SPECIAL SENSES Khaleel Alyahya Ph D MEd www




















 are bilateral and symmetrical cavities")










")







 q Receptors are")


 EAR q Auricle (pinna). q External acoustic canal). meatus (auditory § Narrow")
 § Air-filled, mucosa-lined cavity within the")

 EAR q Includes sense organs for hearing and balance q Bony labyrinth")




 is a benign tumour")







. § § § Stimulated")
 nares or nostrils, lead to the nasal")







. § § § Stimulated")





 are")


- Slides: 77
SPECIAL SENSES Khaleel Alyahya, Ph. D, MEd www. khaleelalyahya. net
RESOURCES q Information, tables and figures of this lecture were taken from the following books: § “Mastering Medical Terminology”. o By Sue Walker, Maryann Wood and Jenny Nicol § Essential of Human Anatomy and Physiology o Elaine Marieb and Suzanne Keller q Additional Recommended Resources: § Mosby’s Dictionary § By Mosby
SPECIAL SENSES q Special senses include: § Smell § Sight § Hearing § Taste § Touch (equilibrium) q Special sense receptors § Large, complex sensory organs § Localized clusters of receptors Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
INTRODUCTION q The five special senses are sight, hearing, smell, taste and touch. q The senses are based on receptor cells or groups of receptor cells called sense organs. q Receptors respond to stimuli in the environment and send nerve impulses along sensory neurons. q Everything we see, hear, feel, smell or taste requires billions of these nerve impulses to send messages to the brain. q The brain interprets the nerve impulses and, thus, we perceive the impulse through one of our senses. q Other than the vocabulary and the tests and procedure sections, all topics in this chapter have been divided according to the respective sense. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
THE EYE
INTRODUCTION q The primary function of the eye is to capture light rays. q 70% of all sensory receptors are in the eyes. q Each eye has over 1 million nerve fibers carrying information to the brain. q The light rays are modified into nerve impulses which are transferred to the visual cortex of the brain to be translated and interpreted into images, thereby enabling a person to see in a process that seems instantaneous. q Of the five senses, the ability to see is one of the most important to allow us to gather information about the external environment. q The eye is a very complex organ and has functions that include light perception, focusing of the light onto the retina, refraction, light accommodation, transmission of messages to the brain and Khaleel Alyahya, Ph. D,
ANATOMY OF THE EYE q Accessory structures include the: § Extrinsic eye muscles § Eyelids § Conjunctiva § Lacrimal apparatus Khaleel Alyahya, Ph. D,
EXTERNAL AND ACCESSORY STRUCTURES q Extrinsic eye muscles: § Six muscles attach to the outer surface of the eye. § Produce gross eye movements. q Tears contain: § § Dilute salt solution. Mucus. Antibodies. Lysozyme (enzyme that destroys bacteria). q Function of tears: § Cleanse, protect, moisten, lubricate the eye. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
EXTRAOCULAR MUSCLES q The extraocular muscles are located within the orbit, but are extrinsic and separate from the eyeball itself. q They act to control the movements of the eyeball and the superior eyelid. q There are seven extraocular muscles: levator palpebrae superioris superior rectus inferior rectus medial rectus lateral rectus inferior oblique superior oblique § § § § q Functionally, they can be divided into two groups: responsible for eye movement: § • Recti and oblique muscles. responsible for superior eyelid movement: § • Levator palpebrae superioris. Khaleel Alyahya, Ph. D,
EYELID & EYELASHES q The eyelids are thin, mobile folds that cover the eyeball anteriorly. q They offer protection from excessive light or injury, and maintain lubrication by distributing tears over the surface of the eyeball. q The eyelids are split into upper and lower portions, which meet at the medial and lateral canthi of the eye. q The opening between the two eyelids is called the palpebral aperture or opening. q Eyelashes also help filter out dust and debris and prevent sweat from getting into the eye. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
CONJUNCTIVA q The conjunctiva is a thin, transparent layer of skin that begins at the outer edge of the cornea, covers the outer part of the sclera and coats the inside of the eyelids. q The conjunctiva produces a thick clear fluid that lubricates the eye, as well as producing some tears which help keep bacteria and foreign material from getting into the eye. q The conjunctiva is made up of microscopic blood vessels. q When the eye is irritated, injured or infected, the blood vessels dilate and make the eye look red. Khaleel Alyahya, Ph. D,
LACRIMAL GLANDS q The lacrimal glands are serous type exocrine glands that secrete lacrimal fluid onto the surfaces of the conjunctiva and cornea of the eye. q Lacrimal fluid acts to the clean, nourish and lubricate the eyes. q It forms tears when produced in excess. q It is located anteriorly in the superolateral aspect of the orbit, within the lacrimal fossa – a depression in the orbital plate of the frontal bone. q Its anatomical relations include: § Superior: zygomatic process of frontal bone § Anterior: orbital septum § Posterior: orbital fat § Inferolateral: lateral rectus muscle Khaleel Alyahya, Ph. D,
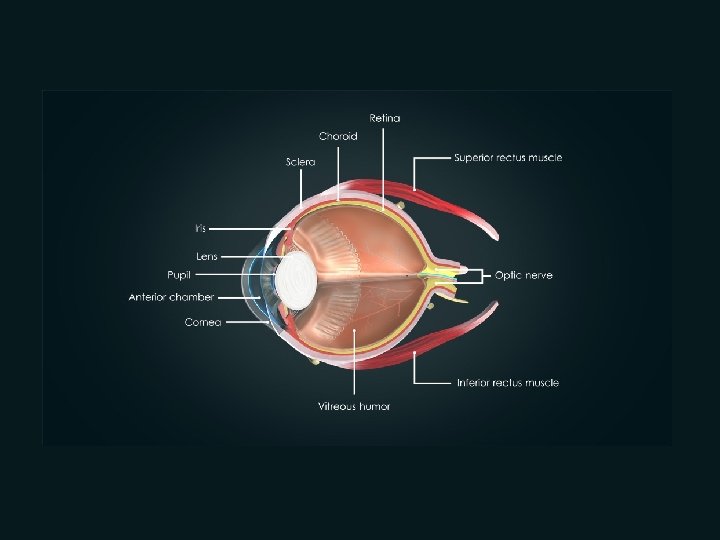
INTERNAL STRUCTURES: THE EYEBALL q Three layers, or tunics, form the wall of the eyeball: § Fibrous layer: outside layer. § Vascular layer: middle layer. § Sensory layer: inside layer. q Humors are fluids that fill the interior of the eyeball. q Lens divides the eye into two chambers. Khaleel Alyahya, Ph. D,
FIBROUS LAYER q Sclera § White connective tissue layer. § Seen anteriorly as the “white of the eye”. q Cornea § § Transparent, central anterior portion. Allows for light to pass through. Repairs itself easily. The only human tissue that can be transplanted without fear of rejection. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
SCLERA & CORNEA q The sclera is the protective outer wall of the eye and is made up of strong, fibrous tissue that expands from the cornea to the optic nerve. q The sclera is what gives the eye its white color and its shape. q The sclera is also attached to the extraocular muscles, which move the eye from side to side, up and down and diagonally. q The cornea is the clear dome-shaped layer at the front and center of the eye in front of the iris. q Its main role is to help bend or refract light into the lens as it enters the eye. q About 70% of the eye’s ability to focus comes from the cornea. q It contains no blood vessels to nourish or protect it against infection but Prof. Saeed Makarem receives these from tears and the Khaleel Alyahya, Ph. D,
VSACULAR LAYER q Choroid is a blood-rich nutritive layer that contains a pigment (prevents light from scattering). q Choroid is modified anteriorly into two smooth muscle structures. § Ciliary body. § Iris—regulates entering eye. amount of light • Pigmented layer that gives eye color. • Pupil—rounded opening in the iris. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
SENSORY LAYER q Retina contains two layers: § § Outer pigmented layer absorbs light and prevents it from scattering. Inner neural layer contains receptor cells (photoreceptors). § Rods and Cones. q Electrical signals pass from photoreceptors via a two -neuron chain. § § Bipolar neurons. Ganglion cells. q Signals leave the retina toward the brain through the optic nerve. q Optic disc (blind spot) is where the optic nerve leaves the eyeball. § Cannot see images focused on the optic disc. q Rods § § § Most are found toward the edges of the retina. Allow vision in dim light and peripheral vision. All perception is in gray tones. q Cones Allow for detailed color vision. Densest in the center of the retina. Fovea centralis–lateral to blind spot. • Area of the retina with only cones. • Visual acuity (sharpest vision) is here. Prof. Saeed Makarem § § § Khaleel Alyahya, Ph. D,
LENS q Flexible, biconvex crystal-like structure. q Held in place by a suspensory ligament attached to the ciliary body. q Lens divides the eye into two chambers: § Anterior (aqueous) segment • Anterior to the lens. • Contains aqueous humor, a clear, watery fluid. o o o Watery fluid found between lens and cornea. Similar to blood plasma. Helps maintain intraocular pressure. Provides nutrients for the lens and cornea. Reabsorbed into venous blood through the scleral venous sinus, or canal of Schlemm. § Posterior (vitreous) segment • Posterior to the lens. • Contains vitreous humor, a gel-like substance. o Gel-like substance posterior to the lens. o Prevents the eye from collapsing. o Helps maintain intraocular pressure. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
I ANTERIOR CHAMBER Y F q Immediately behind the cornea and the iris is a fluid-filled space known as the anterior chamber. q A fluid known as the aqueous humor fills the anterior chamber, providing nourishment for the cornea and the lens. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
POSTERIOR CHAMBER q The posterior chamber is the fluid-filled space in front of the lens and behind the iris. q The posterior chamber is filled with aqueous humor which is produced by the ciliary body. q The aqueous humor moves through the posterior chamber and then forward through the pupil into the anterior chamber. q In addition to the production of aqueous humor, the ciliary body controls the eye’s ability to accommodate or focus by changing the shape of the lens. q When the ciliary body contracts, the lens thickens, increasing the eye’s ability to focus up close. q When looking at an object at a Prof. Saeed Makarem distance, the ciliary body relaxes and Khaleel Alyahya, Ph. D,
ORBIT q The bony orbits (Sometimes called eye sockets) are bilateral and symmetrical cavities in the head. q They enclose the eyeball and its associated structures. q The orbit can be thought of as a pyramidal structure, with the apex pointing posteriorly and the base situated anteriorly. q The boundaries of the orbit are formed by seven bones. § § § § Frontal Sphenoid Ethmoid Zygomatic Maxilla Palatine Lacrimal q Fat pads protect the eye within the orbit. q The orbit also contains the lacrimal gland under the outer portion of the upper eyelid. q The role of the lacrimal gland is to produce tears to lubricate and moisten the eye and Prof. Saeed Makarem help clear the eye of any foreign matter, Khaleel Alyahya, Ph. D,
OPHTHALMOSCOPE q Instrument used to illuminate the interior of the eyeball and fundus (posterior wall). q Can detect diabetes, arteriosclerosis, degeneration of the optic nerve and retina. Khaleel Alyahya, Ph. D,
PHYSIOLOGY OF VISION q Pathway of light through the eye and light refraction. § Light must be focused to a point on the retina for optimal vision. § Light is bent, or refracted, by the cornea, aqueous humor, lens, and vitreous humor. § The eye is set for distant vision (over 20 feet away). § Accommodation—the lens must change shape to focus on closer objects (less than 20 feet away). § Image formed on the retina is a real image. § Real images are: § Reversed from left to right. • Upside down. • Smaller than the object. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
PHYSIOLOGY OF VISION q Visual fields and visual pathways to the brain. § Optic nerve • Bundle of axons that exit the back of the eye carrying impulses from the retina. § Optic chiasma • Location where the optic nerves cross. • Fibers from the medial side of each eye cross over to the opposite side of the brain. § Optic tracts • Contain fibers from the lateral side of the eye on the same side and the medial side of the opposite eye. • Synapse with neurons in the thalamus. § Optic radiation • Axons from the thalamus run to the occipital lobe. • Synapse with cortical cells, and vision interpretation (seeing) occurs. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
PHYSIOLOGY OF VISION q Summary of the pathway of impulses from the retina to the point of visual interpretation. § § § Optic nerve Optic chiasma Optic tract Thalamus Optic radiation Optic cortex in occipital lobe of brain q Visual fields § Each eye “sees” a slightly different view. § Field of view overlaps for each eye. q Binocular vision results and provides: § Depth perception (three-dimensional vision). Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
OPTIC NERVE q The optic nerve is responsible for transmitting visual information from the eye to the visual cortex of the brain for processing into an image. q The optic nerve is the second of twelve pairs of cranial nerves. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
HOW WE SEE? q Light enters the eye by first passing through the cornea, the clear outer portion of the eye. q The cornea is curved, focusing the light through the pupil, a round hole located in the center of the iris. q The thin circular iris is responsible for controlling the diameter and size of the pupil and therefore regulating the amount of light that can reach the retina. q Muscles attached to the iris expand or contract the pupil depending on how much light is present. q The larger the pupil, the more light can enter. q As the light passes through the lens, muscles in the eye cause the shape of the lens to become thicker or thinner to focus the light on the fovea centralis, which is in the middle of the macula on the retina at the back of the eye. q This process is known as refraction. q The retina converts the light into an electric signal that travels via the optic nerve to the brain stem and then to the visual cortex in the Prof. Saeed Makarem occipital lobe, where it is translated into an Khaleel Alyahya, Ph. D,
PHYSIOLOGY OF VISION q When light passes from one substance to another substance that has a different density, its speed changes and its rays are bent, or refracted. q Light rays are bent in the eye as they encounter the cornea, aqueous humor, lens, and vitreous humor. q The refractive, or bending, power of the cornea and humors is constant. q However, the lens can be changed by changing its shape by making it more or less convex, so that light can be properly focused on the retina. q The greater the lens convexity, or bulge, the more it bends the light. The flatter the lens, the less it bends the light. q In general, light from a distant source (over 20 feet away) approaches the eye as parallel rays, and the lens does not Prof. Saeed Makarem need to change shape to focus properly Khaleel Alyahya, Ph. D,
PHYSIOLOGY OF VISION q However, light from a close object tends to scatter and diverge, or spread out, and the lens must bulge more to make close vision possible. q To achieve this, the ciliary body contracts, allowing the lens to become more convex. q This ability of the eye to focus specifically for close objects (those less than 20 feet away) is called accommodation. q The image formed on the retina as a result of the light-bending activity of the lens is a real image—that is, it is reversed from left to right, upside down (inverted), and smaller than the object. q The normal eye is able to accommodate properly. q However, vision problems occur when a lens is too strong (overconverging) or Prof. Saeedweak Makarem (underconverging) or when too Khaleel Alyahya, Ph. D,
VISUAL FIELDS AND PATHWAY q Axons carrying impulses from the retina are bundled together at the posterior aspect of the eyeball and leave the back of the eye as the optic nerve. q At the optic chiasma (ki-as¿mah; chiasm = cross) the fibers from the medial side of each eye cross over to the opposite side of the brain. q The fiber tracts that result are the optic tracts. q Each optic tract contains fibers from the lateral side of the eye on the same side and the medial side of the opposite eye. q The optic tract fibers synapse with neurons in the thalamus, whose axons form the optic radiation, which runs to the occipital lobe of the brain. Saeed Makarem q. Prof. There they synapse with the cortical Khaleel Alyahya, Ph. D,
VISUAL FIELDS AND PATHWAY q Each side of the brain receives visual input from both eyes—from the lateral field of the eye on its own side and from the medial field of the other eye. q Also notice that each eye “sees” a slightly different view but that their visual fields overlap quite a bit. q As a result of these two phenomena, humans have binocular vision. q Binocular vision, literally “two-eyed vision, ” provides for depth perception, also called “threedimensional” vision, as our visual cortex fuses the two slightly different images delivered by the two eyes into one “picture. ” Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
A CLOSER LOOK q Emmetropia—eye focuses images correctly on the retina. q Myopia (nearsightedness) § Distant objects appear blurry. § Light from those objects fails to reach the retina and are focused in front of it. § Results from an eyeball that is too long. q Hyperopia (farsightedness) § Near objects are blurry, whereas distant objects are clear. § Distant objects are focused behind the retina. § Results from an eyeball that is too short or from a “lazy lens”. q Astigmatism § Images are blurry. § Results from light focusing as lines, not points, on the retina because of unequal curvatures of the cornea or lens. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
PATHOLOGY & DISEASES
ASTIGMATISM q Astigmatism occurs when the refractive surface of the cornea or lens is abnormally curved. q Light rays cannot focus sharply on the retina causing vision to be out of focus. q Astigmatism frequently occurs with other vision conditions like myopia and hyperopia. Khaleel Alyahya, Ph. D,
BLINDENESS q Blindness refers to a partial or complete loss of vision. q It may also refer to a loss of vision that cannot be adequately corrected with glasses or contact lenses. q Partial blindness means a person has very limited vision. q Complete blindness means a person cannot see anything and is also unable to perceive light. q The leading causes of blindness among Australians are macular degeneration, glaucoma, cataracts and diabetes. Khaleel Alyahya, Ph. D,
CATARACT q Cataract is a degenerative eye condition characterized by a clouding or opacity of the lens or the lens capsule. q It is a common cause of gradual vision loss. q Light shining through the cornea is blocked by the clouded lens — the image cast onto the retina is blurred, therefore the brain interprets a hazy image. q There are many different types of cataracts such as: senile, congenital, traumatic, complicated, toxic and diabetic. q Symptoms of cataracts include cloudy or blurry vision, faded colors, sensitivity to glare. q A halo may appear around lights. q Night vision is poor. q Cataracts are usually surgically removed and a replacement lens is inserted. Khaleel Alyahya, Ph. D,
GLAUCOMA q Glaucoma is an eye disease in which the optic nerve at the back of the eye atrophies. q In most people this damage is due to raised intraocular pressure due to problems with the drainage of the aqueous humor. q Chronic (primary open-angle) glaucoma is the most common type. q Damage progresses very slowly and destroys vision gradually, starting with peripheral vision. q It has no real symptoms until eyesight is lost at a late stage. q It can lead to blindness if not treated. Khaleel Alyahya, Ph. D,
PHACOEMULSIFICATION q Phacoemulsification is the most common form of treatment for cataracts. q It involves removing the lens by breaking it into tiny pieces and suctioning them off the eye. q The back of the capsule is left in place and an intraocular lens is implanted as a replacement. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
THE EAR
INTRODUCTION q Ear houses two senses: § § Hearing Equilibrium (balance) q Receptors are mechanoreceptors. § Responsible for providing information regarding pressure and texture. • • Chemicals (chemoreceptors) Temperature (thermoreceptors) Pressure (mechanoreceptors) Light (photoreceptors) q Different organs house receptors for each sense. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
FUNCTIONS q The auditory system allows mechanical processing and recognition of sounds. q The major organ of the auditory system is the ear, which acts as the receiver for sound, and has a major responsibility for maintaining balance and body position. q The ear operates with the nerves of the central nervous system to change sound pressure waves and transfer them as electrical impulses to the cerebral cortex in the brain, which processes them and allows us to hear. q Sounds are produced when an object vibrates in another substance — this might be something solid such as the earth, a liquid such as water, or a gas such as air. q The air is the most common way that sound is transferred in the environment. Khaleel Alyahya, Ph. D,
ANATOMY OF THE EAR q The ear is divided into three areas: § External (outer) ear § Middle ear § Internal (inner) ear Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
EXTERNAL (OUTER) EAR q Auricle (pinna). q External acoustic canal). meatus (auditory § Narrow chamber in the temporal bone. § Lined with skin and ceruminous (earwax) glands. § Ends at the tympanic membrane (eardrum). q External ear is involved collecting sound waves. Prof. Saeed Makarem only in Khaleel Alyahya, Ph. D,
MIDDLE EAR q Middle ear cavity (tympanic cavity) § Air-filled, mucosa-lined cavity within the temporal bone. § Involved only in the sense of hearing. § Located between tympanic membrane and oval window and round window. § Pharyngotympanic tube (auditory tube). • Links middle ear cavity with the throat. • Equalizes pressure in the middle ear cavity so the eardrum can vibrate. § Three bones (ossicles) span the cavity: 1) Malleus (hammer). 2) Incus (anvil). 3) Stapes (stirrup). § Function • Transmit vibrations from tympanic membrane to the fluids of the inner ear. • Vibrations travel from the hammer → anvil → stirrup → oval window of inner ear. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
INNER EAR q The inner ear has two roles — one relating to hearing and the other to the sense of balance, known as the vestibular system. q It is composed of three structures: the cochlea, three semicircular canals and the vestibule or labyrinth. q The cochlea is a snail-shaped cavity located in the bony labyrinth and contains the nerves which convert the sound vibrations in the fluid of the inner ear (known as perilymph) into nerve impulses which are transmitted to the brain from the organ of Corti (the body’s ‘microphone’ in the inner ear) via the auditory nerve. q The vestibule (labyrinth) and semicircular canals help maintain balance or equilibrium. q In order to achieve balance, the eyes, ears and the musculoskeletal system need to work together. q The brain receives, translates and processes Prof. Saeed Makarem the information from these systems to Khaleel Alyahya, Ph. D,
INTERNAL (INNER) EAR q Includes sense organs for hearing and balance q Bony labyrinth (osseous labyrinth) consists of: § Cochlea § Vestibule § Semicircular canals q Bony labyrinth is filled with perilymph § It is comparable to that of plasma and cerebrospinal fluid. § Perilymph and endolymph have unique ionic compositions suited to their functions in regulating electrochemical impulsesof hair cells necessary for hearing. Khaleel Alyahya, Ph. D,
EQUILIBRIUM q Equilibrium receptors of the inner ear are called the vestibular apparatus. q Vestibular apparatus has two functional parts: 1. 2. Static equilibrium. Dynamic equilibrium. § Movements cause otoliths to roll and bend hair cells. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
HEARING q Spiral organ of Corti § § § The body’s ‘microphone’ in the inner ear Located within the cochlear duct Receptors = hair cells on the basilar membrane Gel-like tectorial membrane is capable of bending hair cells Cochlear nerve attached to hair cells transmits nerve impulses to auditory cortex on temporal lobe q Pathway of vibrations from sound waves § § § Move by the ossicles from the eardrum to the oval window Sound is amplified by the ossicles Pressure waves cause vibrations in the basilar membrane in the spiral organ of Corti Hair cells of the tectorial membrane are bent when the basilar membrane vibrates against it An action potential starts in the cochlear nerve (cranial nerve VIII), and the impulse travels to the temporal lobe q High-pitched sounds disturb the short, stiff fibers of the basilar membrane Receptor cells close to the oval window are stimulated Prof. Saeed Makarem § Khaleel Alyahya, Ph. D,
DISEASES & PATHOLOGY
HEARING AND EQUILIBRIUM DEFICITS q Deafness is any degree of hearing loss § Conduction deafness results when the transmission of sound vibrations through the external and middle ears is hindered. § Sensorineural deafness results from damage to the nervous system structures involved in hearing. § Ménière’s syndrome affects the inner ear and causes progressive deafness and perhaps vertigo (sensation of spinning). Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
ACOUSTIC NEUROMA q Acoustic neuroma (also called a vestibular schwannoma) is a benign tumour that arises in the schwann cells that surround the acoustic nerve (also called the vestibulocochlear nerve or cranial nerve VIII). q The tumour can cause symptoms such as tinnitus, vertigo, balance problems and deafness. q The tumour grows in the auditory canal and may invade the brain stem and affect other local cranial nerves if not treated. Khaleel Alyahya, Ph. D,
DEAFNESS q Deafness (also called hearing loss is a partial or complete inability to distinguish or hear sounds. q It can be caused by heredity, premature birth, Rh incompatibility, diseases such as rubella and meningitis or due to damage to ear structures from continual exposure to loud noise. q Deafness can be broadly grouped into two main types. q Conductive deafness occurs when the sound conducting abilities of the auditory meatus, the tympanic membrane or the ossicles are affected. q Sensorineural deafness occurs as a result of damage to, or disease of, the nerves of the ear, for example in acoustic neuroma. Khaleel Alyahya, Ph. D,
OTOSCLEROSIS q Otosclerosis is a hereditary condition where the bony tissue of the middle or inner ear hardens. q Spongy bone forms around the oval window causing ankylosis (fixation) of the stapes. q This prevents transmission of sound energy to the inner ear, resulting in deafness. q Other symptoms may include tinnitus and dizziness. Khaleel Alyahya, Ph. D,
VERTIGO q Vertigo is a sensation of moving or spinning that is often symptomatic of inner ear disease. q A person with vertigo either feels that they are spinning (subjective vertigo) or their surroundings are spinning (objective vertigo). q Nausea is often present, and balance is affected. Khaleel Alyahya, Ph. D,
TESTS & PROCEDURES
AUDIOMETRY q Audiometry is a test of a patient’s hearing ability, usually performed using an audiometer and used to determine hearing loss or diseases of the ear. q The tests may also involve testing the patient’s ability to differentiate between sounds. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
COCHLEAR IMPLANT q Cochlear implant is a surgical procedure that involves the implantation of an electrode into the cochlear to allow for a person with sensorineural hearing loss to be able to detect sounds. q The electrode is connected to a small computer which is attached to the external ear. q The computer converts the sound waves to electronic impulses which stimulate nerve fibres. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
SMELL
INTRODUCTION q Smell and taste are considered chemical senses (Chemoreceptors). § § § Stimulated by chemicals in solution. Smell can differentiate a wider range of chemicals. Taste has five types of receptors. q Both senses complement each other and respond to many of the same stimuli. Khaleel Alyahya, Ph. D,
THE NOSE q The external (anterior ) nares or nostrils, lead to the nasal cavity. q Formed above by bony skeleton. q Formed below by plates of hyaline cartilage. Khaleel Alyahya, Ph. D,
FUNCTIONS o Olfaction – smell o Respiration – breathing o Warming the inspired air – submucous venous plexus o Filtration of dust o Humidification of the inspired air – Mucous o Reception of secretions from the paranasal sinuses and nasolacrimal duct. Khaleel Alyahya, Ph. D,
NASAL CAVITY q It is a large air filled space above and behind the nose in the middle of the face. q Each cavity is the continuation of one of the two nostrils. q It extends from nostrils anteriorly to turbinate (Choanae) posteriorly. q It is divided into right and left parts by the nasal septum. q It communicates with the nasopharynx posteriorly. q It consists of Vestibule, Respiratory and Olfactory regions. q Each contains, roof, floor, lateral and medial walls. Khaleel Alyahya, Ph. D,
OLFACTORY RECEPTORS AND THE SENSE OF SMELL q Olfactory receptors are in roof of nasal cavity. § § Olfactory receptor cells (neurons) with long cilia known as olfactory hairs detect chemicals. Chemicals must be dissolved in mucus for detection by chemoreceptors called olfactory receptors. q Impulses are transmitted via the olfactory filaments to the olfactory nerve (Cranial Nerve I). q Smells are interpreted in the olfactory cortex. Khaleel Alyahya, Ph. D,
OLFACTORY BULB q In the cranial cavity, the fibres enter the olfactory bulb, which lies in the olfactory groove, within the anterior cranial fossa. q The olfactory bulb is an ovoid structure which contains specialised neurones, called mitral cells. q The olfactory nerve fibres synapse with the mitral cells, forming collections known as synaptic glomeruli. q From the glomeruli, second order nerves then pass posteriorly into the olfactory tract. Khaleel Alyahya, Ph. D,
ANOSMIA q The absence of the sense of smell. q It can be temporary or permanent. q Temporary anosmia can be caused by infection or by local disorders of the nose. q Permanent anosmia can be caused by head injury, or tumours which occur in the olfactory groove (e. g. meningioma). q Anosmia can also occur as a result of neurodegenerative conditions, such as Parkinson’s or Alzheimer’s disease. Khaleel Alyahya, Ph. D,
DYSOSMIA q A distortion in the quality of the perception of an odor. q Sometimes, the perception of an odor when no odor is actually present. q Damage to olfactory nerve fibers can occur as a complication of upper respiratory tract infections. q A decrease in the number of nerve fibers from these infections mean that there are not enough different fibers to accurately differentiate odors resulting in parosmia. Khaleel Alyahya, Ph. D,
TASTE
INTRODUCTION q Smell and taste are considered chemical senses (Chemoreceptors). § § § Stimulated by chemicals in solution. Smell can differentiate a wider range of chemicals. Taste has five types of receptors. q Both senses complement each other and respond to many of the same stimuli. Khaleel Alyahya, Ph. D,
INTRODUCTION q The sense of taste is also called gustation. q The sensation of taste can be classified into five basic categories: § § § Sweetness Bitterness Sourness Saltiness Savouriness or umami. q Taste allows us to identify products as appetitive or aversive, depending upon the effect they have on the body. q Appetitive means the instinctive desire to eat specific foods to maintain life, while aversive refers to the body’s tendency to reject noxious substances. q The five basic tastes contribute to the sensation and flavour of food in the mouth but are supported by other factors including the sense of smell (as described above) and the texture and temperature of Khaleel Alyahya, Ph. D,
STRUCTURES q The word taste comes from the Latin word taxare, which means “to touch, estimate, or judge. ” q When we taste things, we are, in fact, testing or judging our environment in an intimate way, and many of us consider the sense of taste to be the most pleasurable of our special senses. q The taste buds, or receptors for the sense of taste, are widely scattered in the oral cavity. q Of the 10, 000 or so taste buds that we have, most are on the tongue. q A few are scattered on the soft palate, superior part of the pharynx, and inner surface of the cheeks. q The dorsal tongue surface is covered with small peglike projections, or papillae. q The taste buds are found on the sides of the large round vallate papillae, or circumvallate papillae, on the tops of the more numerous fungiform papillae and in the foliate papillae Prof. Saeed Makarem on the sides of the tongue. Khaleel Alyahya, Ph. D,
TASTE BUDS AND THE SENSE OF TASTE q Taste buds house the receptor organs. q Locations of taste buds. § § Most are on the tongue. Soft palate. Superior part of the pharynx. Cheeks. q The tongue is covered with projections called papillae that contain taste buds. § § § Vallate (circumvallate) papillae. Fungiform papillae. Filiform papillae. q Gustatory cells are the taste receptors. § § § Possess gustatory hairs (long microvilli). Gustatory hairs protrude through a taste pore. Hairs are stimulated by chemicals dissolved in saliva. q Impulses are carried to the gustatory complex by several cranial nerves because taste buds are found in different areas. § § § Facial nerve (cranial nerve VII). Glossopharyngeal nerve (cranial nerve IX). Vagus nerve (cranial nerve X). q Taste buds are replaced frequently by basal Khaleel Alyahya, Ph. D,
FIVE BASIC TASTE SENSATIONS q Sweet receptors respond to sugars, saccharine, some amino acids. q Sour receptors respond to H+ ions or acids. q Bitter receptors respond to alkaloids. q Salty receptors respond to metal ions. q Umami receptors respond to the amino acid glutamate or the beefy taste of meat. § A taste discovered by the Japanese, is elicited by the amino acid glutamate, which appears to be responsible for the “beef taste” of steak and the flavor of monosodium glutamate, a food additive. Khaleel Alyahya, Ph. D,
TOUCH
INTRODUCTION q While the four other human senses (sight, hearing, smell and taste) are located in particular parts of the body, the sense of touch is found throughout the body. q Because there are different numbers of nerve endings in various parts of the body, some areas are more sensitive to touch than others. q The reason that touch is perceived all over the body is because the sense of touch stems from the dermal skin layer. q The human skin acts as the protective barrier between the internal body systems and the external environment. q The perception of touch provides the process whereby the skin tells the brain about its surroundings through an arrangement of nerve endings and touch receptors known as the somatosensory system. Prof. Saeed Makarem Khaleel Alyahya, Ph. D,
STRUCTURES q This system is responsible for sensations such as cold, heat, texture, pressure, irritation, pain and vibration. q Within this system, the four types of main receptors are: § Mechanoreceptors, which react to pressure, vibrations and texture. § Thermoreceptors, which respond to temperature. § Pain receptors, which detect pain or stimuli that could cause damage to the tissues of the body. § Proprioceptors, which act as part of the musculoskeletal system to perceive the position of the different parts of the body in relation to each other and their environment. q The receptors transmit information via sensory nerves in the spinal cord into the brain. q The brain processes the message in the Prof. Saeed Makarem parietal lobe of the cerebral cortex and Khaleel Alyahya, Ph. D,
QUESTIONS?