Going Paperless Donald T Stewart MD Don SPine




 – You have to pay employees to find them –")

























- Slides: 36
Going Paperless © Donald T. Stewart, MD Don. S@Pine. Lake. Med. com PPUG 2006
Going Paperless. . . • Can be a very painful process • May be the part of implementing the EMR that is the hardest for you • Takes away the security of the tool you have used for years – the paper chart • May never be totally successful: – Less Paper, Paper Light, vs Paperless
Why Go Paperless?
Why Go Paperless? • The answers are the same as the answers to the question: “Why get an EMR? ” – Paper charts are costly – Paper charts are hard to keep track of – Paper charts are impossible to get reports from – Paper charts take up space – Paper charts are rarely up to date
Why Go Paperless? (cont) – You have to pay employees to find them – You have to pay employees to put them away – You have to pay employees to copy them – You have to pay to archive them – You have to pay to get them out of archives – They mess up your office – They make you look backwards and incompetent
Why Go Paperless if you Have an EMR? – Double expense of having two systems – Data in chart and EMR rarely in sync – You get basically none of the benefits of having an EMR, but you still have the expenses – You still look backwards and incompetent
So, How do you go Paperless? • Decide what you want in the EMR: – – – – Major Problem List Medication List Allergies Past Medical History Social History Family History Habits – – – – – Lab Consults EKG Radiology Spirometry Procedures Hospital Reports Health Maintenance End of life documents Correspondence
Develop a Plan • for extracting the above data from the paper chart and getting it into the electronic chart – – Nurse/MA Responsibilities Physician Responsibilities “College Student” responsibilities Decide what is to be done and by whom before the provider sees the patient – Decide how you will archive the chart – It is important to make the chart disappear as soon as you get the data you want out. • Once a chart has been extracted and entered, no new data goes into it.
Lab Interface • This is the source of most of your Paper. Do it first. Start several months before going live. See if you can get your old data loaded. • Do not try to operate by scanning labs into the system, or by manually entering them.
Faxes • Get a Fax Server – Zeta. Fax, Rite. Fax, even Win. Fax, or MS Server 2003 • Use it • Two Fax lines – Prescription requests – Medical records
Train Your Consultants • Minimum is Fax all notes, no paper notes allowed – Good for consultant, because it will save them money • Even better is to get them to send you text files via email – Encrypt via Win. Zip – give consultant a password -These can be entered into chart via text, so you don’t have to plink
Train Consultants We let them know that since we have gone to an EMR, we are not able to accept letters any more, so we will only be referring to consultants who fax or email notes to us. Send them a reminder if they forget Three strikes and they are out.
Text Data Loader • A program that allows you to load an ascii or RTF text file into Practice Partner, which automatically goes to the correct place in the data base. This is part of Practice Partner • You can make a template in Microsoft Word or other word processor that can write ascii or RTF files, and have a college student extract the data from the charts into a file, which is loaded • Search Help under “text data loader” and “dot codes”
What Do You Enter with TDL? • • Past Medical History Social History Family History Major Problem List Medication List Allergies Health Maintenance ? Labs
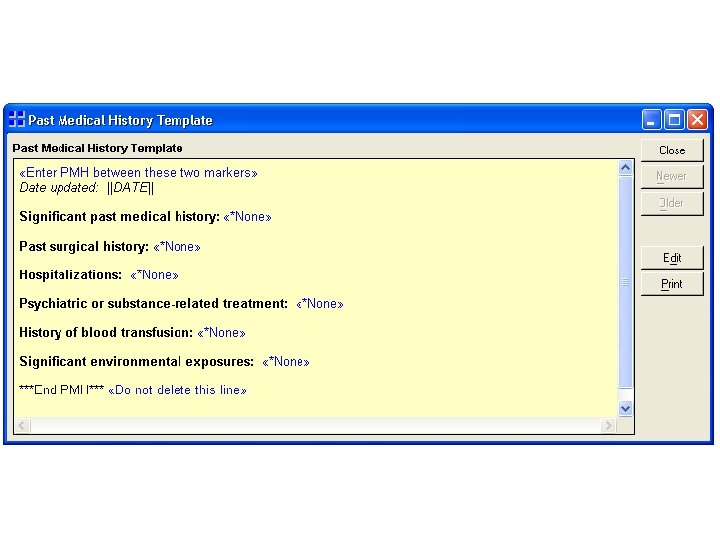
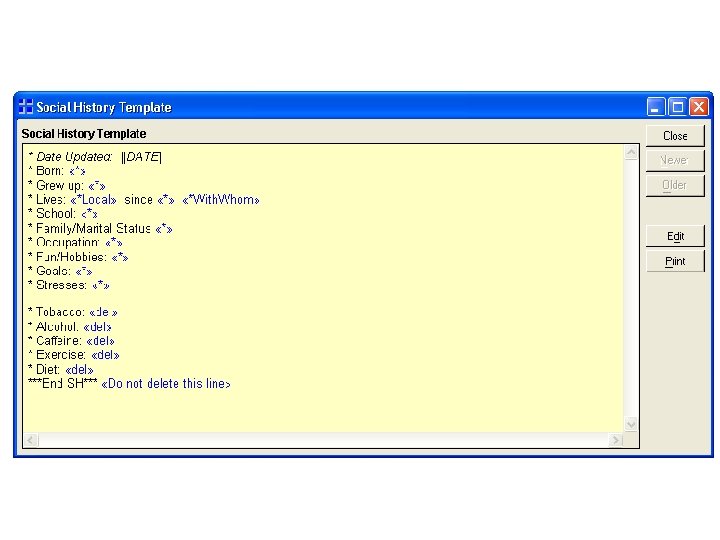
History Section Templates • Past Medical History • Family History • Social History • How you set these up takes special consideration, since this is a place where you can store important data to be imported into your notes
Past Medical History • Surgeries: Approximate Date, perhaps the location, perhaps who the surgeon was, complications • Medical Hospitalizations: Date, location, outcome, who the physicians were, significant procedures or tests done • Psychiatric or Substance-related treatment • Transfusions • Significant past medical illnesses or conditions • Significant environmental exposures
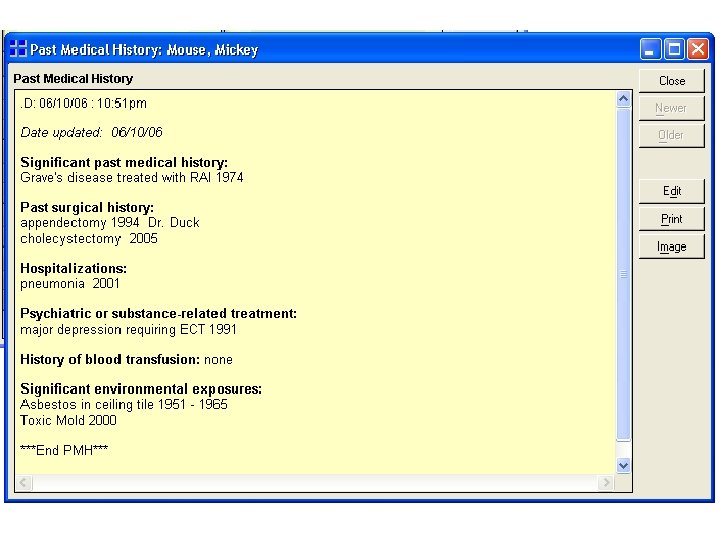
Past Medical History Uses • This is a great place to enter, for example, the details of a cardiac cath or bypass surgery that will be important in the patient’s future management. • It might be a great place to put a paragraph that updates the status of a patient with Crohn’s disease or RA.
Past Medical History Uses • The point is that this section can be pulled into your notes any time you want, can be as large as you want, and can be formatted however you like. • You should update it regularly and be sure to include the date of last update
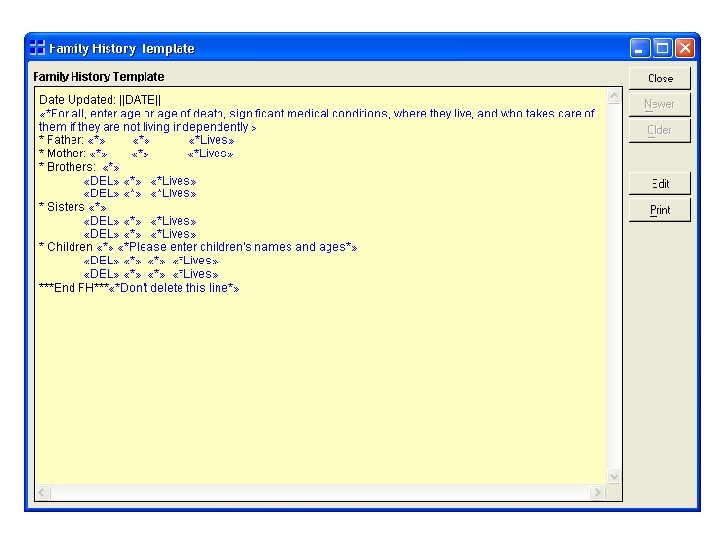
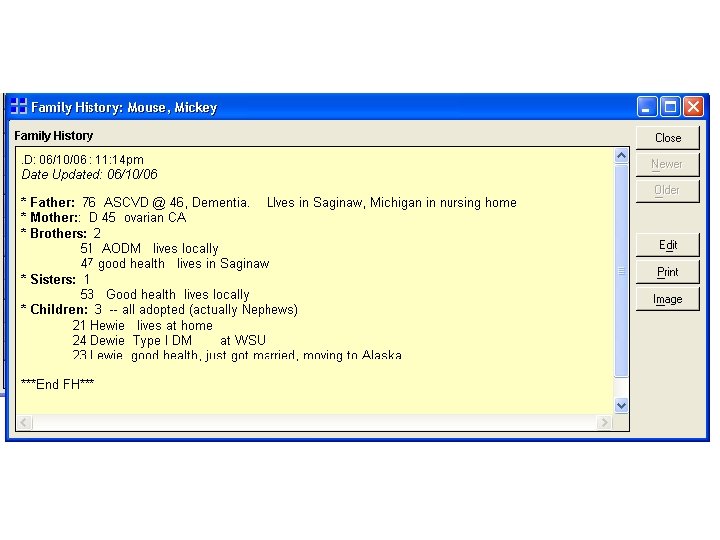
Family History • This can be a tremendous practice-builder and patient relationship builder for anyone in primary care. Lots of important social history included here. • Important to include: – – Date updated Approximate ages of family members or age at death Significant medical problems and health status Names of children (tremendously helpful in primary care), where they live, and what they do
Family History Additional Information • Status of parents, if elderly, quite important – where they live, who checks on them, what responsibilities the patient has for their care. • Number of grandchildren • Which siblings live close, and which ones are far away.
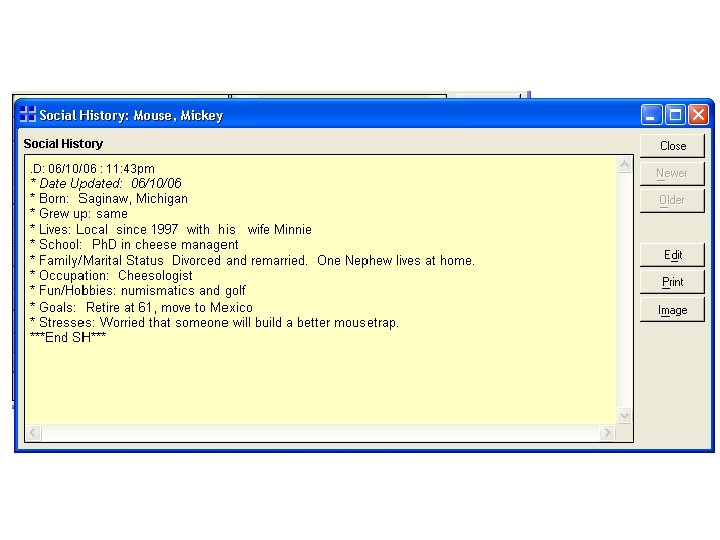
Social History: What makes the patient unique as a person • • • Where were they born? Where did they grow up? Where do they live, and for how long? Who do they live with? How far did they go in school? What is their family and marital status? What is their occupation? What do they do for fun? What are their goals? (retire, move, etc? ) What unusual stresses are they experiencing?
The Workflow • Provider takes the chart, puts sticky notes on pages to scan vs enter in PMH • Chart goes to College Student, who scans the pages and extracts the chart data onto file that will be loaded via TDL file. • The file is loaded (with multiple patients) at the end of the day • The chart goes to the back room, never to be pulled again except by request
Scanning • Some things are best scanned. Practice Partner Zoom and You Got P-Link, and Quick Doc Coder are products that can help link. I like Quick Doc Coder, by Bob Glorioso, MD, because it allows dot codes, and doesn’t require a PP License. (Google Spring Garden Family Practice for this. ) • The biggest issue is deciding what to scan and what not to scan.
What to Scan –Basic Considerations • If you do not own the original document, think twice about scanning it. • If you do own the original document, think thrice about scanning it. • Hospitals always have the original of records • Radiologists always have the old reports – (But you might not remember which radiology office did the tests) • Remember, you can always get the chart out of archives!
What to Scan • Consults – Just the important ones • EKG – Just the most recent, unless significant change • Hospital Records – Think seriously about what you bother to scan – Perhaps you just want to make an entry in PMH • Procedure/Surgical reports – Same as Hospital Records • Path reports – Think hard about what you want to scan vs enter in PMH
What to Scan • End of Life wishes – Living will – DNR forms • Ongoing problems related to MVA, third party injury claims, things you know you will want quick access to. • HIPPA Stuff – permission to share records with people
Workflow Before Going Paperless • Lab interface 3 -6 months before • Scanner and fax-scanner 3 -6 months before • Decide what chart sections will be used for what information • Identify frequent flyers • Prepare your TDL template
Ideal Workflow – All of the data that goes in via the TDL should be loaded before the provider sees the patient for a visit. Charts pulled the day or week before, extracted by MA or Nurse and given to college student. – The provider then enters the visit that day in the EMR, flags pages to scan, then never sees the chart again.
Reality • May not be able to do all charts of patients seen on a given day, depending on resources. – In that case, chose the frequent flyers first. – Once a chart has had data entered by TDL, flag it with a pop-up note to remind that changes to PMH, SH, FH must always be updated if they are entered on a visit after the TDL is run
Getting it Done • Physician never touches chart more than three times after the “paperless” date– then the chart must be removed • Since it costs money to pull charts, fine patient $10. 00 for each chart they request after the “third touch” • Bonuses to staff members—get everyone involved • College students are great!