Women Heart Disease WHATS THE SCOOP Grace Grau



 Disease ▪ 801, 000 deaths in U. S.")













 Acute Prodromal ▪ Precede acute presentation ▪ Anginal Equivalent")






 ▪ Non obstructive ▪ Common in younger women ▪")
 STEMI (mortality 10 -15 %) ▪ Arrhythmias")


 ▪ Aspirin ▪")










- Slides: 41
Women & Heart Disease: WHAT’S THE SCOOP? Grace Grau, DNP, ACNP-BC, CRNP, AACC
Conflicts of Interest NONE
Objectives: Upon Completion, participants will be able to: ▪ Discuss the current state of the science of Ischemic Heart Disease in women ▪ Highlight important aspects of the patient history in risk stratification ▪ Differentiate between acute and prodromal symptoms of cardiac ischemia typical in women ▪ Discuss current diagnostic and treatment strategies specific to women ▪ Discuss the role of the interdisciplinary team in prompt recognition of ischemia in women ▪ Incorporate knowledge into practice to optimize health outcomes for this vulnerable population
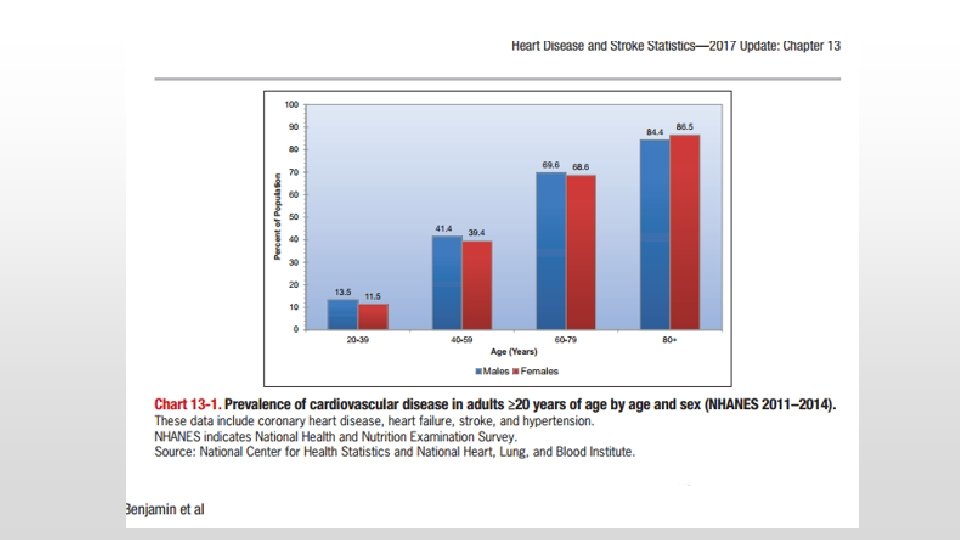
State of the Science: Cardiovascular (CVD) Disease ▪ 801, 000 deaths in U. S. Coronary Heart Disease C V D Heart Failure ▪ Average 1 death q 40 seconds ▪ 92 million American Adults have CVD ▪ Cost estimated at > $316 billion Stroke Hypertension Others:
CVD the #1 Killer of Women ▪ More deadly than all forms of cancer combined ▪ 1 in 3 women die of heart disease each year ▪ Kills 1 woman every 80 seconds ▪ Affects about 43 million women in the US American Heart Association: Heart Statistics at a Glance
Terminology for Coronary Ischemia ▪ ACS-Acute Coronary Syndrome ▪ MI- Myocardial Infarction aka Heart Attack aka ▪ Silent MI- Without recognized symptoms ▪ STEMI- results from complete blockage of blood flow greatest risk of immediate death ▪ NSTEMI- partial obstruction reduces blood flow risk of death http: //www. heart. org/HEARTORG/Professional/Mission-Lifeline/Mission. Lifeline-Heart-Attack 101_UCM_314000_Article. jsp#. WNMk. VW_yu 5 s
Risk Factors for Heart Disease: ▪ Age / gender ▪ Hypertension ▪ Family history of early onset CHD ▪ Smoking ▪ Diabetes ▪ Obesity ▪ Cholesterol ▪ Poor diet ▪ Sedentary lifestyle American Heart Association
2 growing epidemics are greatly contributing to the increasing risk of CVD Obesity and Diabetes CDC, 2017
CVD in Women differs From Men ▪ Clinical Presentation ▪ Pathophysiology ▪ Prognosis https: //www. youtube. com/watch? v=t 7 wm. PWTn. Db. E
It isn’t just a Man’s Disease! ▪ Since 1984, more women than men have died each year from heart disease ▪ 26% of women age 45 and older who have an initial recognized heart attack die within a year compared with 19% of men. ▪ Heart Disease lags behind about 10 -15 years for women, possibly contributing to these statistics ▪ Only 24% of participants in all heart -related studies are women American Heart Association
Add a Slide Title - 2
Symptoms are often different for women and sometimes overlooked or misunderstood. Why do so many women die of Heart Disease?
Case Study 85 YOWF with remote hx. of tobacco use, widowed X 2 months. She c/o 5 week hx. of progressive weakness. She was a marathon runner up until 2 years ago. B/P 149/88, 66, 18, Afebrile, O 2 Sat 94 RA Allergies to shellfish (hives) Meds: Atorvastatin 20 mg PO QHS Metoprolol 5 mg PO daily Glyburide 2. 5 mg PO daily PMHx. HTN, Dyslipidemia, DM T 2 SHx. Carotid endarterectomy What else would you want to know as part of your triage assessment?
Heart Attack Also known as: Causes ▪ Atherosclerosis ▪ Myocardial Infarction ▪ STEMI ▪ NSTEMI ▪ Coronary Spasms ▪ Endothelial Dysfunction ▪ Acute Coronary Syndrome ▪ Silent MI https: //www. nhlbi. nih. gov/healthtopics/cmd/trials Decrease perfusion to myocardium Ischemia Necrosis
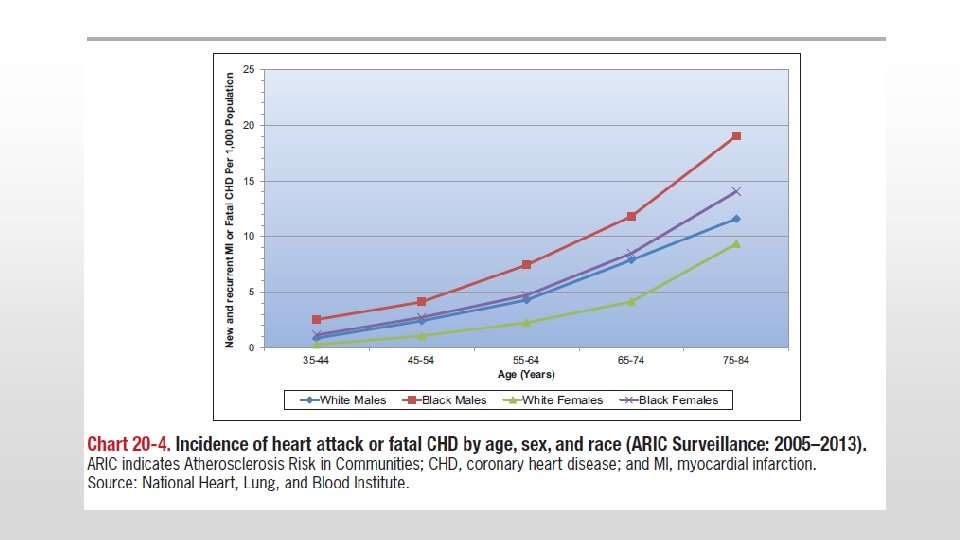
Statistics Hispanic Women African American women • Are likely to develop heart disease 10 years earlier than Caucasian women. ▪ Only 36% of African American women know that heart disease is their greatest health risk. • Only 34% of Hispanic women know that heart disease is their greatest health risk. • 48. 3% aged 20 and over have cardiovascular disease. • Hispanic women are least likely to have a usual source of health medical care and • Only 14% believe that cardiovascular disease is their greatest health problem. • Only 1 in 8 say that their doctor has ever discussed their risk for heart disease. • Only about 50% of African-American women are aware of the signs and symptoms of a heart attack. American Heart Association (2017). Heart Statistics at a glance.
Cardiac Ischemia in Women (Symptoms) Acute Prodromal ▪ Precede acute presentation ▪ Anginal Equivalent Weakness Fatigue http: //www. heart. org/idc/groups/heartpublic/@wcm/@hcm/documents/downloadable/ucm_488240. pdf ▪ weakness ▪ fatigue and ▪ shortness of breath Mc. Sweeney et al. , 2010; O’Keefe. Mc. Carthy, 2008; Redberg, 2010.
Women’s Symptoms: 1. Unusual Fatigue- 70% 2. Sleep disturbance- 48% 3. Shortness of breath- 42% 4. Indigestion- 39% 5. Anxiety- 35% 6. Chest discomfort- 30% (43% without chest pain during heart attack) Circulation, 2003, 108: 2619 -2613
Case Study 35 YOBF presents with c/o n/v since last night, and profound fatigue. She works as a waitress at a busy café. Vital signs are 110/64, HR 98, RR 17, Afebrile. She is accompanied by her daughter who appears concerned. She is a non smoker. NKDA Meds: Vitamins PMHx: None Surgical hx. Cesarian section X 2, tonsillectomy What else would you want to know as part of your assessment?
STEMI
Prinzmetal Angina ▪ CP at rest ▪ Common in women ▪ Associated with transient ST segment elevation ▪ Secondary to coronary spasms ▪ Diagnosis of exclusion
NSTEMI ▪ Partial occlusion of a major coronary artery or ▪ Complete occlusion of a minor coronary artery Rupture or Erosion of plaque Ischemia-> Necrosis http: //nstemi. org/
NSTEMI- EKG changes http: //nstemi. org/
Coronary Syndrome X (Microvascular Disease) ▪ Non obstructive ▪ Common in younger women ▪ Risk factors same as for obstructive heart disease ▪ S&S ▪ shortness of breath ▪ Discomfort in left arm, jaw, neck, back or abdomen associated with chest pain ▪ sleep problems ▪ fatigue ▪ lack of energy American Heart Association (2015). Coronary Microvascular Disease. Retrieved from http: //www. heart. org/HEARTORG/Conditions/Heart. Attack/Diagnosinga. Heart. Attack/Coronary-Microvascular-Disease. MVD_UCM_450320_Article. jsp#. WNNLl. G 8 r. K 5 s
Post MI Complications NSTEMI (mortality 3 -5%) STEMI (mortality 10 -15 %) ▪ Arrhythmias ▪ Acute Heart Failure(R/L) ▪ Cardiogenic Shock ▪ Mitral Regurgitation (MR) ▪ Pericarditis ▪ Embolism ▪ Severe MR, Tamponade http: //nstemi. org/ ▪ Aneurysm
Women ▪ Experience delays to diagnosis & treatment ▪ Heart attack in the absence of Chest Pain Circulation, 2005, 111: 940 -953
Diagnostic Strategies ▪ ECG ▪ Serial cardiac enzymes ▪ Stress test with Imaging (nuclear or ultrasound) ▪ Coronary angiogram ▪ Positron emission tomography (PET Scan) ▪ CT or CT angiography ▪ Cardiac MRI ▪ Endothelial dysfunction test Mayo Clinic. (2017). Small vessel disease. Retrieved from http: //www. mayoclinic. org/diseases-conditions/small-vesseldisease/diagnosis-treatment/txc-20198391
Treatment Strategies Traditional Alternative Medicines ▪ Nitroglycerin ▪ L-argine (Amino Acid) ▪ Aspirin ▪ Anticoagulants ▪ Statins ▪ CCB ▪ BB ▪ ACE-I ▪ ARBS ▪ Ranolazine
Case Study 65 YO Hispanic Female presents to the ED c/o 1 day hx. left ear ache, diaphoresis and nausea. She is a retired school teacher and lives with her husband of 40 years. VS- Afebrile, 88, 17, 138/73. O 2 sat 96% RA. NKDA Current Meds: Vitamin D, Iron Supplements PMHx. Anemia, Uterine Ca age 42 SHx. TAH at age 42 What else would you want to know as part of your triage assessment?
Cardiovascular Disease Mortality 1 in 3 die of heart disease in the United States In the face of the high number of risk factors , Alabama residents have a high CV mortality risk, and limited health resources.
Poverty Demographics and Economic Wellbeing ▪ U. S. 16% ▪ AL ▪ ▪ 19 % Extreme Poverty. Women. Poor working Families. Single parent families- 8. 4% 21% 37. 3 45%
90% of women have 1 or more risk factors for developing heart disease.
Top Health Issues National Ranking How Does Alabama Compare? ▪ Diabetes Mellitus 12. 2% ▪ Obesity 32. 3% ▪ Hypertension 33. 9% ▪ Physical Inactivity 30. 4% Gregg, S. Q. (2013, Sept 27). ▪ Estimated population in AL 4, 802, 740 (2011)
Women C/O ▪ Fatigue ▪ Unexplained SOB ▪ Indigestion ▪ Tooth Ache ▪ Upper back, Shoulder, Neck or Ear Pain ▪ Vague Chest Discomfort The Interdisciplinary Team Risk Stratification
Risk Stratification ▪ Family History OF CVD ▪ Anginal Equivalent ▪ Presence of Prodromal Symptoms ▪ Patient’s Perception of Etiology Institute CP Protocol
The Scoop ▪ As many as 98, 000 people die annually due to medical errors, including delays in diagnosis ▪ Women experience: MI in the absence of pain (43%) Non-classic symptoms => weakness, fatigue and shortness of breath Prodromal Symptoms precede acute presentation by 4 -6 weeks ▪ Assessment Guidelines stress importance of considering complaints of “other” symptoms of MI “high priority triage cases” ▪ ED Triage nurses : Are often the first health providers patients encounter Initial actions are guided by presenting complaint of chest pain Do not consider family history in risk stratification ▪ Genetic predisposition [with “heritability of coronary artery disease estimated at 40%”] is a major, non-modifiable risk factor for the development of CVD ▪ MI increases morbidity, mortality and disability, impacting individuals, an already hurting economy and contributing to rising health care costs
▪ Be Informed ▪ Review Institutional Processes ▪ Advocate ▪ Think outside the picture ▪ Share knowledge with your colleagues ▪ Dare to question Improving Health Outcomes