Overview of Radiation Protection Principles of radiation protection






 is an informal expression of ionising")





 1980 and")












 • It is a matter for national professional bodies, sometimes in")
 • To check that the required information")


 • • • Atomenergy Smoking Antibiotics X-ray diagnostic")
 • • • Smoking Consumtion of alcoholic drinks")






 m. Sv 500 450 400 350 300 250 200")


 Occupational Effective dose Annual equivalent dose to ► Lens of")
 Students, trainee Effective dose Annual equivalent dose to ► Lens")



- Slides: 51
Overview of Radiation Protection Principles of radiation protection, dose limits Bálint Vecsei dr.
• http: //www. kernenergie. de
• radioaktivität röntgenstrahlen und gesundheit
Introduction • • Radiation is indispensable in modern medicine The radiographic examination is one of the principal diagnostic method used in all fields of medical services The risk associated with low-level diagnostic exposures could be low, but greater than zero For this reason it is required to measure the dose in the diagnostic radiology
Introduction • Radiographic examinations play an essential part of dental practice. • • • The use of X-rays is an integral part of clinical dentistry On the majority of patients some form of radiographic examination is necessary „The clinican’s main diagnostic aid. ” • The range of knowledge of dental radiography can be divided conveniently into four main sections: – – Basic physics and equipment Radiaton protection Radiography Radiology
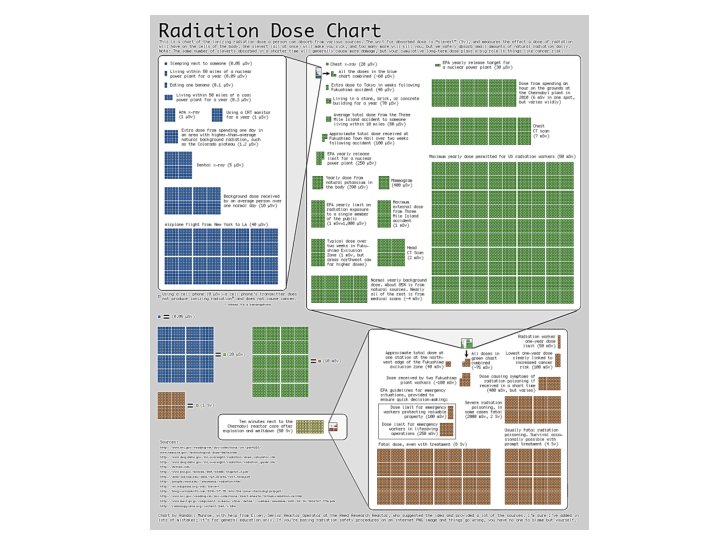
• • Every day all over the world people are exposed to ionising radiation, almost all from natural sources in the environment or for medical reasons. Ionising radiation has enough energy to cause damage cells which can increase the risk of cancer later in life. In general the health effects of ionising radiation are dependent on the received dose. Several different terms and units have been used in dosimetry over the years. Natural sources account most of the radiation we all receive each year
• A banana equivalent dose (abbreviated BED) is an informal expression of ionising radiation exposure, intended as a general educational example to indicate the potential dose due to naturally occurring radioactive isotopes by eating one average sized banana. However, in practice this dose is not cumulative as the principal radioactive component is excreted to maintain metabolic equilibrium. The BED is only an indicative concept meant to show the existence of very low levels of natural radioactivity within a natural food, and is not a formally adopted dose quantity. The concept probably originated on the Rad. Safe nuclear safety mailing list in 1995, [original research? ] where a value of 9. 82× 10− 8 sieverts or about 0. 1 μSv was suggested for a 150 gram banana.
Comparison of doses from sources of exposure Source of Exposure Dental X-ray 135 g bag of Brazil nuts Chest X-ray Transatlantic flight Nuclear power station worker average annual occupational exposure Dose 0. 005 m. Sv 0. 02 m. Sv 0. 07 m. Sv 0. 18 m. Sv UK annual average radon dose CT scan of the head UK average annual radiation dose USA average annual radiation dose CT scan of the chest Average annual radon dose to people in Cornwall 1. 3 m. Sv 1. 4 m. Sv 2. 7 m. Sv 6. 2 m. Sv 6. 6 m. Sv 7. 8 m. Sv Whole body CT scan Annual exposure limit for nuclear industry employees 10 m. Sv 20 m. Sv Level at which changes in blood cells can be readily observed 100 m. Sv Acute radiation effects including nausea and a reduction in white blood cell count 1000 m. Sv Dose of radiation which would kill about half of those receiving it in a month 5000 m. Sv
Units of radiation and radioactivity In order to quantify how much radiation we are exposed to in our daily lives and assess potential health impacts as a result, it is necessary to establish a unit of measurement. • The basic unit of radiation dose absorbed in tissue is the gray (Gy), where one gray represents the deposition of one joule of energy per kilogram of tissue. • However, since neutrons and alpha particles cause more damage per gray than gamma or beta radiation, another unit, the sievert (Sv) is used in setting radiological protection standards. This unit of measurement takes into account biological effects of different types of radiation. • One gray of beta or gamma radiation has one sievert of biological effect, one gray of alpha particles has 20 Sv effect and one gray of neutrons is equivalent to around 10 Sv (depending on their energy). • Since the sievert is a relatively large value, dose to humans is normally measured in millisieverts (m. Sv), onethousandth of a sievert.
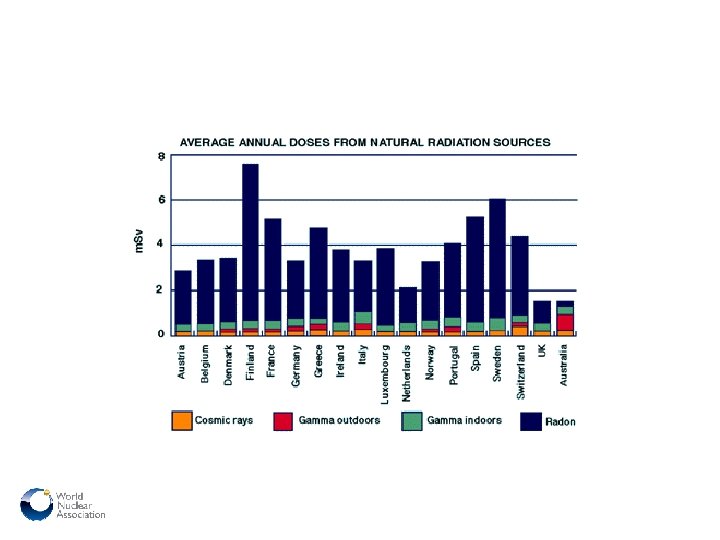
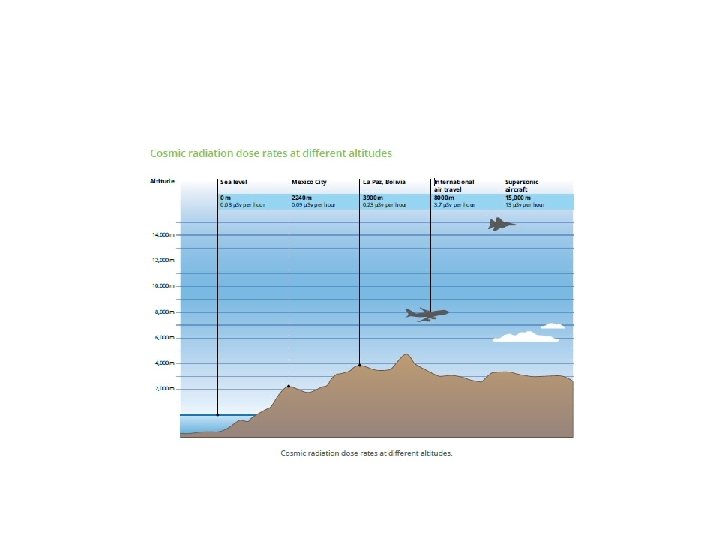
Everyone is exposed to some form of ionizing radiation from the environment in which we live. Natural background radiation • • Cosmic radiation from the earth's atmosphere Gamma radiation from the rocks and soil in the earth's crust Radiation from ingested radioisotopes, e. g. 40 K, in certain foods Radon and its decay products, 222 Rn is a gaseous decay product of uranium that is present naturally in granite. As a gas, radon diffuses readily from rocks through soil and can be trapped in poorly ventilated houses and then breathed into the lungs Artificial background radiation • Fallout from nuclear explosions • Radioactive waste discharged from nuclear establishments • Medical and dental diagnostic radiation • Radiation from occupational exposure.
Estimated annual doses from various sources of radiation: 2, 4 -3, 4 m. Sv/year • Diagnostic radiology represents the largest source of artificial radiation which is comparable to natural background exposure • Recently, patient exposure to medical and dental Xray examination has grown rapidly
Radiologic and Nuclear Medicine Studies in the United States and Worldwide: Frequency, Radiation Dose, and Comparison with Other Radiation Sources— 1950– 2007 Global annual per-capita effective radiation dose from various sources for (a) 1980 – 1984 (11) and (b) 1997– 2007 (15). Bkdbackground. Radiology: Volume 253: Number 2—November 2009 ▪ radiology. rsna. org
U. S. annual per-capita effective radiation dose from various sources for (a) 1980 and (b) 2006 by using UNSCEAR value of 2. 4 m. Sv for natural background (Bkd) (for a, NCRP 1987 estimated value, 3. 0 m. Sv; for b, NCRP 2009 estimated value, 3. 1 m. Sv). Radiology: Volume 253: Number 2—November 2009 ▪ radiology. rsna. org
Egyes repülési útvonalakon adódó sugárterhelések különböző légitársaságok mérései alapján Útvonal Zágráb - Ontarió New York - Florida Buenos Aires - Újzéland Amsterdam - Tokió Amsterdam - Milánó Helsinki - New York Koppenhága - Bangkok Koppenhága - Stockholm Brüsszel - Johannesburg Brüsszel - Tokió Frankfurt - Brakheim Frankfurt - New York Frankfurt - Chicago Budapest - New York Budapest - Beijing Budapest - Bangkok Teljes effektív dózis (μSv) 35, 1 18, 9 57, 2 55, 6 4, 8 34, 8 23, 0 2, 2 28, 4 83, 0 13, 5 30, 3 40, 4 62, 9 56, 4 37, 9 X 15 = 0, 9435 m. Sv
• The risk associated with diagnostic exposures greater than zero • For this reason it is prerequisite to measure the dose to the patients in the diagnostic radiology precisely. • The radiation dose to the patients should be as low as reasonably achievable, a principle known as ALARA (International Commission on Radiological Protection) • The number of diagnostic examinations should also be taken into consideration because the risk is directly proportional to the frequency of X-ray exposure.
How can you reduce external radiation exposure? • Time: It’s important to minimize your time of radiation exposure. • Distance: Doubling the distance between your body and the radiation source will divide the radiation shielding exposure by a factor of 4. • Shielding: Using absorber materials such as lead for X-rays and gamma rays is an effective way to reduce radiation exposures.
• Dental radiographic examinations are one of the most frequently performed radiological studies. • The effective dose delivered to patients per radiograph is low but the collective dose is significant because of the large number of radiographs made.
Effects of radiation are grouped into two categories • Deterministic– effects are based on cell killing and are characterized by a threshold dose. Below the threshold dose there is no clinical effect. With exposures above threshold dose the severity of the injury increases with dose. • Stochastic– effects, including cancer and heritable effects are based on damage to DNA. There is no-threshold or ‘‘safe’’ dose.
�Persons are medically exposed as part of their diagnostic or treatment �According to ICRP and BSS, two basic principles of radiation protection are to be complied with: justification and optimization �Dose limits are not applicable, but a guidance is given on dose levels �Investigation of exposures is strongly recommended
Three types of exposure • Medical Exposure (principally the exposure of persons as part of their diagnostic or treatment) • Occupational Exposure (exposure incurred at work, and practically as a result of work) • Public Exposure (including all other exposures)
!! ! Medical exposure ! Occupatianal exposure ! Public exposure ! ! !
The aim of radiation protection in dentistry is to obtain the desired clinical information with minimum radiation exposure to patients, dental personnel, and the public.
The aim of radiation protection in dentistry is to obtain the desired clinical information with minimum radiation exposure to patients, dental personnel, and the public. Workload?
Framework of radiological protection for medical exposure • Justification – No practice should be adopted unless its introduction produces a positive net benefit. • Optimization – All exposures should be kept as low as reasonably achievable, economic and social factors being taken into account. • The use of doses limits – The exposure of individuals should not exceed the limits recommended for the appropriate circumstances. Dose constraints and guidance (or reference) levels ARE RECOMMENDED
Three levels of justification • General level: – The use of radiation in medicine is accepted as doing more good than harm • Generic level: – Specific procedure with a specific objective (eg. chest radiographs for patients showing relevant symptoms) • Third level: – The application of the procedure to an individual patient
Generic justification (I) • It is a matter for national professional bodies, sometimes in conjunction with national regulatory authorities • The exposures to staff (occupational) and to members of the public should be taken into account • The possibility of accidental or unintended exposures (potential exposure) should also be considered • The decisions should be reviewed from time to time as new information becomes available
Justification for an individual patient (third level) • To check that the required information is not yet available • Once the procedure is generically justified, no additional justification is needed for simple diagnostic investigations • For complex procedures (such as CT, IR, etc) an individual justification should be taken into account by medical practitioner (radiologist, referral doctor. . )
The optimization of protection �Optimization is usually applied at two levels: – The design and construction of equipment and installations – Day to day radiological practice (procedures) �Reducing the patient dose may reduce the quantity as well as the quality of the information provided by the examination or may require important extra resources �The optimization means that doses should be “as low as reasonably achievable, economic and social factors being taken into account” compatible with achieving the required objective
Risk and Dosislevels
Risk of different activities (not ordered) • • • Atomenergy Smoking Antibiotics X-ray diagnostic Electrocity Cycling Food preservation Automobile Consumtion of alcoholic drinks
Risk of different activities (increasing risk) • • • Smoking Consumtion of alcoholic drinks Automobile Electrocity X-ray diagnostic Cycling Atomenergy Food preservation Antibiotics
1 micro-risk • • • 2500 km travel by train 2000 km flight 80 km by bus 65 km by car 12 km by bike 3 km by motor bike smoke of one cigarette 2 month living together with a smoker eat one more bread and butter for a fat man breath 1 hour in Budapest sleep in a house one week to be stroked by thunder in 10 years
Benifit and risk Benifit
Benifit and risk Benifit Risk
Overview of dose quantities Radiation Physical Chemical Bio-chemical Biological effect Absorbed dosis Equivalent dose RISK Effective dose • Reflects the combined detriment from stochastic effects due to the equivalent doses in all the organs and tissues of the body • The combination of probability and severity of harm is called “detriment”.
Estimated lifetime risk as a function of age
Radiation We live with 1 -3 m. Sv Can kill 4000 m. Sv Where to stop, where is the safe point? What are the effects of radiation?
Changes in Dose Limit (ICRP) m. Sv 500 450 400 350 300 250 200 150 100 50 0 1931 1947 1977 Year 1990
Dose constraints for medical exposure • For medical exposure dose constraints should only be used in optimizing the protection of persons exposed for medical research purposes, or of persons, other than workers, who assist in the care, support or comfort of exposed patients. 44
Occupational dose limits • 100 m. Sv/5 years effective dose • BUT does not allowed over 50 m. Sv in any year!
Dose Limits (ICRP 60) Occupational Effective dose Annual equivalent dose to ► Lens of eye ► Skin ► Hands & Feet 20 m. Sv/yr averaged * over 5 yrs. Public 1 m. Sv in a yr 20 m. Sv 500 m. Sv N. B. : M. P. D. 1931 = 500 m. Sv, 1947=150 m. Sv, 1977=50 m. Sv & in 1990=20 m. Sv 15 m. Sv 50 m. Sv
Dose Limits (ICRP 60) Students, trainee Effective dose Annual equivalent dose to ► Lens of eye ► Skin ► Hands & Feet 6 m. Sv/yr 15 m. Sv 150 m. Sv N. B. : M. P. D. 1931 = 500 m. Sv, 1947=150 m. Sv, 1977=50 m. Sv & in 1990=20 m. Sv
Personal Dosimetry �Personal dosimetry provides the means to measure and record radiation doses received by individual workers. �Personal dosemeters should be worn by operators who take more than 100 intra-oral films or 50 panoramic films per week. �In practice, the majority of dentists and support staff do not need to wear dosemeters although many do so as a reassurance measure.
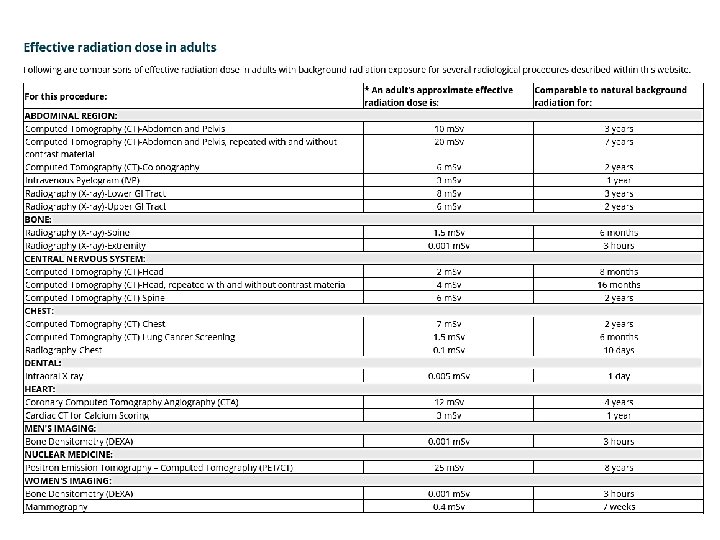
Qualitative risk levels • Negligible risk: less than 2 days of natural background exposure • Minimal risk: more than 2 days and up to 1 month of natural background exposure • Very low risk: more than 1 month and up to 8 months of natural background exposure • Low risk: more than 8 months and up to 6 years of natural background exposure • Moderate risk: more than 6 years of natural background exposure
Thank you for your attention!