Paediatric Procedural Sedation v 2011 Royal Children Hospital








")




, light-headedness Ü Excessive sedation (caution")






 Ü Stridor (malpositioning of the airway)")






- Slides: 29
Paediatric Procedural Sedation v. 2011 Royal Children Hospital ECIICN Victorian Managed Insurance Authority
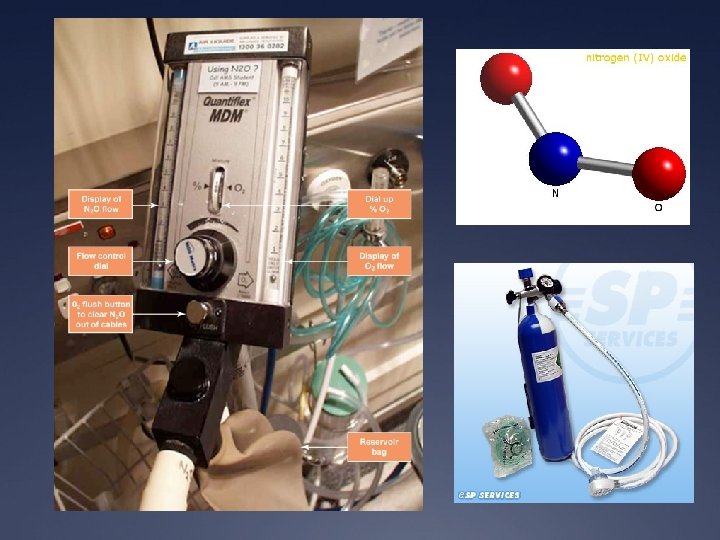
Program Ü Talk Ü Read handout on nitrous connections Ü Nitrous machine practical set up
Goal Ü Physical and psychological distress Ü Optimal environment for success Analgesia Anxiolysis Amnesia Awareness
Who is this talk for ? Ü Deliver quality care consistent with evidence base Ü Minimise risk and adverse events Ü Able to administer procedural sedation safely Ü Able to recognise and address undesirable events (rescue capacity)
Ü http: //www. youtube. com/watch? v=t. GNy. WDlu. ELQ Ü http: //www. youtube. com/watch? v=gm. Nwp. Jf 1 z. UQ Beware in asthmatics / RTI
General principles Ü Will my sedation plan achieve the best outcome for THIS patient ? Ü Successful sedation doesn’t always guarantee success of procedure or best outcome Ü What simple things can I do to reduce anxiety and need for sedation? Ü Preparation and post-procedural issues Ü Patient, Staff, Place
Levels of sedation Ü Minimal Ü Moderate Ü Deep Ü GA American Society of Anesthesiologist (ASA) Classification (circle one) Ü 1 A normal healthy patient Ü 2 A patient with mild systemic disease Ü 3 A patient with severe systemic disease Ü 4 Moribund patient who is not expected to survive without the operation Ü *Class 3 or greater: Benefit of procedure outweighs risk of anesthesia
Reducing need for sedation Ü Early systemic analgesia Ü Paracetamol, painstop, nurofen, IN fentanyl (1. 5 mcg/kg) Ü ALA (adr/lig/ameth) vs EMLA (lig/prilo) Ü Infants : Sucrose (5 -8 min), non-nutritional sucking Ü Non-pharmacological : distraction, balloon, bubbles, “safe person”, build rapport Ü Alternatives : glue, theatre (avoids repeat sedation) Ü Encourage coping behaviours Ü Modify environment Ü Parents Ü Reduce anxiety
Risk assessment Ü Disease factors Ü Cerebral palsy, NM disorders, airway risk (Prader-willi, Down’s) Ü Obvious contraindications / drug int Ü Previous sedation failure Ü Age < 1 yo Ü IN fentanyl enhances NO 2 sedation
Ü The decision to sedate an unfasted patient for emergency procedures should be based on a careful assessment of the urgency of the procedure, the desired sedation depth, the fasting status and individual patient risk factors Ü The more urgent, the less fasting required, when less urgent, stick to minimum fasting guidelines NO 2: Ketamine: 2 hrs clear liquid 4 hrs solids/milk *consensus
Ü Know your age-specific obs Ü Observations Ü 5 minly if child deeply sedated Ü 15 minly once improve Ü Discharge instructions Ü Can child sit up/walk unaided? Ü Tolerating fluids? Ü Back to baseline consious state? Ü Address carer concerns
N 20 Ü Inert colourless odourless Ü First synthesized in 1772 Joseph Priestley Ü “laughing gas” – Sir Humphry Davy Ü Promotes opioid peptide release from midbrain Ü Weak anaesthetic Ü Low solubility => rapid onset
N 20 pros ? Ü Short acting, titratable Ü Fast onset 3 -5 mins, fast offset Ü Inhalational analgesia and anasthesia Ü Safe Ü Requires a good seal with dedicated administrator
N 20 cons ? Ü Vomiting (6% at home), light-headedness Ü Excessive sedation (caution URTI) Ü Requires cooperative child Ü Pregnant staff exclusion Ü Efficacy – not for all Ü Not useful for certain procedures Ü BM / Neurotoxicity, B 12 def (rare)
N 20 tips Ü Check supply Ü Check connections Ü Scavenger – medium flow Ü Suction Ü Bag : encourage blowing, hose : elephant nose Ü Additional O 2 mask/BVM Ü Flavoured scents Ü Familiarise child with equipment Ü OK to apply obs post. NO 2 taking effect
Ü Dose ?
Handout “Use of Nitrous Oxide in the ED”
“Vitamin K” Ü Dissociative anaesthetic Ü Hallucinatory reactions abused Ü Nightmares Ü Delirium
Ketamine pros Ü Major advantages Ü Immobilisation Ü Maintenance of airway and resp drive Ü Profound analgesia Ü Mechanism of action Ü Cardiac stable
Ketamine cons? Ü Overall uncommon and minor Ü Vomiting 8. 6% Ü Emergence 7. 6% Ü Airway / Resp 3. 9% Ü No association with fasting Ü IV vs IM Ü Longer onset and longer LOS with IM Ü Balanced with distress of IV insertion
Respiratory Ü Resp depression (very young, rapid push) Ü Stridor (malpositioning of the airway) Ü Laryngospasm Ü 0. 002 -0. 3% incidence, 1/22 cases required ETT Ü Idiosyncratic Ü Airway support, PEEP and wait Ü Hypersalivation (X atropine, may increase events)
Emergence phenomenon Ü Range of behaviours Ü More common in adolescents, not an absolute CI Ü Responds well to midazolam but not as prophylaxis Ü Manage as per acute agitation
Others Ü Modest rise in HR, BP, metabolism Ü Hypertonicity, tremor, random movements Ü Does not reflect depth of sedation Ü Seizures (case reports) Ü ICP/IOP elevation Ü Rash Ü Ataxia
CI Ü Children < one year / >12 years Ü Previous adverse reaction to ketamine Ü Active respiratory tract infection or disease Ü Procedures involving the lower airway or pharynx Ü Heart disease Ü Bowel obstruction Ü Psychosis / ADHD Ü Porphyria Ü Thyrotoxicosis Ü Unstable epilepsy Ü Glaucoma Ü Central nervous system masses, hydrocephalus
Practical tips Ü Full resus area with airway backup Ü Take time to explain to parents Ü Lights are on, but no one’s home Ü Saliva/tears not sign of pain or distress Ü Parents present Ü Rash spontaneously resolve
Dose