Primary Acquired Hypothyroidism in childhood Dr Abolfazl Heidari

Primary Acquired Hypothyroidism in childhood Dr. Abolfazl Heidari

Primary Acquired Hypothyroidism • The most common cause of acquired hypothyroidism in children is autoimmune thyroiditis, • The disorder is associated with numerous genetic loci including those related to the thyroid itself and to immune functions including CTLA-4, PTPN 22, FOXP 3, and the human leukocyte antigen (HLA) DR 3 allele. • The incidence of autoimmune thyroiditis increases with age: it is rare in the first 3 years of life and becomes progressively more common through school age and adolescence. • It is more common in females and in patients with trisomy 21 and Turner syndrome.

Primary Acquired Hypothyroidism • Other causes: o Iodine deficiency o medications (including lithium, amiodarone, certain antiepileptics, interferons and interleukins) o Iodinated radiographic contrast o viral Thyroiditis o Children with mild defects in certain genes that can cause congenital hypothyroidism (such as DUOX 2) may present with hypothyroidism later in childhood rather than at birth.

Clinical Manifestations of Hypothyroidism

Clinical Manifestations of Hypothyroidism • Hypothyroidism may cause delayed puberty, but rarely severe cases can cause pseudo-precocious puberty with breast development and/or premature menarche in girls or testicular enlargement in boys. • This effect is presumably due to cross-reactivity of high serum concentrations of TSH with the FSH receptor. • Such pseudoprecocity is distinguished from true precocious puberty by the presence of retarded— rather than accelerated—growth and bone maturation.

Treatment and Prognosis of Hypothyroidism • The dose of LT 4 required to restore euthyroidism depends on patient age and on the severity of hypothyroidism. • The dose required per kilogram body mass to fully replace thyroid function is significantly higher in children than in adults and decreases with age.

Treatment and Prognosis of Hypothyroidism

Treatment and Prognosis of Hypothyroidism • Patients with acquired hypothyroidism can generally be initiated immediately on the chosen dose of LT 4 at the time of diagnosis. • In rare cases, initiation of treatment in a child with severe hypothyroidism can be associated with severe behavioral symptoms or pseudotumor cerebri. • however, it is not clear whether initiating a lower dose and increasing it over time decreases the risk of such reactions. • Importantly, poor growth sustained during longstanding hypothyroidism may not be compensated after initiation of treatment, leading to an irremediable loss of adult height.

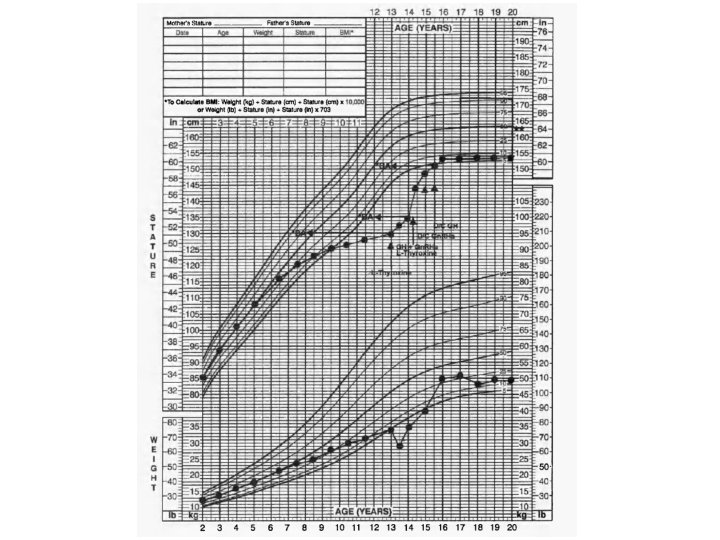
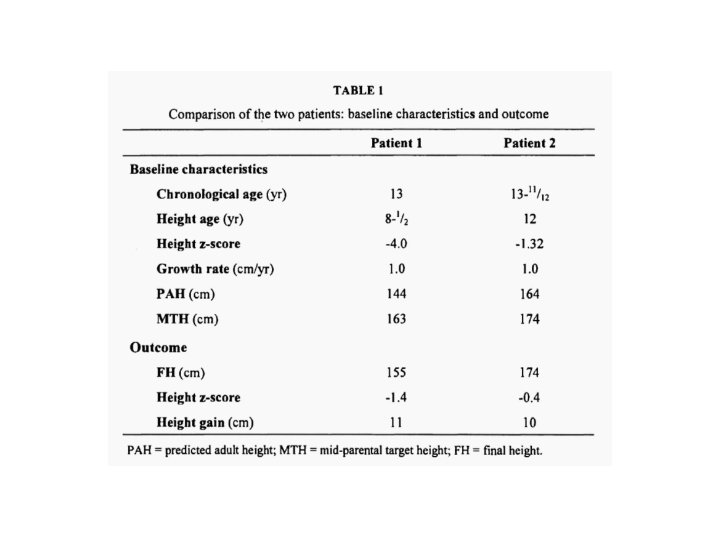
Patient 1 • 13 year-old girl who presented with pubertal delay, short stature (height SDS -4), and marked bone age retardation (BA 8 yr). • Serum T 4 was undetectable and TSH level was 1, 139 m. IU/1. • After 1 year of treatment with Lthyroxine, growth rate improved from 1. 0 cm/yr to 9. 8 cm/yr but puberty progressed (Tanner 3 breast) and BA accelerated by 4 years, compromising predicted adult height (PAH) (144 cm vs mid-parental target height [MTH] of 163 cm). • Combined use of GH and Gn. RHa for one year slowed BA progression, and catch-up growth (10. 4 cm/yr) continued to attain a final height (FH) of 155 cm.

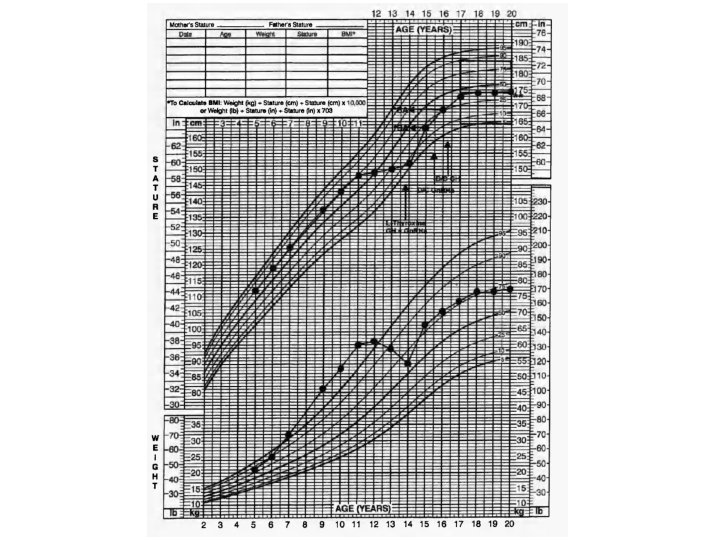
Patient 2 • 14 year-old boy with undetectable T 4, TSH of 811 m. IU/1 in mid-puberty with poor growth rate (1. 0 cm/yr), without any bone age delay (BA 14 years) but compromised PAH (163. 8 cm vs MTH 174 cm). • Because of the advanced puberty and poor growth rate, treatment with GH and Gn. RHa was initiated. Treatment for 2 years led to improvement of growth velocity (10. 6 cm/yr), slowed BA progression to attain a FH equal to MTH.

• Severe acquired hypothyroidism often results in significant height deficit due to rapid bone age advancement following treatment. • Whether gradual correction of hypothyroidism and/or adjunctive growth-promoting therapies (GPTs) augment final adult height (FAH) is controversial.

• In profoundly hypothyroid children, pediatric endocrinologists often recommend replacing thyroid hormone with an initial low dose of levothyroxine that is increased slowly over several months. • An additional strategy that aims to increase ultimate height is to add adjunctive growthpromoting therapies (GPTs) such as a gonadotropin-releasing hormone agonist (Gn. RHa), GH, or an aromatase inhibitor.

Method: • Following institutional review board approval, a retrospective chart review was performed of children seen in the pediatric endocrinology clinics at Riley Hospital for Children over the last 13 years. • Inclusion criteria were a diagnosis of acquired hypothyroidism, initial TSH ≥ 150 m. IU/L, and initial bone age standard deviation score (SDS) ≤ – 1. 75
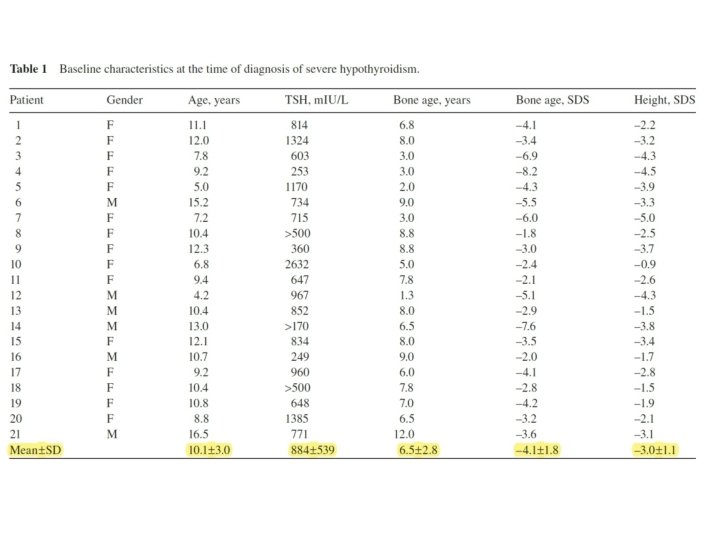

• Four subjects remained prepubertal, whereas 17 were already in or entered puberty during followup. • The average starting dose of levothyroxine was 22. 6 ± 6. 4 μg daily, and doses ranged from 12. 5 μg (n = 5), to 25 μ g (n = 15), to 37. 5 μg (n = 1). • Time to euthyroidism, which is a surrogate for the rate of dose increase, ranged from 2. 3 to 33. 7 months (average 9. 7 months). • The average duration between initial bone age and subsequent bone age was 21. 9 ± 7. 7 months (range 12. 5– 42. 2 months). • The average rate of skeletal maturation ( Δ BA/ Δ CA) was 2. 3 ± 0. 9 (range 1. 0– 3. 9).
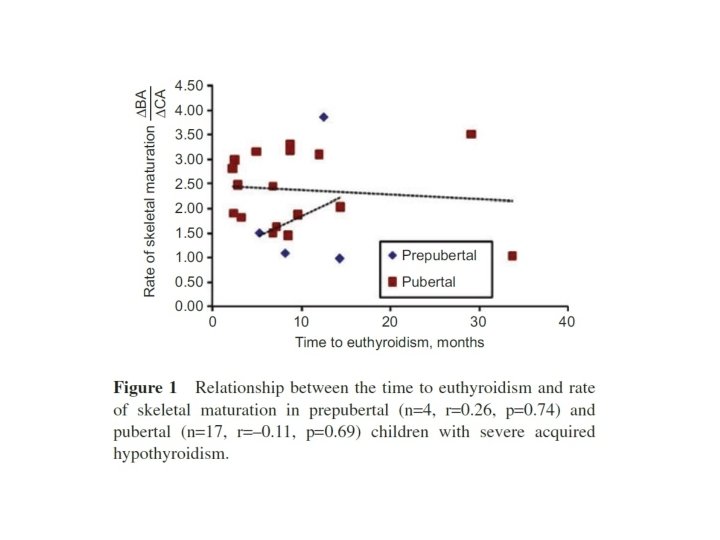

• No correlation was found between the time to euthyroidism and the rate of skeletal maturation in the total group (n = 21, r = – 0. 05, p = 0. 81). • A separate analysis of the prepubertal (n = 4, r = 0. 26, p = 0. 74) and pubertal (n = 17, r = – 0. 11, p = 0. 69) subgroups similarly did not reveal any statistically signifi cant correlations.

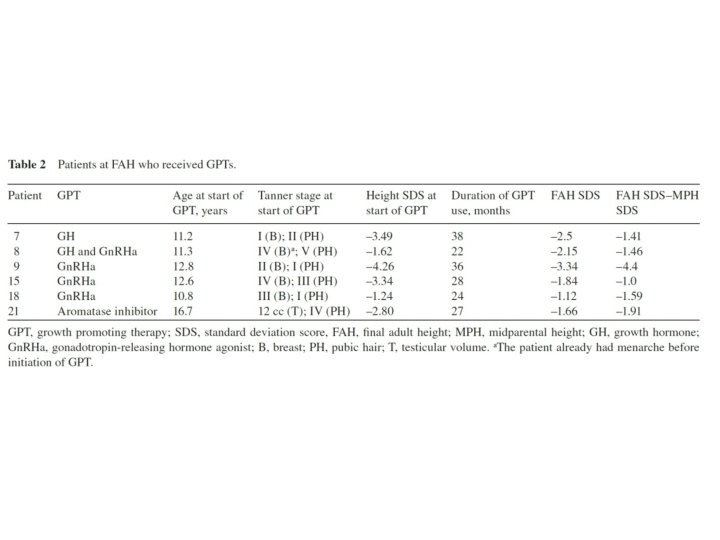
• Of the 21 subjects, 13 had reached FAH at the time of review. • Of these, six had received GPTs in addition to levothyroxine replacement. This consisted of Gn. RHa alone (n = 3), Gn. RHa plus GH (n = 1), GH alone (n = 1), and aromatase inhibitor (n = 1). • The remaining seven patients received no additional therapies beyond thyroid hormone replacement. • No differences were noted in change in height from diagnosis to FAH between those who received GPTs and those who did not at baseline (mean change in height SDS was – 1. 1 vs. – 1. 6, respectively).
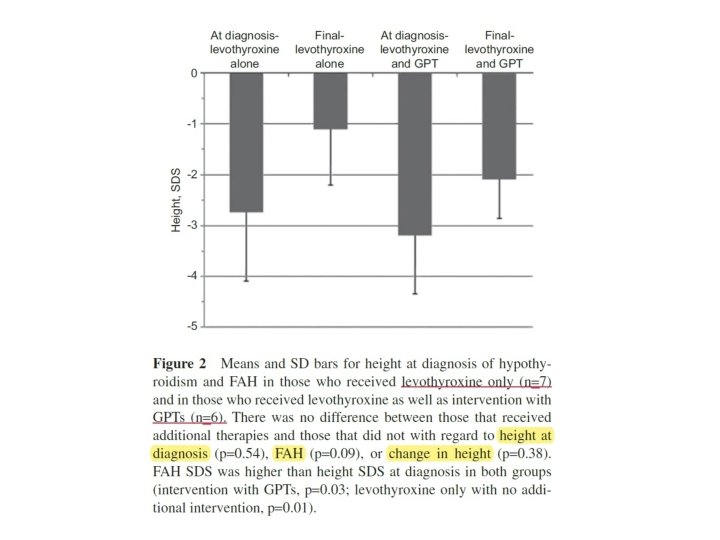

• However, the power to detect this difference was only 12 %. To have 80 % power to detect this effect size, 62 patients per group would have been required. • Overall and within the group that received only levothyroxine as well as within the group that received levothyroxine plus GPTs, patients were significantly shorter than midparental height, both at baseline and at FAH (p < 0. 001 for both comparisons overall and p ≤ 0. 01 for both comparisons within each group).

The Thyroid 2013 • In prepubertal children with severe hypothyroidism, pubertal development and bone maturation should be monitored closely, because progression may be too rapid. • The reason for this is unclear but when it occurs, administration of a Gn. RH agonist to decrease sex steroid secretion and delay epiphyseal maturation may be considered, although the impact of combined T 4 and agonist therapy on adult height is uncertain.
- Slides: 29