GDM why it is important Professor Fidelma Dunne

 • GDM detects an at-risk pregnancy for mother. • GDM detects")








 to")










 • Insulin (30%) • Metformin (NICE)")









 P")

 and National")
. §Contrasts with prior studies in non-diabetic women")






, obesity and insulin resistance indices at follow-up (mean 2. 6")
 at follow-up (mean 2. 6 years) Prevalence (%) 100 54.")







- Slides: 67
GDM- why it is important. Professor Fidelma Dunne MD Ph. D FRCPI Consultant Endocrinologist Saolta University Hospital Group and National University of Ireland Galway Ireland.
Gestational Diabetes (GDM) • GDM detects an at-risk pregnancy for mother. • GDM detects an at risk pregnancy for the infant. • GDM is associated with increased future maternal life-time risk of Type 2 DM (50%). • GDM is associated with increased rates of obesity and prediabetes in adolescents and type 2 DM in adult life of the offspring. • DIABETES BEGETS DIABETES.
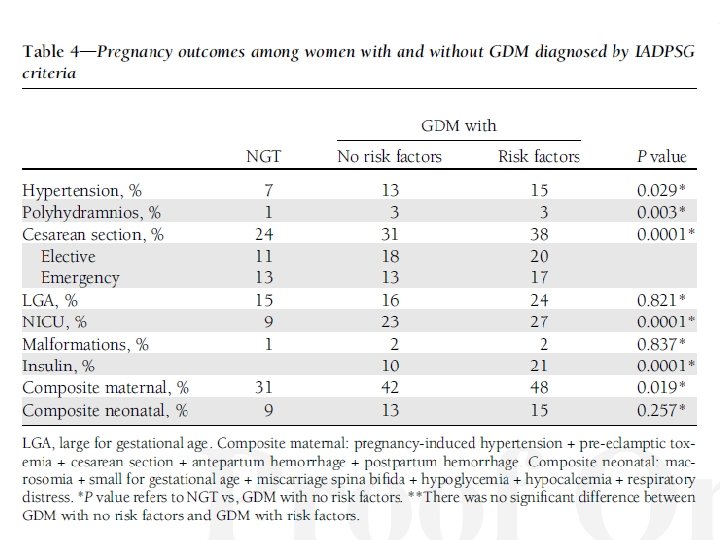
Why are we concerned about GDM? Mother Infant • PIH/PET • Macrosomia. • CS delivery • Hypoglycaemia/NNU • Future Diabetes • Obesity • Future Obesity • Met. S/CVS • Autism • Fatty Liver School Institute Name to go here
What global factors are contributing to increased GDM prevalence? • Prevalence of Type 2 DM; NHANES 4. 6% (18 -44 y). • Prevalence of pre-diabetes NHANES 26. 4% (18 -44 y). • Prevalence of Obesity, 20 -30% global estimates. • Rising maternal age for pregnancy. School Institute Name to go here
GDM- Can we make a difference? • Screening is easy and not costly. • Interventions are low key for the majority. • Treatments make a difference. • Future maternal Type 2 DM can be prevented. • Future maternal CVS risk can be addressed. • Family health can influence offspring health. School Institute Name to go here
Macrosomia
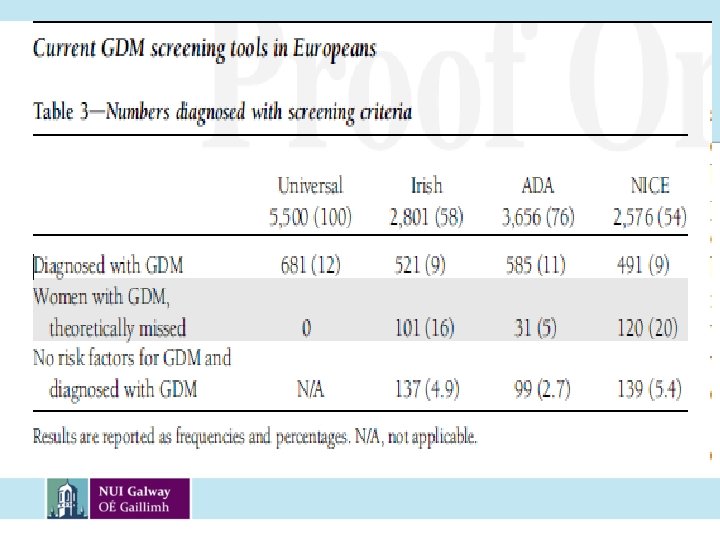
Who should we screen? How should we screen?
Who? • Universal • Selective School Institute Name to go here
How? • IADPSG/ WHO 2014 ---Perinatal outcomes • Carpenter & Coustan--- Future Diabetes Risk • NICE 2015 --- Cost School Institute Name to go here
Socio-Economic Status 1. Womens’ addresses were ‘geocoded’. Geocoding = Assigning geographic coordinates (longitude-latitude) to each address.
Distance from test hospital • For every 10 km required to travel, the probability of attending for screening is reduced by 2% • e. g. If you live 50 km away from hospital, you are 10% less likely to attend • If you like 100 km away you are 20% less likely to attend.
Deprivation Score • Correlation study: Relative to Deprivation score 1, ie ‘wealthiest’; Score 2: 2. 3% less likely to attend p=0. 138 Score 3: 4. 3% less likely to attend p=0. 008 Score 4: 7. 6% less likely to attend p=0. 0001 Score 5: 14. 5% less likely to attend p=0. 0001
School Institute Name to go here
Results: Primary v Secondary uptake rates • Secondary care group significantly more likely to attend at their randomised location (p < 0. 001) School of Medicine National University of Ireland, Galway
Preventing GDM School Institute Name to go here
4 individual risk factors School Institute Name to go here
Combining risk factors School Institute Name to go here
School Institute Name to go here
Exercise pre-pregnancy School Institute Name to go here
Exercise in early pregnancy School Institute Name to go here
Treatment of GDM? • MNT and Exercise (70%) • Insulin (30%) • Metformin (NICE) • Glibenclamide (ACOG) School Institute Name to go here
Is treatment beneficial? School Institute Name to go here
Shoulder Dystocia School Institute Name to go here
Macrosomia School Institute Name to go here
Preeclampsia School Institute Name to go here
What dietary intervention works? School Institute Name to go here
School Institute Name to go here
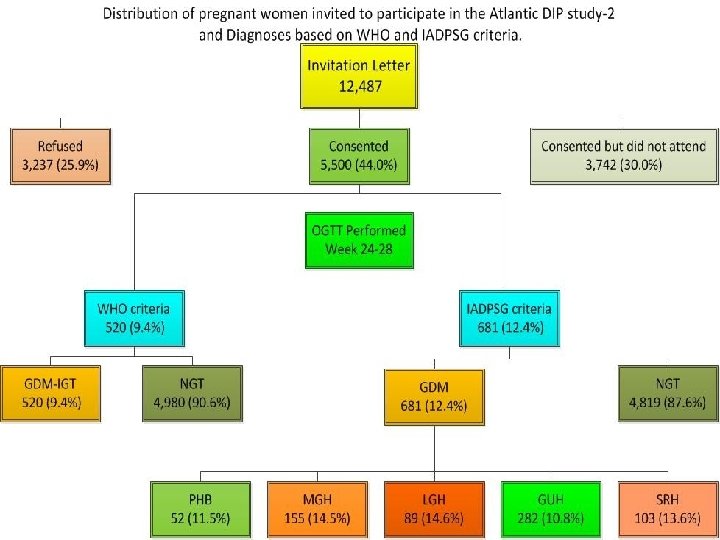
Diet and Exercise interventions in GDMdoes it work? The Atlantic DIP dataset was utilized: N = 567 women with GDM. (D+E) N = 2499 with NGT.
Differences in Characteristics GDM N = 567 NGT N = 2499 P value Age (mean =/-sd) 33. 4 (4. 9) 31. 5(5. 2) <0. 01 BMI (mean+/-sd) 30. 5 (6. 1) 26. 7 (4. 8) <0. 01 BMI>30 N (%) 279 (49%) 522 (21%) <0. 01 SBP (mean+/-sd) 119. 7 (13. 3) 116. 3 (17. 1) <0. 01 School Institute Name to go here
Differences in infant size GDM N =567 NGT N = 2499 P value LGA (>90 th C) BMI <25 BMI 25 -30 BMI>30 9. 4% 10. 4% 15. 1% 12. 2% 16. 0% 21. 8% 0. 4 0. 06 0. 02 Macrosomia (> 4 kg) BMI <25 BMI 25 -30 BMI>30 7. 5% 11. 0% 17. 6% 16. 5% 21. 8% 27. 0% 0. 02 0. 01 School Institute Name to go here
Composite Poor Neonatal Outcome • OR 0. 79 (CI 0. 64 -0. 98) P 0. 03 • 21% less likely to have an adverse outcome School Institute Name to go here
Gestational weight gain in GDM? • Is it important? School Institute Name to go here
Institute of Medicine Guidelines for Gestational Weight Gain Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines; Rasmussen KM YA, editors: Weight Gain During Pregnancy: Reexamining the Guidelines. 2009.
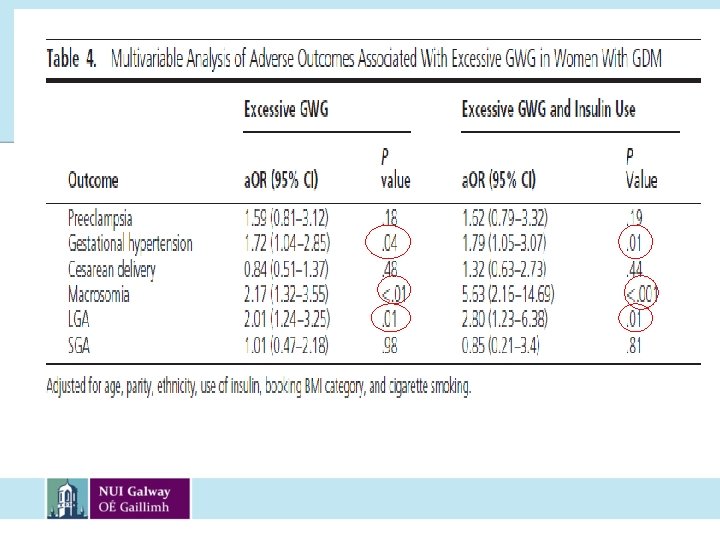
§ 57% women gained excessive weight (n=307). §Contrasts with prior studies in non-diabetic women (33%). 1 1. Nohr et al. Am J Clin Nutr, 2008
Glucophage ? • Used in South Africa in Type 2 DM since 1970. Perinatal mortality similar. • Used extensively with PCOS with no adverse outcomes (Tang 2010). • 3 systematic reviews and meta analysis (Gutzin 2003; Gilbert 2006; Juan Gui 2013; favour metformin re GWG, LGA, PIH, PET. • Less macrosomia in N/OW women (Ljas 2011). School Institute Name to go here
School Institute Name to go here
School Institute Name to go here
What are the health risks post GDM? School Institute Name to go here
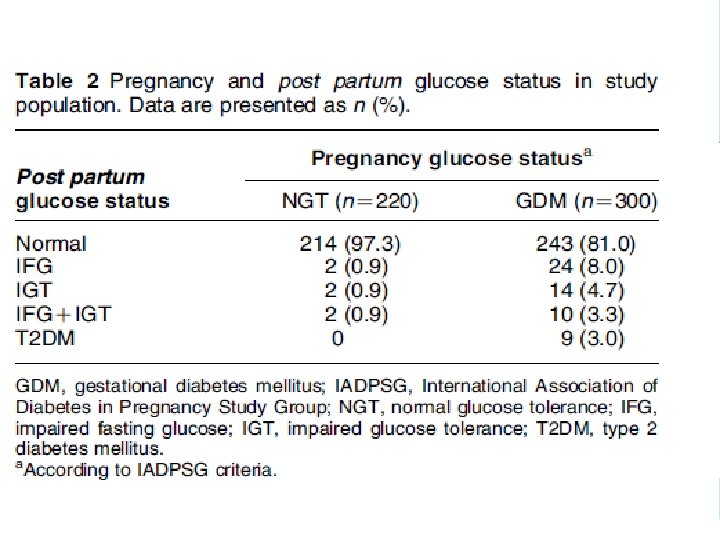
Abnormal glucose tolerance status at follow-up Glucose tolerance Previous GDM Previous NGT p value for status (n=270) (n= 388) difference IFG 12. 2% 1. 8% IGT 5. 9% 1. 5% IFG/IGT 5. 6% 0. 3% DM 2. 2% 0% Total 25. 9% 3. 6% <0. 001
Comparison of Hb. A 1 c and FPG to identify abnormal glucose post partum Criteria Sensitivity Specificity PPV NPV (95% CI) not requiring OGTT N(%) Hb. A 1 c 5. 7% FPG 5. 6 mmol/l Hb. A 1 c 5. 7% and FPG 5. 6 mmol/L 45 84 39 87 206 (32, 59) (78, 88) (27, 52) (82, 91) (78) 80 100 96 224 (66, 89) (98, 100) (91, 100) (92, 98) (85) 90 84 56 97 184 (78, 96) (78, 88) (45, 66) (94, 99) (70)
Metabolic syndrome (Met. S), obesity and insulin resistance indices at follow-up (mean 2. 6 years)
Metabolic syndrome components (ATP-III) at follow-up (mean 2. 6 years) Prevalence (%) 100 54. 7 50 GDM by IADPSG criteria 38. 9 NGT by IADPSG criteria 32. 5 31. 2 20. 4 15. 6 15. 1 14. 8 6. 1 1. 9 0 Waist circumference BP HDL Triglycerides Fasting glucose
Feig D. PLOS medicine 2013
Can we prevent Type 2 DM? School Institute Name to go here
Prevention Type 2 following GDM DPP Aroda VR. JCEM 04/2015 • DPP 3 year data; ILS reduced by 53%, metformin by 50% • DPP 10 year data; ILS reduced by 35%, metformin by 40% • Both ILS and metformin (850 mg BD) are effective in reducing progression to Diabetes School Institute Name to go here
Preventing Type 2 DM after GDM Bao W. Diabetologia 03/2015 N =1695 • Over 18 year F/U period • Each 5 kg increase in weight after index GDM pregnancy associated with 27% higher risk of T 2 DM. • Postpartum weight management essential School Institute Name to go here
School Institute Name to go here
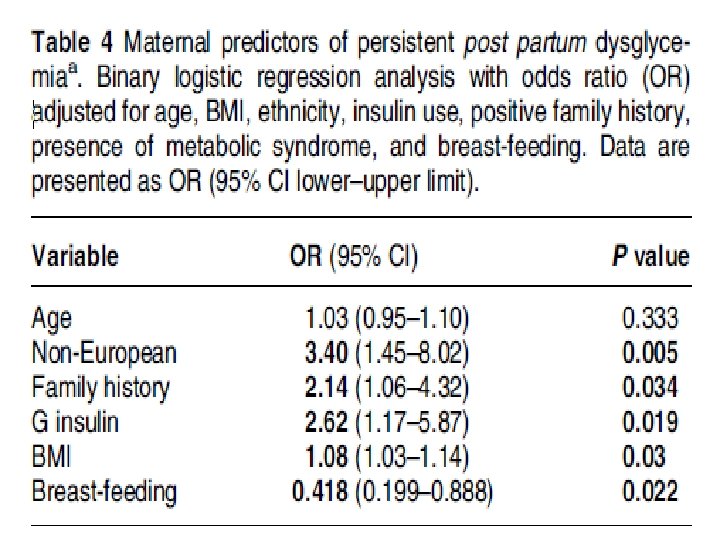
Summary • GDM is common. • Dietary intervention works. • Breast feeding should be encouraged. • Diabetes post GDM is a public health concern but can be prevented. • Metabolic syndrome and future CVS risk post GDM is a public health concern and requires F/U. • A strong screening programme is essential. • Integrated care is required. School Institute Name to go here