Water Homeostasis Hyponatremia James Brandes M D Carroll

Water Homeostasis: Hyponatremia James Brandes, M. D. Carroll University Sinai. EM

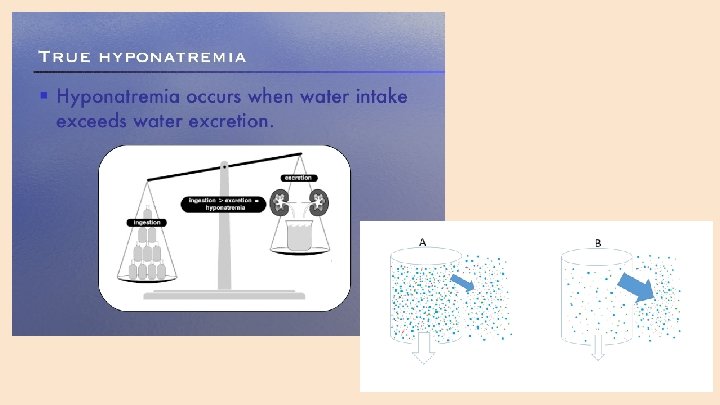
The Basics ● Na is the major extracellular determinant of the osmolality ● Osmolality is the total number of solute particles dissolved in 1 kg of solvent (water) ● Osmolarity is defined as the total number of solute particles dissolved in 1 liter of solution ● There is very little difference between the values for Osmolality and Osmolarity

Test Question #1 What is the most likely diuretic to cause hyponatremia is? ● A. Furosemide ● B. HCTZ ● C. Diamox ● D. Bumex

Test Question #2 The major complication in treatment of chronic hyponatremia can be avoided by ? ● A. Using hypertonic saline (3%) ● B. Correct the Na by 12 meq/L in the first 24 hours ● C. Water restricting the patient ● D. Correct the Na by less than 8 meq/L in the first 24 hour

Water Flow Between Cellular and Extra. Cellular Spaces ● The osmolality difference between the cellular and extra-cellular space determines direction of water flow ● Water flows freely through cell membranes always toward the compartment with the higher osmolality.

Serum Osmolarity ● The major solute particles in the extracellular compartment include Na, potassium, glucose, and blood urea nitrogen (BUN) ● The extra-cellular Sosm can be measured directly in the laboratory (measured as osmolality) ● The extra-cellular Sosm can also be calculated from a basic metabolic panel utilizing the following equation: Sosm (osmolarity) = 2(Na + K) + glucose/18 + BUN/2. 8

Serum Osmolarity ● Sosm is tightly controlled with the normal value around 285 osmoles/liter. ● Na accounts for about 95% of the total Sosm ● Changes in serum Na concentration greatly affects Sosm and water flow between the intra- and extra-cellular compartments ● An osmolal gap occurs when the measured Sosm > calculated Sosm.

Causes of Increased Osmolal Gap ● If the osmolal gap is greater than 10 (measured > calculated), a search for the un-calculated osmole should be done ○ Alcohol (Et. OH, methanol, ethylene glycol, prophylene glycol, isopropyl alcohol) ○ Ketoacids (Alcoholic, starvation, diabetic) ○ ARF ○ Lactate elevation

Tonicity ● Tonicity is the “effective serum osmolality” and refers to solutes that do NOT cross the cell membrane. ● For example, changes in Na concentration (hyponatremia) will decrease Sosm since Na is primarily in the extra-cellular space (Why? -Na/K ATPase pump), hence, extracellular osmolality is lower than the intracellular osmolality. Water thus moves into the intracellular compartment. (Decreased Sosm, decreased tonicity). ● Solutes like BUN cross the cell membrane freely, thus Sosm increases, but tonicity is unchanged, so no water movement occurs.

Tonicity Questions ● What happens to Sosm, Tonicity, and Water movement in ○ Hyperosmotic, hyperglycemic coma before treatment ○ Giving mannitol for brain swelling ○ Acute renal failure with increased BUN

Regulation of Extracellular Osmolality ● It is essential that the Sosm stay within a very specific range to avoid water shifts between the two compartments: extracellular and intracellular ● A decrease in Sosm--most commonly due to a decrease in serum Na--will cause water to flow intracellulary--most critical in brain cells ● Cerebral edema against a non-compliant cranium can result in the development of seizures, significant neurological dysfunction, brain herniation, and ultimately, death
 and the thirst")
Regulation of Extracellular Osmolality ● Osmolality is controlled by vasopressin (ADH) and the thirst mechanism ● Osmole receptors in the hypothalamus when triggered by a rising Sosm will ○ Increase thirst mechanism ○ Stimulate ADH release from the pituitary ● ADH increases free water absorption from the distal nephron in the kidney in order to normalize the Sosm ● The reverse occurs when the osmoreceptors sense a falling Sosm ● ADH release also occurs when there is a decrease in effective blood volume ○ Decreased effective blood volume stimulates the renin-angiotensin system and A -II stimulates the release of ADH, regardless of the Sosm ● ADH release can also occur in response to some medications, pain, stress, lung tumors, and brain abnormalities regardless of the Sosm--leading to hyponatremia

-Dehydration -Hypotension -Blood Loss -Heart Failure Increasing Osmolality Increase Renin-Angiotensin Release Increase ADH Release

Signs and Symptoms of Hyponatremia ● Normal Na range is 135 -145 meq/l ● Hyponatremia is defined as a Na level less than 135 meq/l ● Hyponatremia is almost always associated with hypo-osmolality and it is the extracellular fluid hypo-osmolality that promotes water movement into cells, importantly, brain cells ● In the ACUTE development of hyponatremia, symptoms of nausea and vomiting (Na levels 125 -130) are the earliest symptoms ● As Na drops further in the range of 115 -120, headache, lethargy, obtundation, seizures, coma, brain herniation, and respiratory distress can occur ● It is important to treat ACUTE hyponatremia aggressively, as will be described. If not treated, complications may be permanent

Brain Adaptations to Hyponatremia ● Brain adapts to Sosm, the initial cerebral edema increases interstitial hydraulic pressure, forcing fluid movement out of the brain into the cerebrospinal fluid ● Next, brain cells lose solutes including potassium and organic solutes (osmolytes) thus lowering the intracellular osmolality allowing the brain cells to lose water, coming back to their original volume ● These adaptations occur within the first 24 hours and up to 2 -3 days ● Once hyponatremia is being treated, the reuptake of brain solutes occurs but at a much slower rate and hence treatment much be gradual or serious complications of osmotic demylination syndrome (ODS) may occur--when treating chronic hyponatremia

New Engl J Med

Chronic Hyponatremia ● In chronic hyponatremia, the adaptive changes in the brain cells makes symptoms less urgent and many patients may be asymptomatic ● Symptoms that may occur when Na levels are below 120 meq/l include fatigue, nausea, dizziness, vomiting, gate disturbances, forgetfulness, confusion, lethargy, and muscle cramps ● Brain herniation and Seizures are rare with chronic hyponatremia
 ○")
Evaluation of Patients with Hyponatremia ● Pseudohyponatremia ○ High lipids ○ Paraproteins (myeloma) ○ Water not distributed in fat or protein, so volume appears greater that the Na is distributed in resulting in a reading of hyponatremia ○ Does NOT occur with direct potentiometry ○ May occur in flame photometry or indirect potentiometry ● Once true hyponatremia established, next question--is there other solutes (not able to pass through the cell membrane) present--like hyperglycemia in poorly controlled diabetics

Hyperosmolar-hyponatremia occurs with hyperglycemia, mannitol, glycine, immune globulin, and sorbital irrigation solutions

Evaluation of Patients with Hyponatremia ● Once pseudohyponatremia and hyperosmolar hyponatremia are ruled out, the next step in evaluation of hypotonic hyponatremia is dependent on the patient’s volume status. ● Stratify as hypovolemia, euvolemia, or hypervolemia ● A good history and physical exam is required to determine volume status ● Review patient medications including OTC meds and illicit drug use ● How much water are they drinking? ● Are they eating enough? ● Elicit any signs or symptoms of hyponatremia

Evaluation of Patients with Hyponatremia ● Initial laboratory testing, besides bmp to determine Na and calculate Sosm, includes ○ Uosm (normal greater than 200) ○ FENa to help determine volume status, reninangiotensin activity

Evaluation of Patients with Hyponatremia ● In cases where the kidney sees a low perfusion state, the FENa is less than 1% which occurs in ○ Dehydration ○ Heart Failure ○ Liver Disease ● ADH is elevated in each of these clinical situations because the reninangiotensin system is activated thus releasing ADH ● The patient develops hyponatremia in these settings. The Uosm is high.
 -Cerebral salt wasting -Adrenal insufficiency -GI losses")
Differential Diagnosis of Hyponatremia Hypovolemia -Diuretics (thiazides) -Cerebral salt wasting -Adrenal insufficiency -GI losses -Third spacing Euvolemia Hypervolemia -Hypothyroidism -Heart Failure -Ecstasy -Liver Disease -Primary polydipsia -Renal Failure -Exercise induced -Low protein diet -Beer Potomania -Tea and toast diet -SIADH -Reset osmostat

Hyponatremia: Hypovolemia ● Thiazide diuretics cause hyponatremia. Loop diuretics cause hypernatremia ● Cerebral salt wasting: Low FENa, caused from trauma to the brain, brain hemorrhages or brain surgery leading to an elevation of natriuretic peptides causing dehydration and ADH release ● Primary adrenal insufficiency: (low aldosterone), nautriuretic, high ADH ● GI losses with low FENa, high Uosm ● Third spacing: Low FENa, high Uosm

Hyponatremia: Euvolemia ● ● ● Hypothyroidism Ecstasy: MDMA causes increase thirst and ADH release, high Uosm Primary polydipsia: Low Uosm, normal FENa Exercise induced: Increase water intake, normal FENa Reset osmostat: The osmoreceptors in the hypothalamus have changed the range with which ADH is released ● Low protein intake/normal fluid intake: Low Uosm, normal FENa ○ Beer potomania ○ Tea and Toast Diet ● SIADH: High Uosm, normal FENa
")
Low Protein Diet ● Osmoles from protein need to be generated (BUN in urine) to excrete enough free water that the patient is drinking. If the patient is not taking in enough protein, they are unable to generate enough osmoles to excrete the free water in the urine that they are drinking--thus hyponatremia results ● This occurs in beer potomania where the patient drinks significant fluid but not enough protein intake to generate BUN ● This occurs in the elderly as they drink enough fluid but don’t take in enough protein to generate the osmoles (BUN) required to excrete their free water load, thus leading to hyponatremia

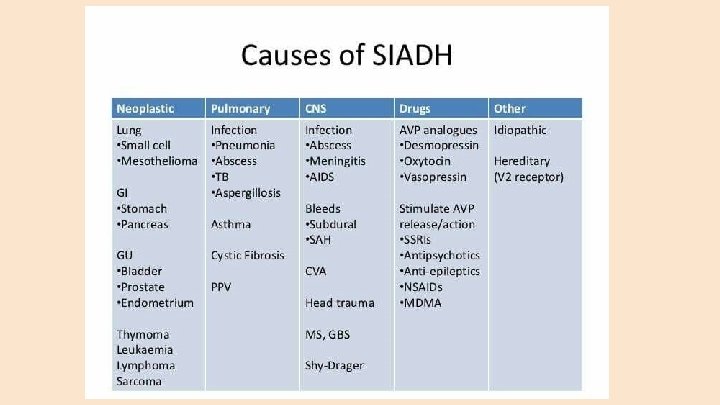
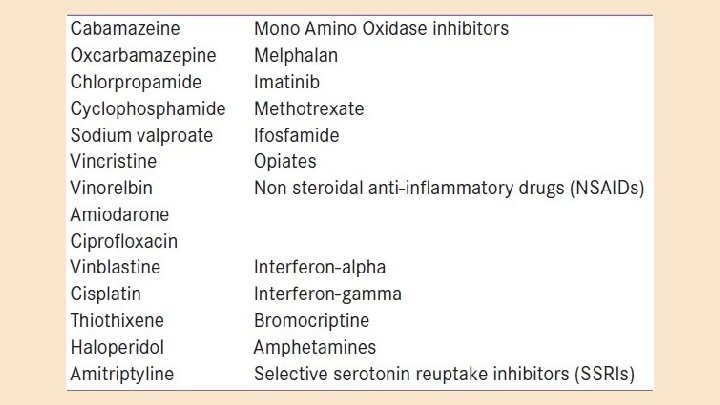
SIADH ● SIADH is an inappropriate release of ADH in clinical settings where there is no hyperosmolality or effective blood volume issue (renin-angiotensin system is not activated). ● Causes of SIADH include ○ CNS Disorders ○ Neoplasm ○ Pulmonary Disorders ○ Pain ○ Surgery ○ Drug induced ○ Psychosis

Hyponatremia: Hypervolemia ● Heart Failure: Low FENa, high Uosm ● Liver Failure: Low FENa, high Uosm ● Renal Failure: Normal Uosm, normal FENa

Treatment of Hyponatremia: The Basics ● Duration of hyponatremia needs to be determined. Acute hyponatremia develops in less than 48 hours. Chronic hyponatremia has been present for over 48 hours. If unclear, assume chronic. ● Determine severity of hyponatremia ○ Severe: Na<120 meq/L ○ Moderate: Na levels between 120 -129 meq/L ○ Mild: Na levels between 130 -134

Treatment of Hyponatremia: The Basics ● Determine severity of symptoms ○ Severe: Seizures, obtundation, coma, respiratory distress ○ Mild-Moderate: Headache, fatigue, lethargy, nausea, dizziness, forgetfulness, confusion, and muscle cramps ● Patients should be hospitalized if they have acute hyponatremia, severe hyponatremia (Na<120), or have any symptoms as listed above ● Neurological symptoms of seizures and obtundation are much more prevalent with acute hyponatremia
 prevention")
Treatment of Hyponatremia: The Goal The major goals of therapy include the (a) prevention of further declines in Na concentration, (b) decrease intracranial pressure (brain edema) to avoid brain herniation, (c) relieve the symptoms of hyponatremia-- BUT avoid excessive (rapid) correction of hyponatremia which could lead to osmotic demyelination syndrome (ODS), a major complication of treatment.
 ● Major complication of treatment for hyponatremia ● In chronic")
Osmotic Demyelination Syndrome (ODS) ● Major complication of treatment for hyponatremia ● In chronic hyponatremia, the brain has adapted to the low Sosm by decreasing intracellular water and dumping organic solutes, thus lowering the intracellular osmolality to prevent water shifts. ● In this chronic setting, correction of extracellular osmolality (Sosm)-if too rapid-- will cause water to flow out of the brain cells since they cannot readjust their osmolality as quickly (takes several days) ● This rapid fall in brain cell volume leads to demyelination, for reasons that are not clear.
 ● Symptoms of ODS include dysarthria, dysphasia, paraparesis, quadriparesis, seizures,")
Osmotic Demyelination Syndrome (ODS) ● Symptoms of ODS include dysarthria, dysphasia, paraparesis, quadriparesis, seizures, lethargy, confusion, disorientation, obtundation, and coma ● Symptoms may be delayed for 2 -6 days after treatment for hyponatremia ● Risk factors for development of ODS include ○ Initial Na of less than 120 meq/L ○ Longer duration of hyponatremia ○ Rapid correction exceeding 8 meq/L in the first 24 hours


Treatment of Acute Hyponatremia ● For treatment of acute hyponatremia with significant symptoms, the Na level should be raised 4 -6 meq/L within the first six hours to avoid worsening cerebral edema and herniation ● Never exceed a correction rate of > 8 meq/L in the first 24 hours ● Use 3% Na. Cl (513 meq/L)--hypertonic saline ○ 100 ml boluses given up to 3 times over 30 minutes to avoid brain herniation ○ Monitoring serum Na level q 1 -2 hours is essential to adjust actual rate of correction ● Treat underlying cause of hyponatremia

Treatment of Chronic Hyponatremia ● In asymptomatic patients with Na levels 130 -134 --determine the underlying cause and treat that (i. e. stopping the drug that causes SIADH, stopping the thiazide diuretic), no need to hospitalize ● In moderate hyponatremia with mild to moderate symtoms, would admit and monitor Na, treat underlying cause of hyponatremia ● In patients with mild to moderate symptoms of hyponatremia and a Na level < 120 meq/L ○ 3% Na. Cl at rate of 15 -30 ml/hour ○ Monitor serum Na (every 1 -2, as necessary), and adjust rate of 3% Na. Cl ○ Goal is to correct Na level by no more than 4 -6 meq/L in the first 24 hours ● For chronic hyponatremia with severe symptoms, treat with boluses like in acute hyponatremia to avoid brain edema, but total correction should not exceed 6 -8 meq/L in the first 24 hours

Treatment of Hyponatremia ● Shoot for a correction 4 -6 meq/L in first 24 hours but NEVER exceed 8 meq/L in first 24 hours ● Treating the underlying cause of hyponatremia may result in too rapid of a correction with or without using hypertonic saline. In this instance, maneuvers to lower the rate of rise may be required ○ D 5 W ○ ADH agonist, DDAVP, desmopressin ● Rapid auto-correction of hyponatremia occurs in patients who have hyponatremia due to polydipsia, dehydration, drugs causing SIADH, and thiazide-induced. In these situations, desmopressin may be given at the outset

Treatment of Hyponatremia ● In addition to removing/treating the underlying cause of the hyponatremia, subsequent therapy after the first 24 hours includes ○ Continued monitoring of serum Na level ○ Fluid restriction in edematous/fluid overloaded states ○ Loop diuretics in edematous states ○ Protein supplementation in beer potomania and tea and toast diets ○ Treat endocrine disorders ● Use of demeclocycline and ADH antagonists (tolvaptan) in selected patients with chronic hyponatremia in which the underlying cause cannot be treated

Case 1 24 yo presents to ER with confusion and his family noticed tonic-clonic seizures that lasted approximately 3 minutes. He is lethargic and unable to report a history. He has bipolar disorder for which he takes Depakote per his family. He is on no other medications. On exam, his vitals are normal and he is euvolemic. On analysis, his Na level is 110 meq/L, other electrolytes normal, renal function normal. His Uosm was only 75 m. Osm/Kg and his FENa was 2%. a) How would you classify his hyponatremia? b) What is the differential diagnosis for his hyponatremia? Most likely?
 -Cerebral salt wasting -Adrenal insufficiency -GI losses -Third spacing Euvolemia Hypervolemia")
Hypovolemia -Diuretics (thiazides) -Cerebral salt wasting -Adrenal insufficiency -GI losses -Third spacing Euvolemia Hypervolemia -Hypothyroidism -Heart Failure -Ecstasy -Liver Disease -Primary polydipsia -Renal Failure -Exercise induced -Low protein diet -Beer Potomania -Tea and toast diet -SIADH -Reset osmostat
 Classify the severity of his hyponatremia, and his symptoms d)")
Case 1, continued c) Classify the severity of his hyponatremia, and his symptoms d) How would you treat him? e) During treatment, what complications could occur? What might you do in order to decreae the risk of these complications.

● In asymptomatic patients with Na levels 130 -134 --determine the underlying cause and treat that (i. e. stopping the drug that causes SIADH, stopping the thiazide diuretic), no need to hospitalize ● In moderate hyponatremia with mild to moderate symtoms, would admit and monitor Na, treat underlying cause of hyponatremia ● In patients with mild to moderate symptoms of hyponatremia and a Na level < 120 meq/L ○ 3% Na. Cl at rate of 15 -30 ml/hour ○ Monitor serum Na (every 1 -2, if necessary), and adjust rate of 3% ○ Goal is to correct Na level by no more than 4 -6 meq/L in the first 24 hours ● For chronic hyponatremia with severe symptoms, treat with boluses like in acute hyponatremia to avoid brain edema, but total correction should not exceed 6 -8 meq/L in the first 24 hours
 Classify the severity of his hyponatremia, and his symptoms d) How would you")
c) Classify the severity of his hyponatremia, and his symptoms d) How would you treat him? e) During treatment, what complications could occur? What might you do in order to decreae the risk of these complications.

● Treating the underlying cause of hyponatremia may result in too rapid of a correction with or without using hypertonic saline. In this instance, maneuvers to lower the rate of rise may be required ○ D 5 W ○ ADH agonist, DDAVP, desmopressin ● Rapid auto-correction of hyponatremia occurs in patients who have hyponatremia due to polydipsia, dehydration, drugs causing SIADH, and thiazide-induced. In these situations, desmopressin may be given at the outset

Case 2 An 87 yo woman presents to your office with frequent falls, increasing forgetfulness, and dizziness. She lives alone as her family checks on her about once per week. Her PMH is significant for HTN, arthritis, and hyperlipidemia. Her medications include HCTZ, motrin, and zocor. On exam, her vitals are normal and she is euvolemic. She is not orthostatic. Her Na level is 126, electrolytes otherwise normal. She has normal kidney function. Her albumin is low at 2. 5 g/dl, and her BUN is only 2 mg/dl. Her FENa is 2 % and her Uosm is 85 m. Osm/kg.
 How would you classify her hyponatremia? b) What is the")
Case 2, continued a) How would you classify her hyponatremia? b) What is the differential diagnosis for her hyponatremia? Most likely? c) Could her symptoms be associated with this degree of hyponatremia? d) How would you treat this patient’s hyponatremia?
 -Cerebral salt wasting -Adrenal insufficiency -GI losses -Third spacing Euvolemia Hypervolemia")
Hypovolemia -Diuretics (thiazides) -Cerebral salt wasting -Adrenal insufficiency -GI losses -Third spacing Euvolemia Hypervolemia -Hypothyroidism -Heart Failure -Ecstasy -Liver Disease -Primary polydipsia -Renal Failure -Exercise induced -Low protein diet -Beer Potomania -Tea and toast diet -SIADH -Reset osmostat

● In asymptomatic patients with Na levels 130 -134 --determine the underlying cause and treat that (i. e. stopping the drug that causes SIADH, stopping the thiazide diuretic), no need to hospitalize ● In moderate hyponatremia with mild to moderate symtoms, would admit and monitor Na, treat underlying cause of hyponatremia ● In patients with mild to moderate symptoms of hyponatremia and a Na level < 120 meq/L ○ 3% Na. Cl at rate of 15 -30 ml/hour ○ Monitor serum Na (every 1 -2, if necessary), and adjust rate of 3% ○ Goal is to correct Na level by no more than 4 -6 meq/L in the first 24 hours ● For chronic hyponatremia with severe symptoms, treat with boluses like in acute hyponatremia to avoid brain edema, but total correction should not exceed 6 -8 meq/L in the first 24 hours

Test Question #1 What is the most likely diuretic to cause hyponatremia is? ● A. Furosemide ● B. HCTZ ● C. Diamox ● D. Bumex

Test Question #2 The major complication in treatment of chronic hyponatremia can be avoided by ? ● A. Using hypertonic saline (3%) ● B. Correct the Na by 12 meq/L in the first 24 hours ● C. Water restricting the patient ● D. Correct the Na by less than 8 meq/L in the first 24 hour

Answer to Question #1 ● B. Correct the Na by 12 meq/L in the first 24 hours

Answer to Question #2 ● D. Correct the Na by less than 8 meq/L in the first 24 hour
- Slides: 55