HYPONATREMIA HYPERNATREMIA by M S Mojtabavi Hypernatremia Plasma

HYPONATREMIA & HYPERNATREMIA by: M. S. Mojtabavi

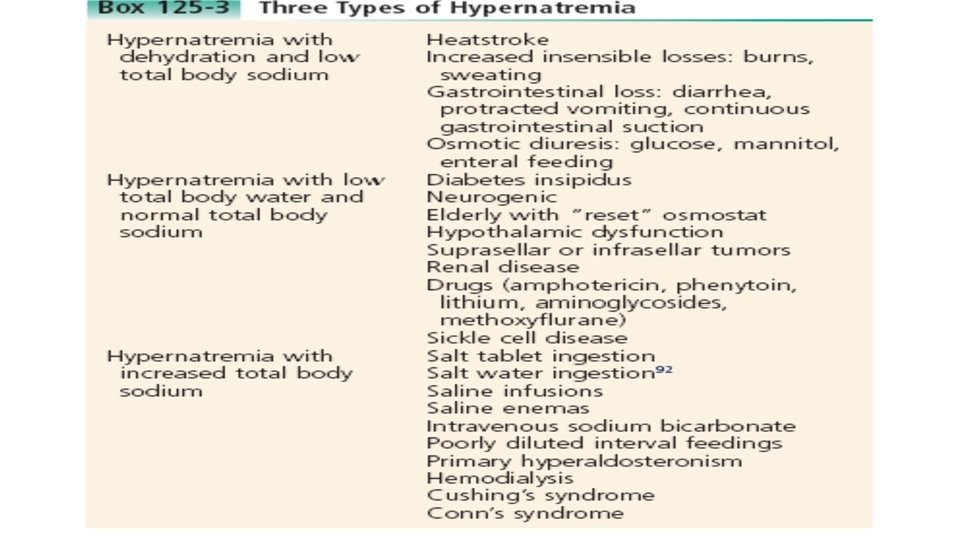
Hypernatremia – Plasma Na+ > 145 m. Eq / L – Due to ↑ Na + or ↓ water Due to: – Excess Na intake (hypertonic IV solution) – Excess Na retention (oversecretion of aldosterone) – Loss of pure water • Long term sweating with chronic fever • Respiratory infection Diabetes (mellitus or insipidus) – polyuria – Insufficient intake of water (hypodipsia)

Clinical manifestations of Hypernatremia • • • Thirst Lethargy Irritability Seizures Fever Oliguria

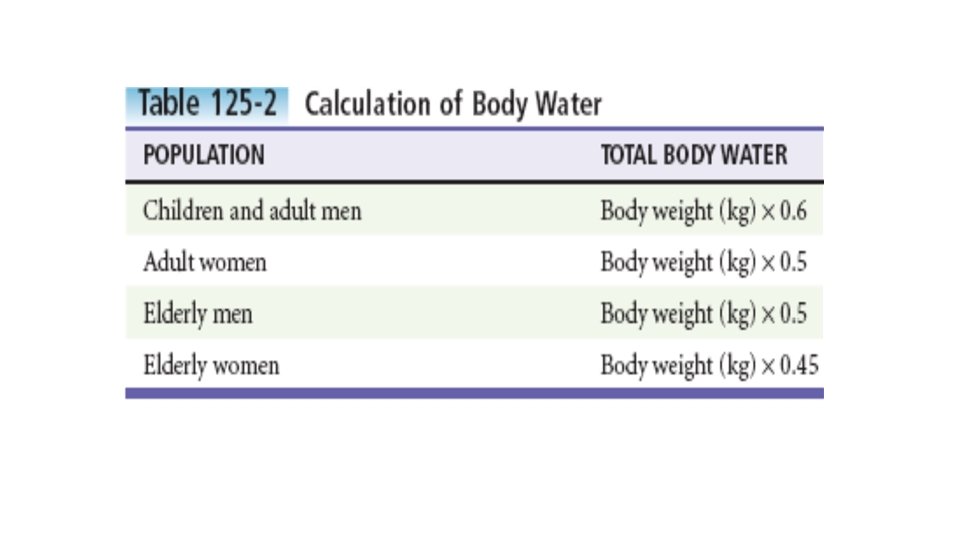
Diagnostic Strategies • In addition to routine serum chemistries, serum osmolarity and • urine sodium concentration and osmolality should be obtained. • The degree of hypernatremia almost always equals the total body • water deficit in adults. • TBW deficit = TBW×(serum Na+ /140)− 1

• The rate of correction in hypernatremia is extremely important to minimize morbidity and mortality. In adult patients who have had hypernatremia during a short time as a result of sodium loading, “rapid correction” at 1 to 2 m. Eq/hr lowering of serum sodium appears relatively safe. • However, most adult patients have hypernatremia during days to weeks. In this group of patients, serum sodium concentration should be slowly corrected at no more than 0. 5 m. Eq/hr or 10 to 12 m. Eq/day.

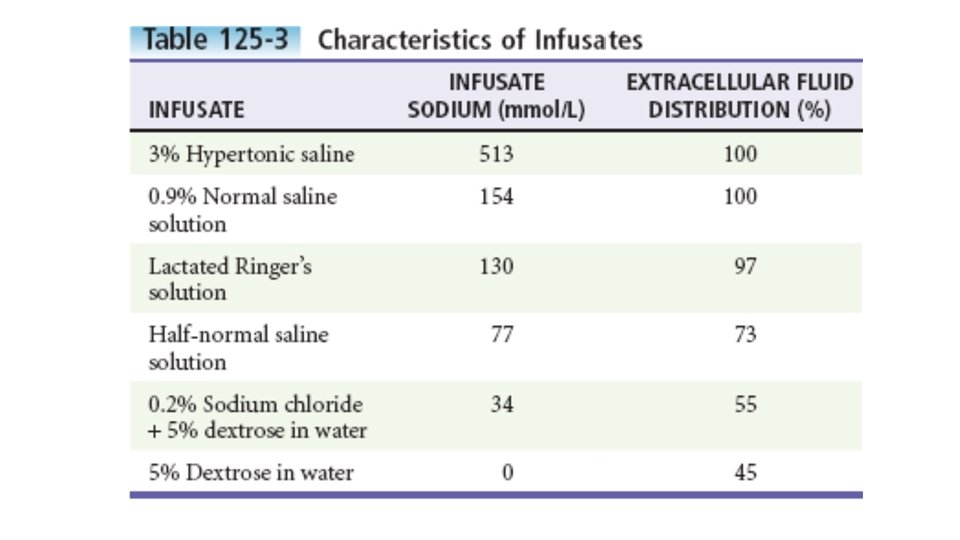
• Normal saline can typically be started for volume replacement until the patient is hemodynamically stable and then changed to half-normal saline at 100 m. L/hr once vital signs have normalized. • The treatment of central diabetes insipidus with desmopressin (DDAVP) is an effective means of improving polyuria and hypernatremia; initial doses in the acute setting range from 1 to 2 μg.

So let’s do a sample calculation: • 60 kg woman with 168 m. Eq/L • Water deficit = 0. 4 x 60 ([168/140]-1) = 4. 8 L • sodium should not be lowered by more than 12 m. Eq/L in 24 hours • Overcorrection can lead to cerebral edema which can lead to encephalopathy, seizures or death • The 4. 8 L which will lower the sodium level by 28 should be given over 56 -60 hours, or at a rate of 75 -80 m. L/hr • Typical fluids given in form of D 5 water

HYPONATREMIA • Definition: – Commonly defined as a serum sodium concentration 135 meq/L • The most common causes of severe hyponatremia in adults are therapy with thiazides, the postoperative state including transurethral prostatectomy, the syndrome of inappropriate secretion of antidiuretic hormone (SIADH), polydipsia in psychiatric patients,
 with hyponatremia are asymptomatic")
• Most patients presenting to the emergency department (ED) with hyponatremia are asymptomatic and do not require emergent therapy. • Symptoms range from headache, nausea, and vomiting to confusion, seizures, and coma.

• two groups of hyponatremic patients require treatment with either normal saline or hypertonic saline: • 1) asymptomatic hyponatremia with a sodium level of 110 m. Eq/L or less • 2)acute symptomatic hyponatremia with a sodium level below 120 m. Eq/L.

HYPONATREMIA • Types • Hypovolemic hyponatremia • Euvolemic hyponatremia • Hypervolemic hyponatremia • Pseudohyponatremia
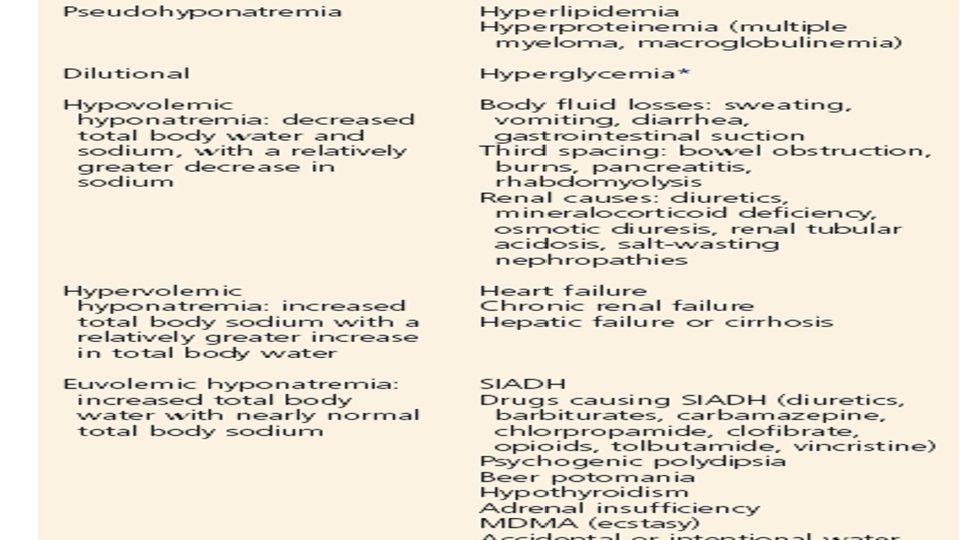

Diagnostic Strategies: • urinary sodium or urinary chloride level is useful: • Patients with hypovolemic hyponatremia due to nonrenal causes, urinary sodium or chloride level (<20 m. Eq/L) • Patients with hypovolemic hyponatremia due to renal causes , urine sodium and chloride levels above 20 m. Eq/L • Patients with euvolemic hyponatremia typically have a urinary sodium greater than 20 m. Eq/L • Patients with hypervolemic hyponatremia secondary to CHF or cirrhosis have urine sodium levels of less than 20 m. Eq/L • renal causes of hypervolemic hyponatremia or with SIADH have sodium levels in excess of 20 m. Eq/L

Diagnostic Strategies , , Plasma osmolality Urine sodium concentration , Uric acid level, Fe. Na • Plasma osmolality • normally ranges from 275 to 290 mosmol/kg • If >290 mosmol/kg : • Hyperglycemia or administration of mannitol • If 275 – 290 mosmol/kg : • hyperlipidemia or hyperproteinemia • Urine Sodium • >20 m. Eq/L • SIADH, diuretics • <20 m. Eq/L • Uric Acid Level • < 4 mg/dl consider SIADH • Fe. Na • Help to determine pre-renal from renal causes

Clinical Manifestations • most patients with a serum sodium concentration exceeding 125 m. Eq/L are asymptomatic • Patients with acutely developing hyponatremia are typically symptomatic at a level of approximately 120 m. Eq/L • Nonspecific signs of hyponatremia include anorexia, nausea, vomiting, and generalized weakness. • Acutely hyponatremic patients whose sodium level drops below 120 m. Eq/L during 24 to 48 hours may present with severe neurologic findings, including confusion, seizures, cerebral edema, coma, and brainstem herniation.

Management: • For relatively asymptomatic patients with sodium values of 115 to 135 m. Eq/ L, free water restriction is typically the single most important treatment. • In more severe cases when the sodium value is 120 m. Eq/L or less and the patient has alterations in mental status, has focal findings, or is seizing, hypertonic saline is indicated.
 = 0.")
Treatment • calculate the total body water • total body water (TBW) = 0. 6 × body weight • How much sodium does the patient need? • Sodium deficit = Total body water x (desired Na – actual Na) • critically ill hyponatremic patients with seizures, focal findings, or coma receive 100 m. L of 3% hypertonic saline during 10 minutes. If a second bolus is required, an additional 100 m. L of the 3% solution (513 m. Eq/L of sodium) may be administered during the next 50 minutes. • Goals for correction: • 1. 5 to 2 m. Eq/L per hour for first 3 -4 hours until symptoms resolve • Increase by no more than 10 m. Eq/L in first 24 hrs • Increase by no more than 18 m. Eq/L in first 48 hrs

• Hypovolemic Hyponatremia: • the normal saline is started at 500 to 1000 m. L/hr until the blood pressure is stable. • then slowed to 200 m. L/hr with frequent sodium checks. • rise only by an average of 0. 5 m. Eq/hr or 10 to 12 m. Eq/day.

• Hypervolemic Hyponatremia: • Restriction of fluid and sodium is the preferred treatment. • loop diuretics • Hemodialysi • albumin

• Euvolemic Hyponatremia: • As the hypo-osmolality in SIADH, restriction of free oral water intake is the first recommendation. • antineoplastic therapy • hypertonic saline • Demeclocycline and lithium • Vaptans • hemodialysis

an example: • 60 kg woman with sodium level of 116 • Sodium needed = 0. 5 x 60 x (124 -116) = 240 • The patient needs 240 m. Eq in next 24 hours • That averages to 10 m. Eq per hour or 20 m. L of hypertonic saline per hour • However, this will only raise the serum sodium by 0. 33 per hour therefore, increasing the rate 60 m. L to 90 m. L will produce the desired rate of serum sodium increase of 1. 0 to 1. 5 m. Eq per hour until symptoms resolve

What if the sodium increases too fast? • The dreaded complication of increasing sodium too fast is Central Pontine Myelinolysis which is a form of osmotic demyelination • Symptoms generally occur 2 -6 days after elevation of sodium and usually either irreversible or only partially reversible • Symptoms include: dysarthria, dysphagia, paraparesis, quadriparesis, lethargy, coma or even seizures

- Slides: 26