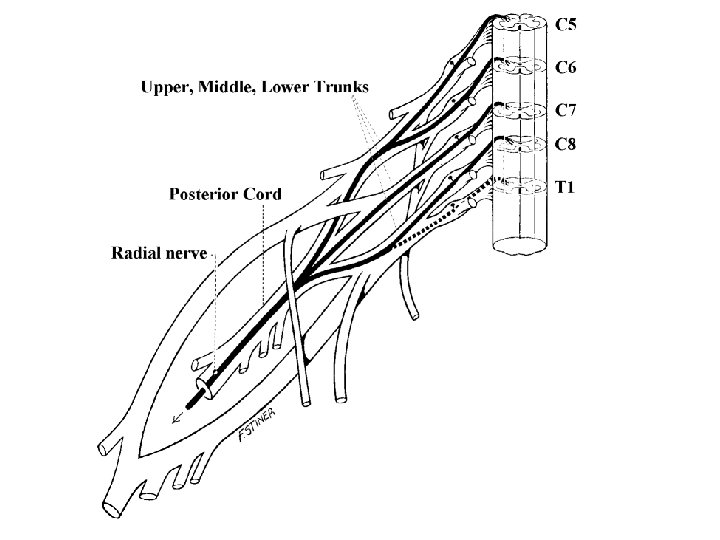
Differential Diagnosis • Root vs Plexus – C 5/6 vs Upper Trunk – C 8 vs Lower Trunk – L 3/4 vs Lumbar Plexus – L 5/S 1 vs Sacral Plexus
Differential Diagnosis • Root vs Entrapment – C 6/7 vs CTS – C 8 vs UNE – L 3/4 vs Femoral – L 5 vs Peroneal at the Knee
Electrophysiologic Evaluation In patients with radiculopathy, nerve conduction studies are typically normal, and the electrodiagnosis is established on needle EMG
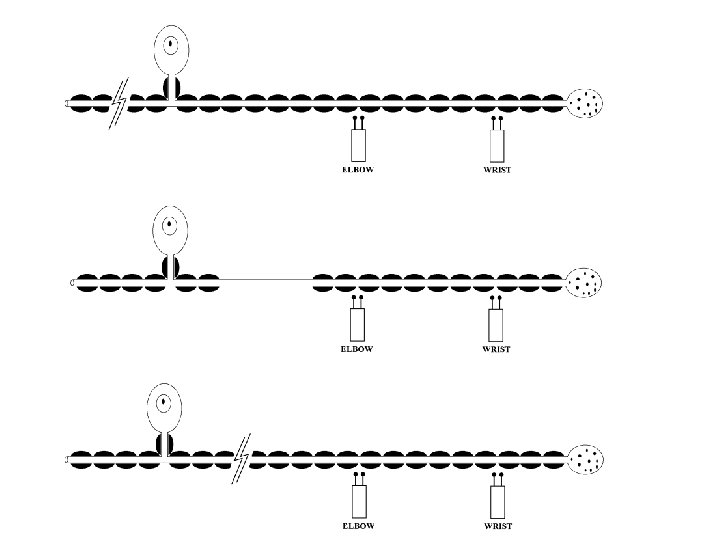
Motor Studies • Generally normal unless: – In the distribution of the root loss and associated with axonal loss • Median and ulnar with C 8 • Peroneal with L 5 • Tibial with S 1
F Responses and H reflex • Generally normal unless: – In the distribution of the root loss, and multiple roots • • Median and ulnar with C 8 Peroneal with L 5 Tibial with S 1 H Reflex only with S 1 – Cannot differentiate plexus from root – Usually need to compare side to side
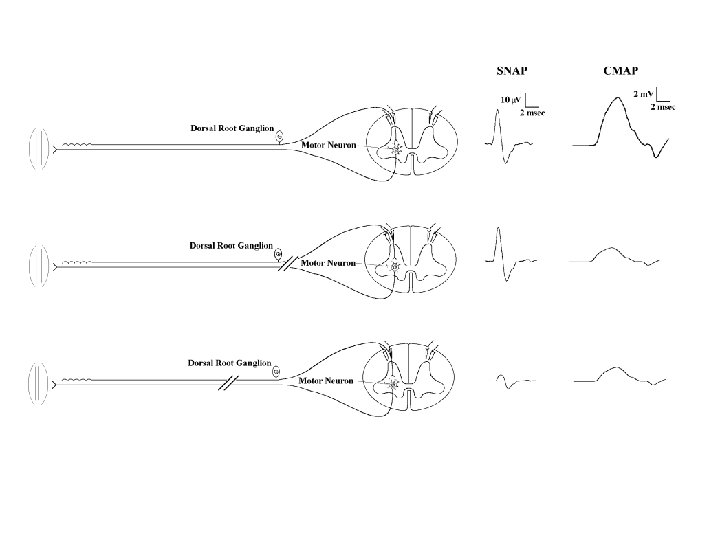
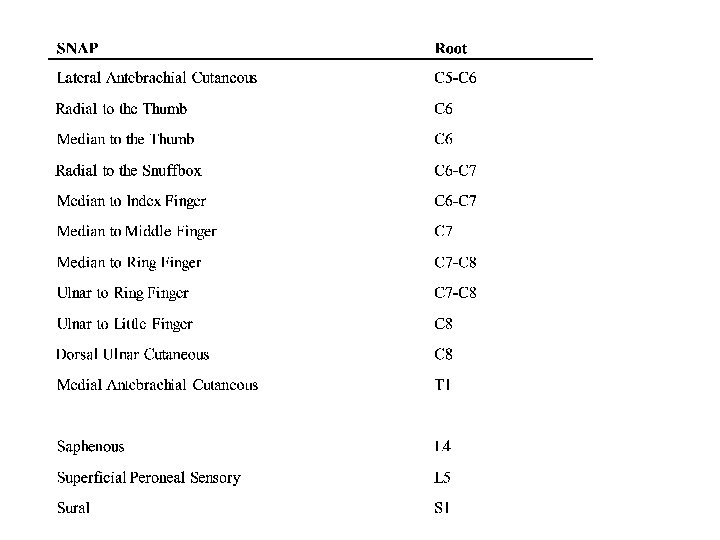
Sensory Studies • NORMAL !!! • Caution: Co-existent conditions
Sensory Studies • It is always imperative to check the SNAP that is in the distribution of the sensory symptoms
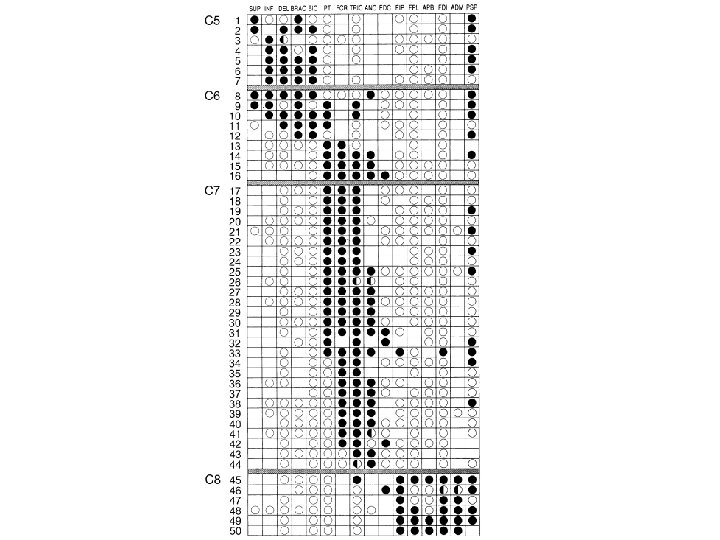
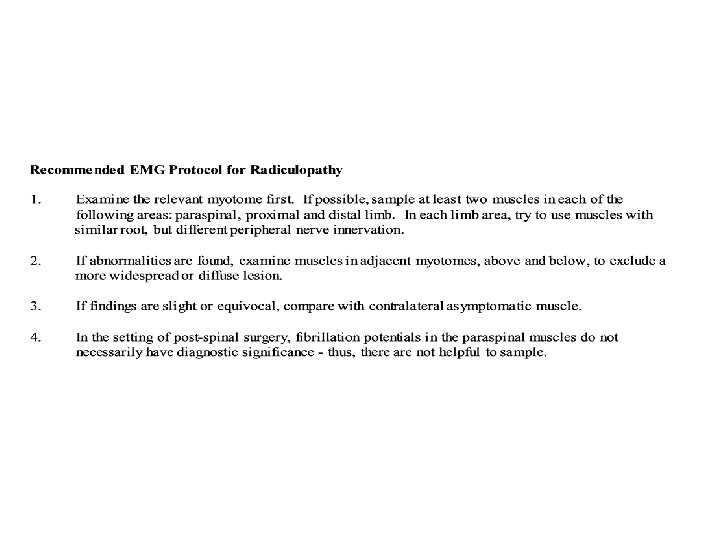
Needle EMG • The needle EMG strategy in radiculopathy is straightforward: distal, proximal, and paraspinal muscles in the symptomatic extremity are sampled, looking for abnormalities in a myotomal pattern that are beyond the distribution of any one nerve.
Needle EMG • Muscles innervated by the same myotome but by different nerves must be sampled to exclude a mononeuropathy. • Proximal and distal muscles that are innervated by the same myotome should be sampled to exclude a distal-toproximal pattern of abnormalities such as occurs in polyneuropathy. • Muscles innervated by myotomes above and below the suspected lesion level must be sampled to exclude a more widespread or diffuse process. • The paraspinal muscles should be examined.
Time Course of EMG Changes • Acute: decreased recruitment of MUAPs in clinically weak muscles • Day 10 -14: fibrillation potentials and positive waves n the paraspinal muscles • Week 2 -3 similar changes in the proximal muscles • Week 3 -4 similar changes in the distal muscles • Week 5 -6 similar changes in the foot muscles • > Several weeks – reinnervation, first satellites/increased polyphasia then long duration and high amplitude. • Chronic State: Reinnervated motor units with no active denervation
Limitations of the Needle EMG in Radiculopathy • It May Be Difficult to Localize a Radiculopathy to a Single Root Level
Limitations of the Needle EMG in Radiculopathy • The Lesion Is Acute, the EMG Study May Be Normal
Limitations of the Needle EMG in Radiculopathy • If the Sensory Nerve Root Is Predominantly Affected, the Study Will Be Normal.
Limitations of the Needle EMG in Radiculopathy • Different Fascicles May Be Preferentially Affected or Spared • Thus, if the index of suspicion is high – the more muscle checked, the higher yield
Limitations of the Needle EMG in Radiculopathy • Abnormal Paraspinal Muscles Are Useful in Identifying a Radiculopathy, but Not the Segmental Level of the Lesion
Limitations of the Needle EMG in Radiculopathy • The Paraspinal Muscles May Be Normal
Limitations of the Needle EMG in Radiculopathy • There Is No Difference on the EMG Study Between: – Radiculopathy and Focal Motor Neuron Disease – Polyradiculopathy and Diffuse Motor Neuron Disease
Limitations of the Needle EMG in Radiculopathy • Fibrillation Potentials May Persist in the Paraspinal Muscles after Spinal Surgery. • Thus, do not check the paraspinals in patients s/p surgery – they are not helpful
Limitations of the Needle EMG in Radiculopathy • Only the Distal Muscles May Be Abnormal in Radiculopathy
Limitations of the Needle EMG in Radiculopathy • There May Be Few or No Electromyographic Abnormalities in Spinal Stenosis.
Limitations of the Needle EMG in Radiculopathy • Fibrillation Potentials in the Paraspinal Muscles Do Not Necessarily Imply Radiculopathy.
Limitations of the Needle EMG in Radiculopathy • In the Elderly, It May Not Be Possible to Differentiate a Mild Chronic Distal Polyneuropathy from Mild Chronic Bilateral L 5 -S 1 Radiculopathies
Limitations of the Needle EMG in Radiculopathy • Sural and superficial peroneal SNAPs are just at the lower limits of normal in amplitude. • Peroneal and tibial CMAP amplitudes are slightly reduced with mildly slowed conduction velocities, although still in the range of axonal loss. • Peroneal and tibial F responses and H reflexes are slightly prolonged. • Denervation/reinnervation changes are present in the distal leg muscles. • Nerve conduction study and EMG findings are normal in the upper extremities.