Percutaneous Treatment of Mitral Regurgitation Why do we


 Sept")


")
 vs. Secondary (functional or FMR) Mitral Regurgitation • • •")







 Anatomic Target Device Name Manufacturer Status Leaflet/Chordal Mitra. Clip")



:")


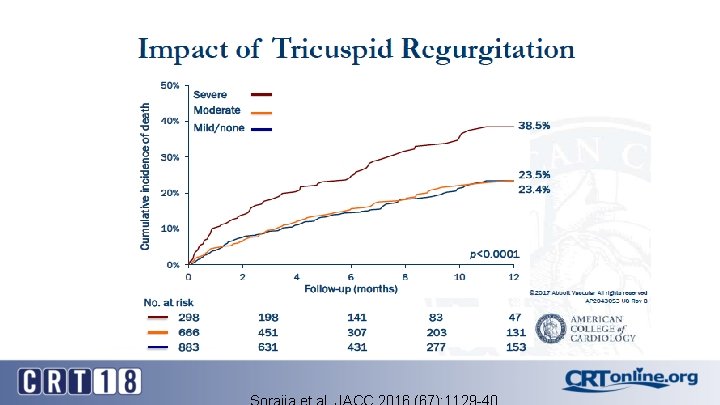
 Outcomes Sorajja et al. JACC 2016 (67): 1129 -40")
: 1129 -40")
: 1129 -40")
: 1129 -40")
: 1129 -40")


")

- Slides: 37
Percutaneous Treatment of Mitral Regurgitation: Why do we need it at the VA? Santiago Garcia, MD Associate Professor of Medicine, University of Minnesota Director, Structural Heart Program MVAHCS Garci 205@umn. edu
Disclosures <Type of Relationship>: <Company 1> <Company 2> Examples of relationships are: Advisory Board/Board Member, Consultant, Honoraria, Research Support, Speaker’s Bureau, Stockholder Please list full company name
Prevalence of Valvular Heart Disease by Age Nkomo et al. The Lancet (368) Sept 16, 2016
The mitral valve
Primary MR: The problem is in the leaflets
Secondary MR: The problem is in the MV complex (annulus, PM, chordae, LV)
Primary (degenerative or DMR) vs. Secondary (functional or FMR) Mitral Regurgitation • • • Severe Primary MR Central jet > 40% of LA or holosystolic eccentric jet Vena contracta ≥ 0. 7 cm Regurgitant volume > 60 ml Regurgitant fraction ≥ 50% ERO ≥ 0. 40 cm 2 Angiographic grade 3 -4+ Severe Secondary MR (ACC 2014) • ERO > 0. 2 cm 2 • Regurgitant volume > 30 cc • Regurgitant fraction > 50% Severe Secondary MR (ACC 2017) • ERO ≥ 0. 40 cm 2 • Regurgitant volume > 60 ml JACC/AHA Valvular Heart Disease Guidelines. JACC (63). N 22. June 10 th 2014. Nishimura et al. J Am Coll Cardiol 2017; 70: 252– 89.
Stages of MR Nishimura et al. J Am Coll Cardiol 2017; 70: 252– 89.
Indications for Surgery
Indications for Intervention: Primary MR
Indications for Intervention: Secondary MR No Class I Indications
Standard of care: MV Repair
Double Lumen Valve: Alfieri’s Procedure or “Surgical Clip”
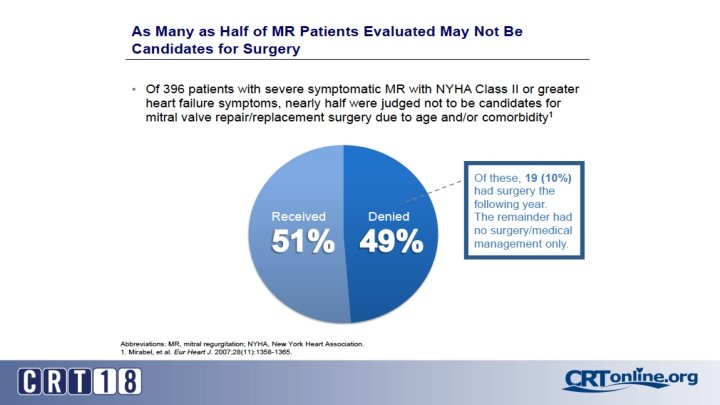
Transcatheter Therapies: Why? • Surgery is associated with mortality rates of 1 -5% • Morbidity rates 10%-20% (stroke, prolonged ventilation, renal failure, bleeding) • Mortality in octogenarians as high as 17% with > 20% risk of hospitalization within 30 days • 30% recurrence of 3 -4+ MR in patients with ischemic MR treated with surgery • Up to 50% of patients that have an indication for MVR do not undergo surgery
Transcatheter Therapies for MR (2018) Anatomic Target Device Name Manufacturer Status Leaflet/Chordal Mitra. Clip Abbott Vascular CE Mark/FDA approved Neochord (MN) CE Mark PASCAL Edwards Phase I, FIM Carrillon Cardiac Dimensions CE Mark Cardioband Valtech Cardio CE Mark GDS Accucinch Guided delivery systems Phase I Hybrid surgical Annuloplasty ring SJM (MN) CE Mark LV remodeling Basal Annuloplasty (BACE) Mardil Medical (MN) Phase I Replacement Tiara Neovasc Phase I, FIM Intrepid Medtronic (MN) Phase I, FIM Cardia Q Edwards Phase I, FIM Tendyne Abbott Vascular Phase I, FIM Annuloplasty
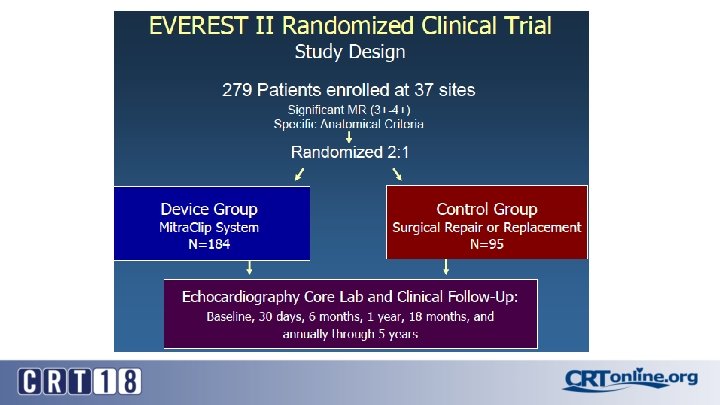
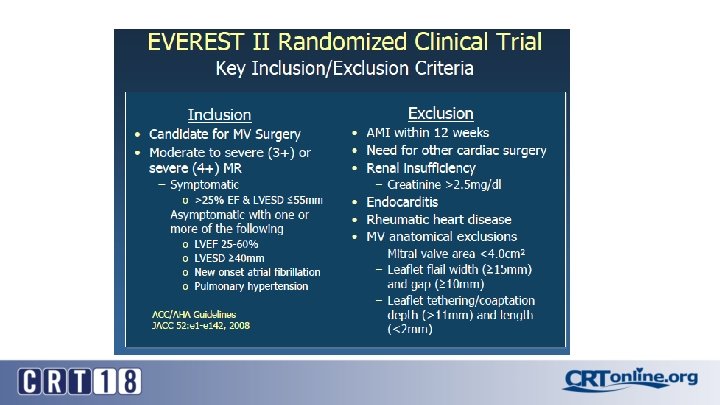
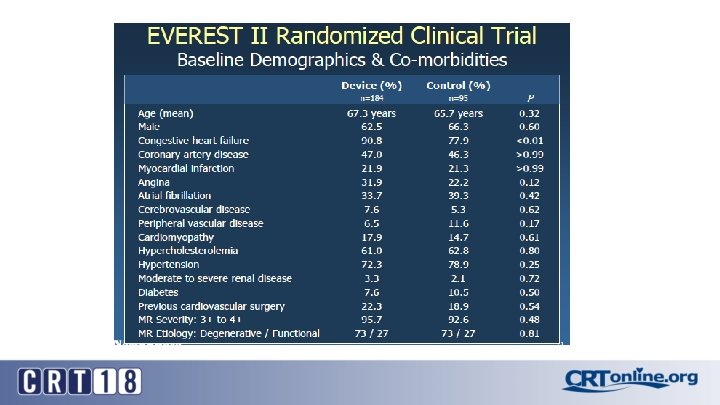
The Clinical Evidence: EVEREST II Trial
EVEREST II 1 -Year Results “percutaneous repair less effective… but associated with superior safety” Device Control (Surgery) Death 6% 6% Surgery for MV dysfunction 20% 2% Grade 3+ or 4+ MR 21% 20% Primary End-Point (freedom from death, MV surgery or MR grade 3 -4) MACE 55% 73% 15% 48% Feldman et al. NEJM 2011; 364: 1395 -406
FDA approved indications and ACC/AHA Guidelines: Mitra. Clip
Commercial Experience in the US Average Age=83, STS=8 Sorajja et al. JACC 2016 (67): 1129 -40
Residual MR After Mitra. Clip 93 % with Residual MR Grade 1 or 2. 37% required > 1 Clip
Predictors of Success after Mitra. Clip : A 2 -P 2 Pathology and Case Volume
Short-Term (30 -day) Outcomes Sorajja et al. JACC 2016 (67): 1129 -40
Sorajja et al. JACC 2016 (67): 1129 -40
Sorajja et al. JACC 2016 (67): 1129 -40
Sorajja et al. JACC 2016 (67): 1129 -40
Sorajja et al. JACC 2016 (67): 1129 -40
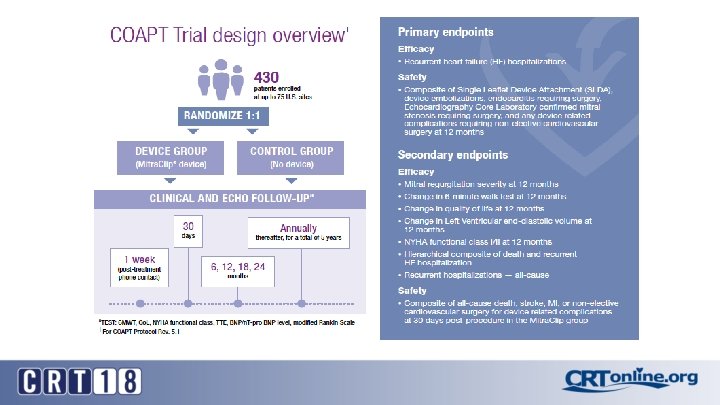
Ongoing Mitra. Clip Trials • COAPT: Clinical Outcomes Assessment of the Mitra. Clip Percutaneous Therapy for Extremely High-Surgical Risk Patients (NCT: 01626079)
Worldwide Mitra. Clip Registries: Most Patients Treated in Europe have FMR
FDA approved indications and ACC/AHA Guidelines: Mitra. Clip (2017)
Percutaneous Treatment of Mitral Regurgitation Santiago Garcia, MD Associate Professor of Medicine, University of Minnesota Director, Structural Heart Program MVAHCS Garci 205@umn. edu