Head Injury Sports Medicine Management Concussion Evaluation Bellwork

Head Injury Sports Medicine Management Concussion Evaluation

Bellwork Think of a time when you or someone you knew had a head injury? If it has never happened, think of a time when you saw a head injury on TV or in a movie? What happened and what did you feel when this head injury happened? Be ready to share any symptoms that you remember from that injury? Do you remember the treatment or recovery of that injury?

Today’s Objectives Student will be able to: 1. 2. 3. 4. 5. 6. Define terminology Identify a head injury Assess a head injury Treat a head injury Videos of head injury scenarios Discuss Current Events

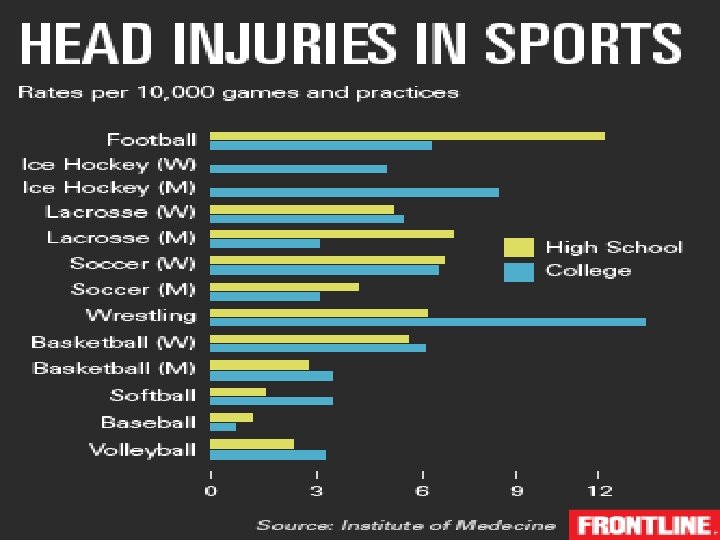
Head Injuries: Most common cause of catastrophic sports injuries. Sports with the highest incidence of head injuries are; Football Boxing Ice hockey

Graphic Organizer Fill in the vocab word as they are explained during class on the following pages

B. Terminology Cerebral Concussion __________- characterized by immediate and temporary impairment of neural function such as alteration of consciousness, disturbance of vision or equilibrium caused by mechanical forces. v Leading cause of athletic death v Most frequent type of head injury in sports v 20% of high school football payers sustain a concussion over a single season v National Football Head/Neck Injury Registry, Talley of the FB injuries annually Avg. per yr: 250, 000 concussions 8 deaths 7 quads 45 cervical fractures

Contusion 2. Cerebral ________ 3. 4. 5. - implies “bruising” of the brain, involves bleeding of the brain tissue Hemorrhage __________– is bleeding or pooling of blood between the tissue layers covering the brain or inside the brain Fracture ______– a crack or break in the skull Contracoup _______– occurring on the opposite side. An injury to the brain located on the side opposite that of the primary injury.

Mechanism of Injury

Cerebrospinal 6. _________– 7. 8. fluid which completely surround and suspends the brain. The main function is cushioning, to diminish the transmission of shocking forces Tinnitus _____– ringing in the ears Nystagmus – dancing eyes _____

Anterograde Amnesia 10. _________ – unable to recall events occurring immediately after trauma Retrograde Amnesia 11. _________ – unable to recall events occurring immediately before trauma Post-Traumatic Amnesia 12. __________– Unable to recall events that have occurred since the time of injury PEARL _____ – pupils equal and reactive to light 13.
 14. ____________– “knocked out” Asymptomatic 15. _______– (No Signs or")
Loss of Consciousness (LOC) 14. ____________– “knocked out” Asymptomatic 15. _______– (No Signs or Symptoms) no headache, no dizziness, no impaired orientation, concentration, or memory, during rest or. Post execration Concussion Syndrome 16. ____________– reflects alter neurotransmitter function, rapid processing and recall of new information is the most impaired Rhomberg’s Test function 10. _______ - a test for balance and coordination. Stand with feet together and head tilted back. Positive test = swaying

Second Impact Syndrome 18. ___________ – acute, usually fatal, brain swelling that occurs when a second concussion is sustained before complete recovery from a previous concussion. Causes vascular congestion and increased intracranial pressure which may be difficult or impossible to control ü Effects of head trauma are cumulative ü Chance of second impact is 4 X greater ü

Arrival Assessment What you should observe as you are approaching the downed athlete Are they moving? Limbs? Eyes? Body position? Rigidity? Prone? Level Supine? Neck angle? of consciousness: Unconscious and not breathing Unconscious and breathing Conscious

On Field Assessment When you get to the athlete: › › › One immediately stabilizes the head, while another performs the evaluation Check ABC’s- begin CPR? AED? Determine level of consciousness (LOC) If unconsc and not breathing- begin CPR/ AED If unconsc and breathing- treat as if a neck fx If consc- continue with eval › Check ears and nose- presence of CSF

On Field Assessment If they’re conscious and moving their limbs as you are approaching, should you still immediately stabilize the head and neck? If they’re conscious and you stabilize the head and neck, how long should you continue to stabilize? If they are unconscious ALWAYS treat like a cervical fracture with head trauma
? Any unusual sensations? Pain,")
HIPS Evaluation History Mechanism- how they got hurt, Previous concussion(s)? Any unusual sensations? Pain, numbness? Can they move their hands and feet? Headache, nausea, blurred vision, tinnitus? Where is pain located? Head, neck?

Signs and Symptoms of a Concussion › › › › Headache Balance problems Dizziness Concentration difficulties Loss of consciousness (LOC) Lightheadedness Delayed motor/ verbal response Memory Loss › › › › › Disorientation Amnesia Blurred vision Vacant stare Photophobia Tinnitus Nausea Vomiting Emotionality Slurred speech

HIPS Evaluation Inspection › Working with these athletes daily give you the advantage, because you know how each person NORMALLY acts and what their normal personality is. › Visual inspection of athletes disturbances in coordination, orientation, attention, emotional response, verbal and motor response, and physical deformity such as swelling, bleeding, fluid from ears or nose… etc.

HIPS Evaluation Make sure the following have been checked: Otorrhea, rhinorhea, Battle’s sign, Halo test raccoon eyes, hyphema, nystagmus= 911 If any of these are observed, call 911!!

Pupillary Response

Nystagmus

Ottorrhea

Basal Skull Fracture

Battle’s Sign

Racoon Eyes

Hyphema

Subconjunctival Hemorrhage

HIPS Evaluation Palpation › › Skull- feel for tenderness, depressions Cervical spine- pain over the spinous processes? ( middle of neck) Sensation in extremities? This is point in which you completely rule out a cervical fracture

HIPS Evaluation Special Tests › Memory Check- retrograde, anterograde amnesia Anterograde amnesia- after the brain injury Example: Remember these three words…. Have athlete repeat words back to you every five minutes Retrograde amnesia- before the brain injury Example: What team are you playing? Presence of sustained (>30 minutes) antero amnesia = 911 Keep asking questions- date, location, who scored last point, what they ate for breakfast… etc.
")
HIPS Evaluation Special Tests Continued Balance/ coordination Rhomberg’s test Heel to toe walking (Trendelenburg) Reflexes L 4 - L 5 Patellar tendon reflex PEARL S 1 - S 2 Achilles tendon reflex

HIPS Evaluation Special Tests Continued Cognitive Functioning Serial 7’s (Count backwards from 100 by 7) Months Backwards (Dec, Nov, …) Alphabet Backwards (Z, Y, X, W, V, U…) Halo Test- for presence of CSF

Other Cognitive Options May have the athlete go over plays with a teammate/coach This will give you feedback if the athlete is thinking clearly

SCAT 5 Look at the SCAT 5 handout and follow along with explanation

SCAT 5 Demonstration

Partner A turn to partner B. Assess your partner using the SCAT 3 Switch roles and repeat the process. PROPERTY OF PIMA COUNTY JTED, 2010 36

HIPS Evaluation Cranial Nerve Assessment › › › Cranial Nerves 1 -12 Both sensory and motor Need to be rechecked every 20 minutes until severity of trauma is established

# Cranial Nerve Name 1. I Olfactory 2. II Optic 3. III Occulomotor 4. IV Trochlear 5. V Trigeminal 6. VI Abducens 7. VII Facial 8. VIII Auditory 9. IX Glossopharyngeal 10. X Vagus 11. XI Accessory 12. XII Hypoglossal

Cranial Nerve What action tests each nerve I- Olfactory Ask if they can smell ammonia salts, tuft skin, perfume…. Etc. II- Optic Ask athlete to read the score board, look at cars in the distance III- Occulomotor PEARL IV- Trochlear Roll their eyes, follow your finger downward and inward V-Trigeminal Bite down, clench jaw, sensation in cheeks VI- Abducens Follow your finger outward VII- Facial Raise eyebrows, smile, frown VIII- Auditory Close eyes balance on both legs, balance one leg, close eyes balance on one leg, heel to toe walking, finger to nose IX-Glossopharyngeal Swallowing X- Vagus Stick out tongue and say “ahhhh” XI- Accessory Resist the athlete doing a shoulder shrug XII-Hypoglossal Stick out tongue and wiggle it around

Dangerous Concussions Epidural Hematoma Sits outside of duramater in between skull Symptoms occur in first 24 hours but up 72 hours Signs and Symptoms include: Pupils unreactive, Rapid shallow breathing, very drowsy, weakness in arms and legs and may have some paralysis, amnesia, possible convulsions, nausea and vomiting, severe headache Treatment Doctor ASAP

Very Dangerous Concussion Subdural Hematoma: Collection of blood between the dura and the arachnoid space of the brain Commonly delayed onset of symptoms (2 days- 2 weeks) High Signs mortality rate and Symptoms: LOC, irritability, seizures, numbness, headache, dizziness, disorientation, amnesia, weakness, nausea, vomiting, personality changes, inability to speak, slurred speech, difficulty walking, blurred vision, deviated gaze or abnormal movement of eyes

Consequences of returning to athletic participation too soon Second Impact Syndrome › › Deadly!! Can take only minor blow the second time to create life threatening situation Loss of auto regulation of the brain’s blood supply; vascular engorgement in the cranium; increased intracranial pressure; the second blow bursts the engorged area Death in nearly 50% of all cases, disability in almost 100% of all cases… 911… maintain vitals if possible THIS IS WHY WE TREAT ALL CONCUSSIONS CONSERVATIVELY

Preston Plevretes Second Impact Syndrome- Second Impact Syndrome happened to young man while in freshman year of college during football game Sustained initial injury 4 days before 2 nd injury Four and a half years later, Plevretes struggles to walk and talk and needs round-the-clock care ALL BECAUSE CONCUSSION WENT UNDIAGNOSED!!! http: //sports. espn. go. com/espn/e 60/news/story? id=5162747

Snapshot Write a “snapshot” of today’s learning in 25 words or less. PROPERTY OF PIMA COUNTY JTED, 2010

Whewww…. Questions? Comments? Concerns? A lot of information to digest…. . But with repetition and practice, it will become MUCH easier to understand What are the current events regarding concussions?
- Slides: 45