Spontaneous ICH in Taiwan NTUH 1993 male female





.")

, 2. Ischemic stroke evaluation, 3. Coagulopathy")


 validated the ICH score by retrospective analysis indicating")


. - Predictors: short time interval between")


- Slides: 65
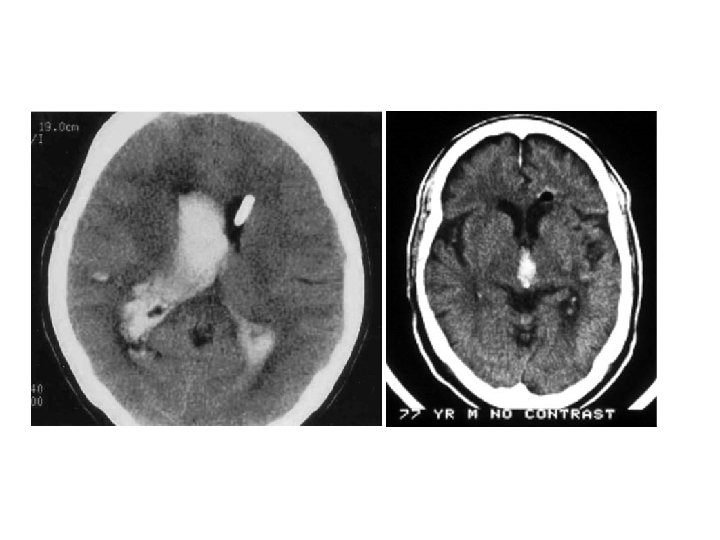
Spontaneous ICH in Taiwan, NTUH, 1993 • male/ female-- 1. 1/ 1 • prognosis-- 23 -30% death (24. 3% in patients with medical Tx. , 18. 7% in patients with medical & surgical Tx. ) • localization-- putamen 41%, thalamus 23%, combined p+t 9. 7%, subcortical area 9. 3%, brain stem 6. 5%, cerebellum 5. 9%
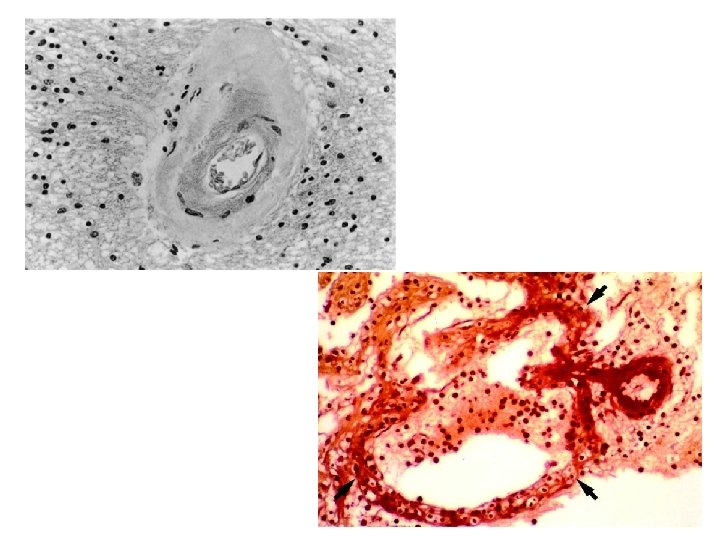
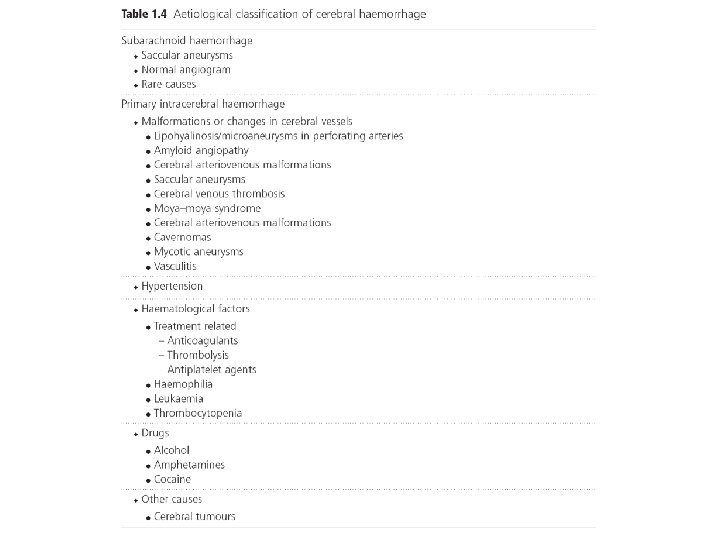
治病機轉 • • Chronic hypertension Lipohyalinosis Arterial sclerosis and fibrinoid necrosis Focal aneurysmal dilatation (Charcot. Bouchard intracerebral microaneurysm)
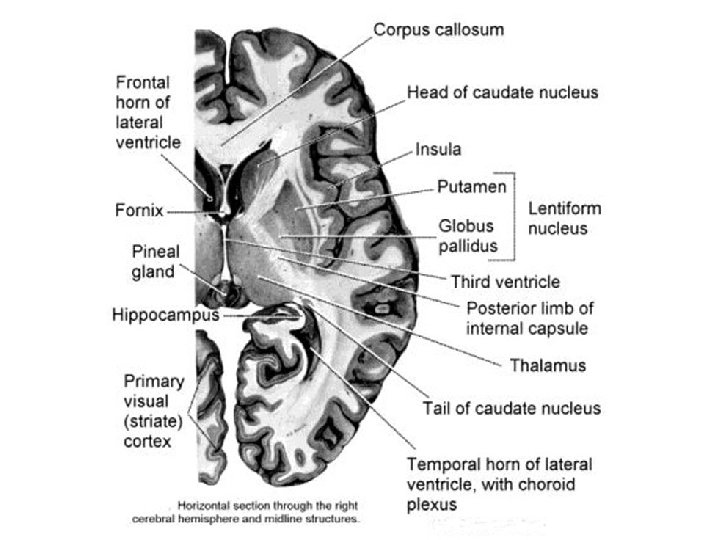
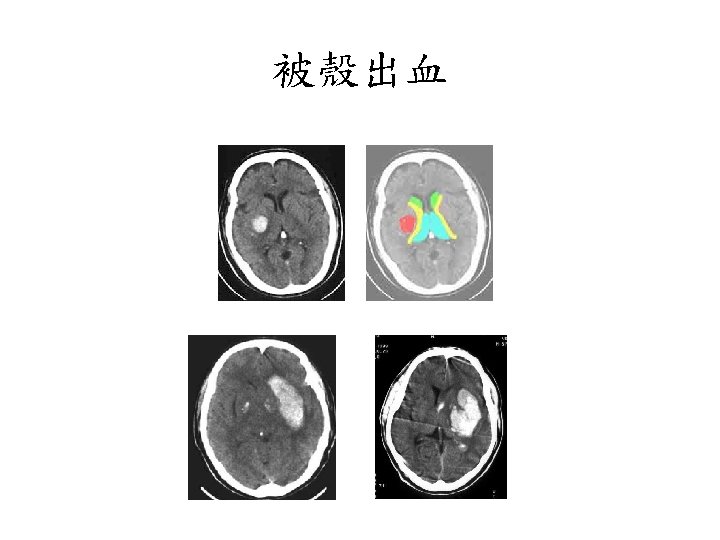
被殼出血 • • Flaccid hemiplegia Complete hemisensory deficit Homonymous hemianopsia Paralysis of conjugate gaze to the side opposite the lesion • Mild to moderate impairment of consciousness with or without headache and vomiting • Neuropsychological disorders (in some cases).
視丘出血 • similar syndromes may occur, but sensory deficit usually predominates over the other manifestations • Oculomotor signs such as forced downward gaze, convergence paralysis, and unreactive miotic pupils. • 被殼出血很大時,可以考慮手術,而視丘出血則 常常往下犯到腦幹,預後相當不好。一般比較不 考慮開刀。 • 另外,視丘非常靠近第三腦室。大部分的視丘出 血都會破到腦室裡面。這點比被殼出血常見。
Lobar Hemorrhage • 神經學表現依血塊大小及出血位置不同而 有所不同 • Contralateral hemiparesis or sensory loss, aphasia, neglect, or confusion • Headache is common, disturbance of consciousness is milder
小腦出血 • Dysequilibrium, ataxia, vertigo, nausea, and vomiting. • Brainstem dysfunction (in large hematoma).
腦幹出血 • Rapid development of coma, quadriplegia, conjugate gaze deviation opposite to the lesion or ocular bobbing, and abnormal respiration. • Small pontine hemorrhages occur more frequently than previously thought and produce milder symptoms, such as “pure motor hemiparesis” , “ataxic hemiparesis” or even “Bell’s palsy”.
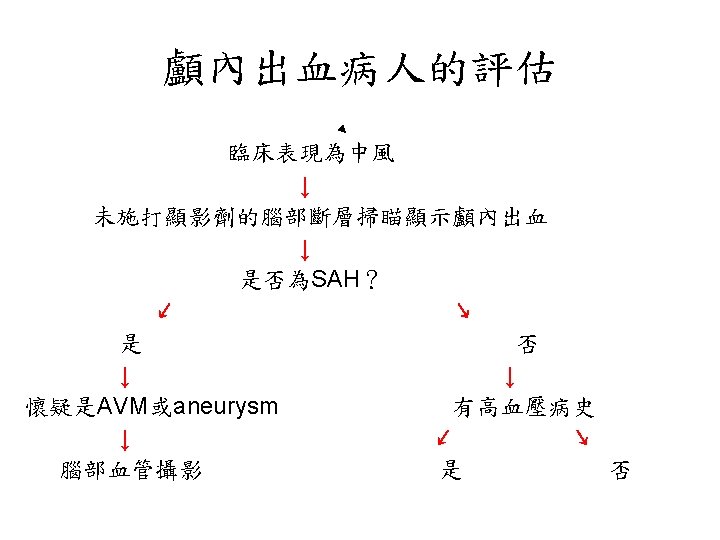
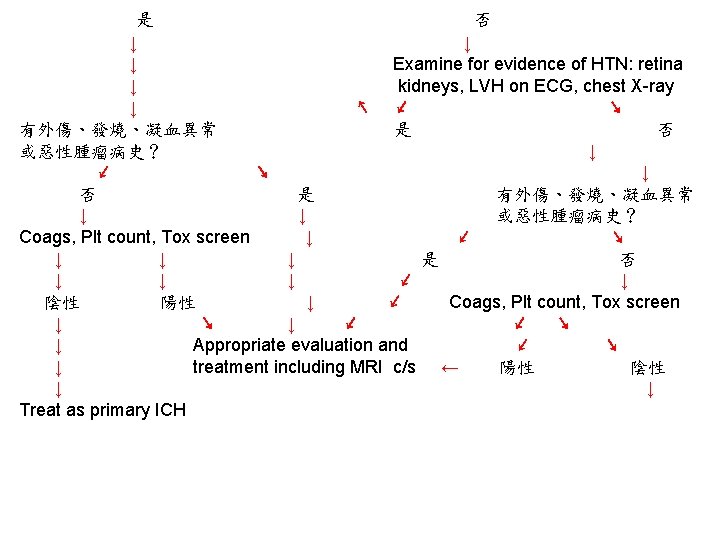
陰性 ↓ 1. Blood cultures (x 3), 2. Ischemic stroke evaluation, 3. Coagulopathy evaluation, 4. MRI c/s gadolinium, 5. Consider cerebral angiography • 血管攝影是一種侵襲性的檢查。 • 血腫的大小是評估預後最好的 具。 • Volume: estimated from CT ( A x B x C) / 2 A = the greatest diameter of hematoma B = the diameter perpendicular to A C = the thickness measured as the number of CT slices where the hematoma is visualized multiplied by slice thickness.
Hemorrhage Volume-Mortality • Volume graters 60 cm 3 – Deep-93% – Lobar-71% • Volumes 30 -60 cm 3 – Deep-60% – Lobar-60% – Cerebellar-75% • Volumes less 30 cm 3 – Deep-23% – Lobar-7% – Cerebellar-57% Broderick: Volume of ICH; Stroke Vol 24, No 7
Evaluating Intracerebral Hemorrhage • ICH score — A simple six-point clinical grading scale called the ICH score has been devised to predict mortality after ICH • The ICH score is determined as follows: – Glasgow Coma Scale (GCS) score 3 to 4 (= 2 points); GCS 5 to 12 (= 1 point) and GCS 13 to 15 (= 0 points) – ICH volume 30 cm 3 (= 1 point), ICH volume <30 cm 3 (= 0 points) – Intraventricular extension of hemorrhage present (= 1 point); absent (= 0 points) – Infratentorial origin yes (= 1 point); no (= 0 points) – Age 80 (= 1 point); <80 (= 0 points)
• Cheung et al. (2003) validated the ICH score by retrospective analysis indicating it as a better predictor of outcome than the Glasgow coma scale alone. • Thirty-day mortality rates increased steadily with ICH score; mortality rates for ICH scores of 1, 2, 3, 4, and 5 were 13, 26, 72, 97, and 100 percent, respectively. No patient with an ICH score of 0 died, and none had a score of 6 in the cohorts studied.
ICH Hemorrhage Volume • Old concept-Hemorrhage static process; bleeding complete in a minutes • New concept-Hemorrhage is dynamic; process continues for several hours
• Hematoma enlargement or hematoma growth - increase in the volume of hematoma, can occur several hours after stroke onset, frequently associated with neurologic deterioration (66%). * initial CT scan < 3 hrs (35%) * at 3 – 6 hrs (16%) * at 6 – 12 hrs (15%) * at 12 – 24 hrs (6%) - Predisposing factors: history of brain infarction; liver disease; high blood glucose ( >141 mg/dl) or Hb. A 1 C ( >5. 1%); high systolic
blood pressure ( > 200 mm Hg). - Predictors: short time interval between onset and admission; habitual alcohol consumption; consciousness disturbance; an irregularly shaped hematoma shown on initial CT scan; and low levels of fibrinogen. • Outcome - mortality rate from ICH decreased dramatically due to: * increased detection rate of milder ICH. * decrease in the prevalence of HTN. * improved antihypertensive therapy.
Hunt and Hess分級 • Grade 0 Unruptured aneurysm. • Grade 1 Asymptomatic or mild headache. • Grade 2 Moderate-severe headache, nuchal rigidity, cranial nerve deficits. • Grade 3 Confusion. Lethargy, mild focal symptoms. • Grade 4 Stupor, Hemiparesis. • Grade 5 Comatose.
低血鈉的治療 • 治療低血鈉時,特別要注意的是要避免 volume contraction,可以等張溶液靜脈給予。 • 為了監測volume status,可以central venous pressure,pulmonary capillary wedge pressure, fluid balance及體重來評估。 • 要小心與cerebral salt wasting syndrome及 SIADS作鑑別診斷。