Micronutrient deficiencies Prof Pushpa Raj Sharma Department of





 causes an estimated 14, 000 -20, 000 Nepalese")



 affect an estimated 10 million")








 Dose 6 mg/kg/d : infants")
 • Functions: v. Maintenance of Normal")



 causes an estimated 14,")




 Weight")








- Slides: 41
Micronutrient deficiencies Prof. Pushpa Raj Sharma Department of Child Health Institute of Medicine
• Nutrients, such as vitamins, iron, copper, and zinc, that are required in very small amounts by humans in order to survive, as distinguished from the macronutrients such as water, carbohydrate, protein and fat, that are needed in large quantities. • Micronutreints are essential to the body in small amounts because they are either components of Enzymes (the minerals) or act as coenzymes in managing chemical reactions. • Essential dietary elements required only in small quantities. They are present in the body in amounts less than. 005% of body weight.
If we could give every individual the right amount of nourishment and exercise, not too little and not too much, we would have found the safest way to health. Hippocrates
Commonest micronutrient deficiencies • The World Health Report published recently by WHO cites iron, vitamin A and iodine deficiencies as three of the most prevalent and critical nutrient deficiencies in the world.
Burden of the disease Globally: • Between 100 and 140 million children are vitamin A deficient • Anemia, mostly due to iron deficiency, affects some 2 billion people • About 41 million infants are born every year unprotected from losses in IQ or more severe mental retardation due to iodine deficiency.
Nepal: • Vitamin A deficiency (VAD) causes an estimated 14, 000 -20, 000 Nepalese children to die of infections annually. • Iodine deficiency disorders (IDD) affect an estimated 10 million Nepalese nationwide • A Goiter prevalence of 41. 5% among females and 38. 4% among males among school-aged children 6 -14 years • The anaemia prevalence was highest among infants aged 6 -11 months (90%) and during the second year of life (87. 2%), and decreased linearly with age to 59. 2% in the 48 -59 month age group.
United Nations General Assembly Special Session on Children convened in May 2002 set the following targets: • The sustainable elimination of iodine deficiency disorders by 2005; • The sustainable elimination of vitamin A deficiency by 2010; • Reducing anemia prevalence, including iron deficiency by a third by 2010; • Accelerating progress towards the reduction of other micronutrient deficiencies through dietary diversification, food fortification and supplementation.
Iodine : Micronutrient • Iodide uptake is a critical first step in thyroid hormone Synthesis. 10 to 25% of radioactive tracer (e. g. , 123 I) is taken up by the normal thyroid gland over 24 h; • Iodine deficiency, there is an increased prevalence of Goiter. • when deficiency is severe, hypothyroidism and cretinism develops. • Iodine deficiency remains the most common cause of preventable mental deficiency
Iodine deficiency world wide WHO Regions a Proportion of population with UI < 100 �g/L (%) Population with UI < 100 �g/L (in millions) b Africa 47. 6 48. 342 The Americas 14. 1 9. 995 Eastern Mediterranen 55. 4 40. 224 Europe 59. 9 42. 206 South East Asia 39. 9 95. 628 Western Pacific 19. 7 36. 082 Total 36. 9 272. 438
Iodine Deficiency prevalence in Nepal Iodine deficiency disorders (IDD) affect an estimated 10 million Nepalese nationwide A Goiter prevalence of 41. 5% among females and 38. 4% among males among school-aged children 6 -14 years
Estimated Goiter Prevalence: Note: The prevalence in the sample was assessed for grades, 1, 2, as well as TGR (total goiter rate) Group Women Sample Indicator Size 15, 540 Children 15, 542 6 -11 yrs (school aged children) Visible or palpable goiter (grades 1 and 2) Prevalence in Sample Population Affected* G 1 G 2 48. 1 1. 3 TGR 50. 0 2, 887, 515 40. 5 0. 0 40. 5 1, 328, 648 The Nepal Micronutrient Status Survey was completed in 1998.
Iodine requirement To meet iodine requirements, the current recommended daily iodine intakes are: • 50 mg for infants (first 12 months of age) • 90 mg for children (2 -6 years of age) • 120 mg for school children (7 -12 years of age) • 150 mg for adults (beyond 12 years of age) • 200 mg for pregnant and lactating women
Prevention of Iodine Deficiency There is legislation governing IDD in Nepal. It was passed in 1955 and has been revised since. Salt iodization is mandatory at the level of 20 -60 ppm. The estimated percent of households consuming salt with some iodine is 91%. The estimate of households consuming adequately iodized salt (15 ppm or above) is 63%. Sourced from the Between Census Household Information, Monitoring and Evaluation System 2000 - BCHIMES.
Iron: Micronutrient • Most Abundant Trace element in body • Functions v. Structure of hemoglobin & Myoglobin: O 2 & CO 2 Transport v. Oxidative Enzymes v. Cytochrome C v. Catalase v. Peroxidase v. MAO (neurotransmitters)
• Causes Deficiency – Inadequate intake/ Poor bioavailability/ Infections/ Chronic blood loss/Decreased absorption – Increased Demand (young children/ preg. & Lactation) • Manifestations IDA : End stage of long process: Tip of iceberg Stage Manifestation Diagnosis Early Storage iron depletion N- Hb/Serum iron Ferritin/ marrow & liver iron Second Iron limited erythropoiesis N- Hb Ferritin/ TIBC Third Iron Deficiency Anemia Hb/Ferritin/Serum iron, MC/HC Anemia
The cutt-offs for haemaglobin and haemocrit which are used to define anemia in people living at sea level: • Population Group. Haemoglobin(g/d. L) Haemocrit(%) • Children 6 months to 5 years 11. 033 Children 5 -11 Years 11. 534 • Children 12 -13 years 12. 036 • Non-pregnant women 12. 036 • Pregnant women 11. 033 • Men 13. 039
Prevalence of Anaemia in Nepal MOH/USAID Sharma PR, Baral MR, Khetan BK 1975 National 1985 MOH, Child 1998 Health Division 6 -23 months 24 -71 months 319 946 19. 5 25. 7 Kanti Children’s Hospital 0 -1 1 -4 5 -14 1000 65. 25 59. 44 47. 93 National 6 -11 months 12 -23 months 24 -35 months 36 -47 months 549 1220 978 637 90 87. 2 74. 9 70. 2 48 -59 months 515 59. 3
Prevention of Iron Deficiency • Supplementation with medicinal iron - Pregnant women/ infants/ preschool children • Increasing dietary intake - promoting breast feeding/ timely introduction of weaning foods • Enhancing bioavailability - Vit. C, tannins & phytates • Control of infections - Feeding during illness/ Deworming • Food fortification
Iron doses Oral iron therapy ( safe, cheap, effective) Dose 6 mg/kg/d : infants & children 60 -120 mg/d: adolescents and adults - Parenteral thearapy (not very safe but ensures compliance)
Vitamin A: Micronutrient • First Vitamin Discovered (1913) • Functions: v. Maintenance of Normal Vision v. Growth, Repair and Cell Differentiation v. Health of Epithelial Cells v. Pregnancy and Fetal Development v. Protection Against Infection
Deficiency • Causes – Inadequate intake/ Infections/ Measles • Manifestations – – – – XN Night Blindness (Earliest manifestation) X 1 A Conjunctival xerosis X 1 B Bitot’s Spots X 2 Corneal xerosis X 3 A Corneal ulcer/Keratomalacia < 1/3 X 3 B Corneal ulcer/Keratomalacia > 1/3 XF Fundal changes XS Corneal Scarring
Prevalence of Vit A deficiency Nepal: preschool children Age group number cases % Number cases % 6 -11 0 0 0. 00 1995 0 0. 00 11 -23 4457 3 0. 07 4534 2 0. 04 24 -35 4305 8 0. 19 4348 10 0. 23 36 -47 3455 18 0. 52 3470 21 0. 61 48 -59 3084 14 0. 45 3102 24 0. 77 National 15307 42 0. 27 17455 57 0. 33 Night blindness Bitot’s Spot Nepal mocronutrient status survey 1998
Prevalence of Vit A deficiency Nepal: school children
Burden of Disease in Nepal • Vitamin A deficiency (VAD) causes an estimated 14, 000 -20, 000 Nepalese children to die of infections annually.
Vitamin A requirement Infants< 6 -12 months of age only if not breastfed (breast fed children in this group should be protected by post partum supplementation of their mothers. ) Infants 6 -12 months of age 50, 000 IU orally Children> 12 months of age 200, 000 IU orally, every 4 -6 months Mothers (post-partum, lactating) 200, 000 IU orally within 8 wks of delivery 100, 000 IU orally, every 4 -6 months
Zinc : Micronutrient • In 1958, a 21 year old male patient in the Iranian city of Shiraz. • In 1974 the Food and Nutrition Board of the US National Academy of Sciences • The immunological effects of zinc deficiency during the late 1960 s. • BMJ 2003; 326: 409 -410 ( 22 February ) Ananda S Prasad Editorials
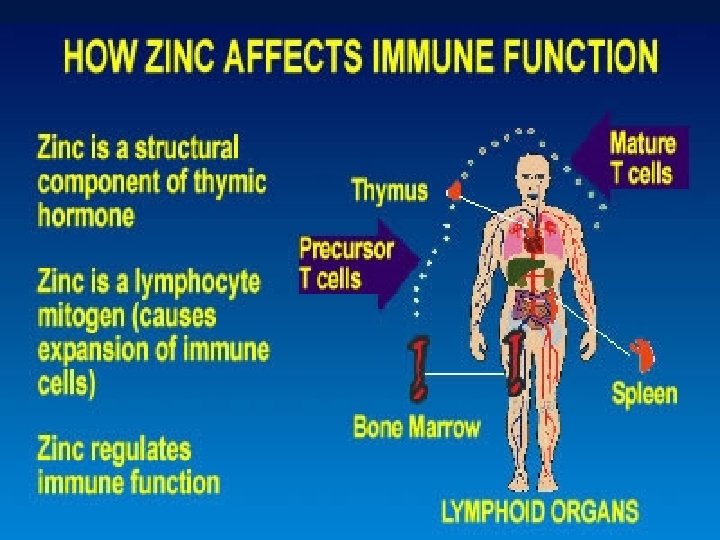
Zinc • 3 rd most abundant trace element in body • There are no zinc stores in the body to mobilize from, and in 16 hours an animal can be deficient with rapid effects. • Functions: v Metabolism (functions in over 200 enzymatic reactions) v Antioxidant function v Immunity and Wound healing v Fetal Growth and Development
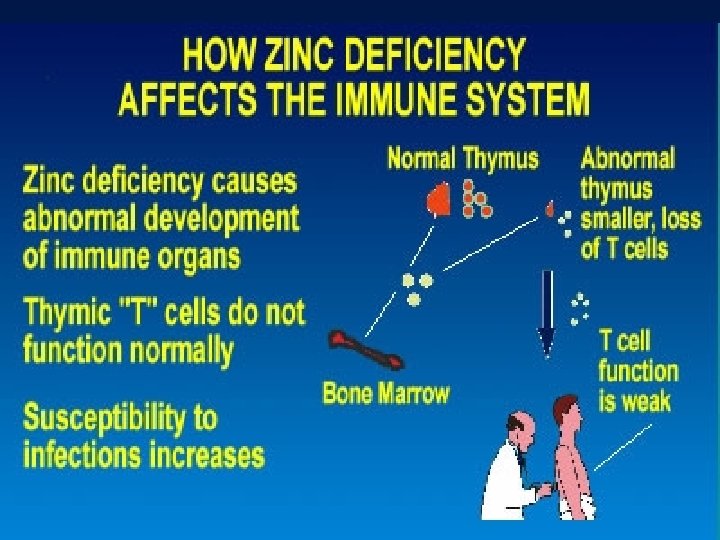
Zinc and its effect When pregnant mice were fed a diet moderately deficient in zinc, their offspring exhibited a malfunctioning immune system for the first six months of life. More alarming, the second and third generations also showed signs of poor immunity - even though they were fed a zinc-plentiful diet. Jean Carper, writing in Jean Carper's Total Nutrition Guide, in reference to zinc studies done at U. C. Davis
Symptoms of Zinc Deficiency Delayed skeletal maturation and defective mineralization of bone (monkeys) Weight loss Intercurrent infections Hypogonadism in males Lack of sexual development in females Growth retardation Dwarfism • Delayed puberty in adolescents • Rough skin • Poor appetite • Mental lethargy • Delayed wound healing • Short stature • Diarrhea • Pneumonia • Stretch marks (striae)
Symptoms of Zinc Deficiency • White spots on fingernails • Reduction in collagen turnover and synthesis (in chicks) • Reduction in collagen (in humans) • Poor Immune system • Acne • Cross-linking of collagen • Hyaluronic acid abnormalities (in swine) • Defective connective tissue • Macular degeneration • Cataracts (in salmon)
Deficiency • Severe Deficiency – Acrodermatitis enteropathica – Syndrome of hypogonadism, stunting, anemia, anorexia and hepatosplenomegaly • Mild/Subclinical Deficiency True estimate: currently not possible : Lack of valid marker for nutriture ? common in children/women developing world – susceptibility to infection/ wound-healing time. – ? Growth retardation/? Pregnancy related complications and LBW
Vitamin A and zinc are micronutrients known to be important in the maintenance of normal immune function Zinc deficiency is associated with chronic diarrhea, growth failure, and immune deficiency. Supplementation resulted in a 23 percent reduction (95 percent confidence interval, 12 to 32 percent) in the risk of continued diarrhea and a 39 percent reduction (95 percent confidence interval, 6 to 70 percent) in the mean number of watery stools per day. Tomkins A, Behrens R, Roy S. The role of zinc and vitamin A deficiency in diarrhoeal syndromes in developing countries. Proc Nutr Soc 1993; 52: 131 -142.
Three Recommended Daily Allowances of zinc given daily by caretakers or by field workers substantially reduced theduration of diarrhea. . Strand TA, Chandyo RK, Bahl R, Sharma PR, Adhikari RK, Bhandari N, Ulvik RJ, Molbak K, Bhan MK, Sommerfelt H. Pediatrics. 2002 May; 109(5): 898 -903. An emphasis on the costs and economic benefits of an alternative therapy is an important aspect of health services research. The cost savings and theattractive cost-effectiveness indicates the need to further assess the role of micronutrients such as zinc and copper in the treatment of acute diarrhea in a larger and more varied population Patel AB, Dhande LA, Rawat MS. Cost Eff Resour Alloc. 2003 Aug 29; 1(1): 7.
Zinc in growth and respiratory infection • Zinc-deficient Bangladeshi infants showed improvements in growth rate and a reduced incidence of acute lower respiratory infection after zinc supplementation. In infants with serum zinc concentrations > 9. 18 micro mol/L, supplementation improved only biochemical zinc status. Osendarp SJ, Santosham M, Black RE, Wahed MA, van Raaij JM, Fuchs GJ. Am J Clin Nutr. 2002 Dec; 76(6): 1401 -8.
Safe Upper Limit of Zinc Intake • 0. 5 -1 yr • 1 -6 yr • 10 -12 yr 13 mg/d 23 mg/d 32 mg/d 34 mg/d Girls Boys Trace elements in human nutrition and health. Geneva. WHO 1996.
Intestinal Diseases and micronutrients Three months after treatment, significant differences in serum copper, zinc and magnesium were seen in patients with E. VERMICULARIS infection, and in serum magnesium levels in patients with G. LAMBLIA. Olivares JL, Fernandez R, Fleta J, Rodriguez G, Clavel A. Serum mineral levels in children with intestinal parasitic infection Dig Dis. 2003; 21(3): 258 -61 Children with inflammatory bowel disease have abnormal levels of the trace elements which is more marked in those with Crohn's disease The reduced free radical scavenging action of zinc and selenium as a result of their deficiency may contribute to the continued inflammatory process of IBD. Ojuawo A, Keith L. The serum concentrations of zinc, copper and selenium in children with inflammatory bowel disease. Cent Afr J Med. 2002 Sep-Oct; 48(9 -10): 116 -9.
The doctor of the future will give no medication, but will interest his patients in the care of the human frame, diet and in the cause and prevention of disease. Thomas A Edison Thank you