Hyponatremia Lecture 4 Hyponatremia is a condition that


 are")















 – hypotension, nausea/vomiting")

 – Water shifts from the intracellular to the extracellular compartment, with")
 > In the hyperglycemia patients there is always higher osmolality compared")



- Slides: 28
Hyponatremia Lecture 4
Hyponatremia is a condition that occurs when the level of sodium in your blood is abnormally low. Sodium is an electrolyte, and it helps regulate the amount of water that's in and around your cells. In hyponatremia, body's water levels rise, and cells begin to swell. This swelling can cause many health problems, from mild to life-threatening. – Commonly defined serum sodium concentration is 135 -145 mmol/L – Hyponatremia represents a relative excess of water in relation to sodium. – Mostly in elders due to cardiac, hepatic or renal problems, – Healthy one can have hyponatremia only due to excess of water intake compare to water excreted
Hyponatremia • Epidemiology • Acute hyponatremia (developing rapidly, in 48 h or less) are subject to more severe degrees of cerebral edema, brain swelling and can lead to coma • Cerebral edema or cerebral oedema is excess accumulation of fluid in the intra/extracellular spaces of the brain. – sodium level is less than 105 mmol/L, the mortality is over 50% • Chronic hyponatremia (developing gradually, in days or weeks) experience milder degrees of cerebral edema – Brainstem herniation has not been observed in patients with chronic hyponatremia
Morbidity vs Mortality Morbidity refers to the state of being diseased or unhealthy within a population. Mortality is the term used for the number of people who died within a population. Fistula In medicine, a fistula is an abnormal connection between two hollow spaces (technically, two epithelialized surfaces), such as blood vessels, intestines, or other hollow organs. Fistulas are usually caused by injury or surgery, but they can also result from an infection or inflammation. Fistulas are generally a disease condition, but they may be surgically created for therapeutic reasons.
Edema, an accumulation of an excessive amount of watery fluid in cells, tissues, or body cavities. Oedematous refer to a tissue with an excess of interstitial fluid; fluid-filled.
Hyponatremia • Physiology – Serum sodium concentration regulation: • stimulation of thirst • secretion of ADH • renal handling of filtered sodium
Hyponatremia • Physiology Cont. – Stimulation of thirst • Osmolality increases – Main driving force – Only requires an increase of 2 - 3% • Blood volume or pressure is reduced – Requires a decrease of 10 - 15% • Thirst center is located in the anteriolateral center of the hypothalamus – Respond to Na. Cl and angiotensin II
Hyponatremia www. merricks. com/tech_electrolyte_new. htm
Hyponatremia • Pathophysiology – hyponatremia can only occur when some condition impairs normal free water excretion – acute drop in the serum osmolality: • neuronal cell swelling occurs due to the water shift from the extracellular space to the intracellular space • Swelling of the brain cells elicits 2 responses for osmoregulation, as follows: – It inhibits ADH secretion and hypothalamic thirst center – immediate cellular adaptation
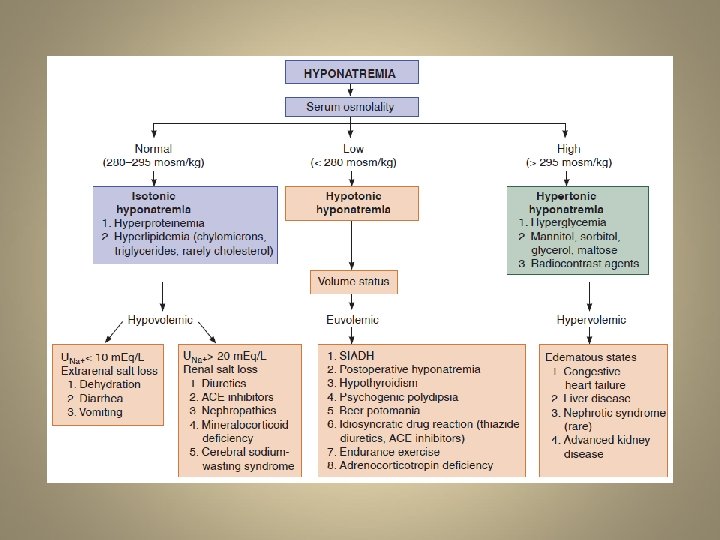
Hyponatremia • Types based on blood volume – Hypovolemic hyponatremia – Iso/Euvolemic hyponatremia – Hypervolemic hyponatremia Types based on Osmolality – Redistributive hyponatremia (Hypertonic) – Pseudohyponatremia
Hypovolemic hyponatremia • Decreased total body water and total body sodium (sodium more decreased than water). • Symptoms and signs resemble those in dehydration: prolonged skin turgor, dark urine, loss of body weight, tiredness, headache • develops as sodium and free water are lost and/or replaced by inappropriately hypotonic fluids • Sodium can be lost through renal or non-renal routes www. grouptrails. com/. . . /0 -Beat-Dehydration. jpg
Hypovolemic hyponatremia • Non-renal loss – GI losses • Vomiting, Diarrhea, fistulas, pancreatitis – Excessive sweating – Cerebral/Renal salt-wasting syndrome (C/RSW) • traumatic brain injury, and intracranial surgery • Must distinguish from SIADH (syndrome of the inappropriate antidiuretic Hormones) encountered in infections, malignancy, chest diseases, trauma, surgery etc.
Clinical Findings Common to both SIADH and RSW Association with intracranial disease Hyponatremia Concentrated urine Urine sodium [Na] usually >20 m. Eq/L Non-edematous Hypouricemia, with increased fractional excretion urate (FEurate) Only Difference between SIADH and RSW ECFV Volume state: normal/high in SIADH low in RSW
Chlorine is a deadly poison gas employed on European battlefields in World War I. Sodium is a corrosive metal, which burns upon contact with water. Together they make a placid and unpoisonous material, table salt. Why each of these substances has the properties it does is a subject called chemistry. — Broca's Brain, Carl Sagan, 1934– 1996, American astronomer, astrophysicist, author, and cosmologist The recommendation to treat virtually all hyponatremics exposes the need to resolve the diagnostic and therapeutic dilemma of deciding whether to water restrict a patient with the syndrome of inappropriate antidiuretic hormone secretion (SIADH) or administer salt and water to a renal salt waster.
Hypovolemic hyponatremia • Renal Loss – Acute or chronic renal insufficiency – Diuretics ; any substance that promote urination www. ct-angiogram. com/images/renal. CTangiogram 2. jpg
Iso/Euvolemic hyponatremia • Increased total body water, normal total body sodium, isovolemia or mild hypervolemia. Symptoms: no dehydration or edema • It is the most common and accounts for 60% of all cases of hyponatremia. The commonest cause of euvolemic hyponatremia is Syndrome of inappropriate secretion of Anti diuretic hormone (SIADH). • Plasma sodium concentration (PNa) is given by ratio of the body's content of exchangeable sodium and potassium (Na. E and KE) and total body water (TBW): PNa ≈ Na. E + KE/TBW depends on urine volume. Urine volume cannot be increased in SIADH. This occurs because of defects in Antidiuretic hormone (ADH, arginine vasopressin) secretion.
Iso/Euvolemic hyponatremia Psychogenic polydipsia, often in psychiatric patients Primary polydipsia Is characterized by increase in thirst and is most often seen in patients with psychiatric illnesses. Normally the thirst threshold is equal to or a few mmol/L higher than that for ADH. Hence, ADH is suppressed once ADH threshold is reached. However; in the osmotic threshold for thirst is reduced below the threshold for ADH release. The patients continue to drink until the thirst threshold. However; fall in plasma osmolality suppresses ADH secretion with diuresis. This causes continued stimulation of thirst. Thus normal osmolality is not achieved. Excess water is thus excreted and hence serum sodium concentration is normal or only slightly reduced and hence these patients are usually asymptomatic or may have polydipsia and polyuria. Administration of hypotonic intravenous or irrigation fluids in the immediate postoperative period
Iso/Euvolemic hyponatremia • Exercise-associated Euvolemic hyponatremia • Marathon runners may develop severe hyponatremia due to excessive water intake associated with persistent ADH secretion in some. • Low dietary solute intake • Beer drinkers or other malnourished patients (those with lowprotein, high water intake diets) have a marked reduction in water excretory capacity despite suppressed ADH. – Infants who may have been given inappropriate amounts of free water – bowel preparation before colonoscopy or colorectal surgery
Iso/Euvolemic hyponatremia • Triggers: – Severe hypovolemia (decrease in blood volume) – hypotension, nausea/vomiting • Causes: – Pulmonary Disease pneumonia, TB – Cerebral Diseases • Temporal arteritis, meningitis (meninges is the membrane around brain and spinal cord), encephalitis – Medications • Antipsychotics
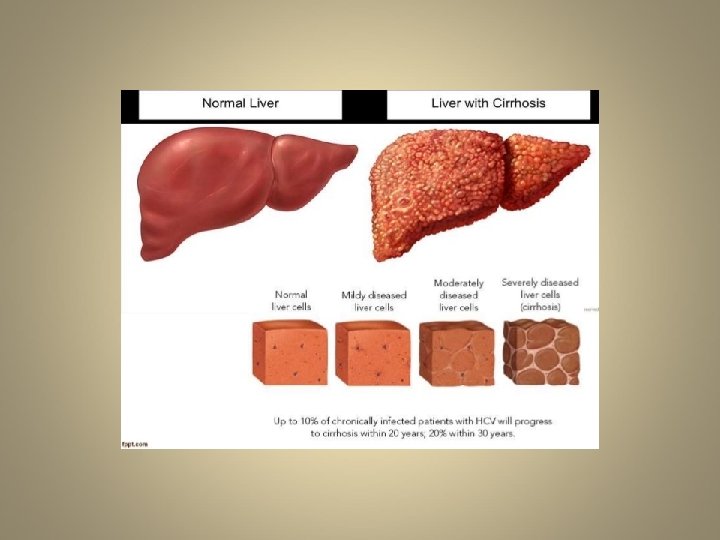
Hypervolemic hyponatremia • Greatly increased total body water, normal total body sodium. Symptoms: edema. • It is seen in congestive heart failure and cirrhosis of liver, nephrotic syndrome and chronic kidney disease. • Even though the plasma and extracellular volumes is increased in heart failure and cirrhosis, there is ADH stimulation. • Total body sodium increases, and TBW increases to a greater extent. • Can be renal or non-renal – acute or chronic renal failure • dysfunctional kidneys are unable to excrete the excess ingested water load (and sodium).
Redistributive hyponatremia (hypertonic) – Water shifts from the intracellular to the extracellular compartment, with a resultant dilution of sodium. The TBW and total body sodium are unchanged. • This condition occurs with hyperglycemia • Administration of mannitol (for urination or pressure reduction on brain)
Redistributive hyponatremia (hypertonic) > In the hyperglycemia patients there is always higher osmolality compared to a normal person which lead to low Na concentration in the ECF and thus lead to condition of hypertonic hyponatremia > Due to transcellular shifting of water, Na level is low but the measured serum osmolality is high Ø Glucose is an effective osmole which casuses excessive movement of the water from intracellular compartment into the extracellular compartemnt, thus reducing the sodium level in the extracellular compartment Ø Mannitol administration can also lead to the same hypertonic condition
• Pseudohyponatremia • Artifactualy low sodium conc. in Hyperlipidemia, hyperproteinemia patients • Reduction of water in plasma due to high lipid or protein conc. lead to high Na conc. • Plasma is 93% water and 7% protein and lipid – The aqueous phase is diluted by excessive proteins or lipids. The TBW (total body water) and total body sodium are unchanged (normal sodium concentration). • hypertriglyceridemia • multiple myeloma
• Serum osmolality does not changes as lipids and proteins are not dissolved in the plasma fraction. This condition is known as pseudohyponatremia • This will lead to increase in osmolal gap. • Normal osmolality with serum Na 110 mmol/L? • So clinicians should be aware of this and therefore normally sodium electrodes are used to measure exact Na level
Brief summary Hyponatremia results from the inability of the kidney to excrete a water load or excess water intake. Water intake depends upon thirst mechanism. Thirst is stimulated by increase in osmolality. Thirst is sensed by osmoreceptors located in the hypothalamus and leads to the release of anti-diuretic hormone (vasopressin) from the posterior pituitary.