Controversies in Diagnosis of GDM H Delshad MD













 ►Founded in 1998 ►Purpose : facilitate")

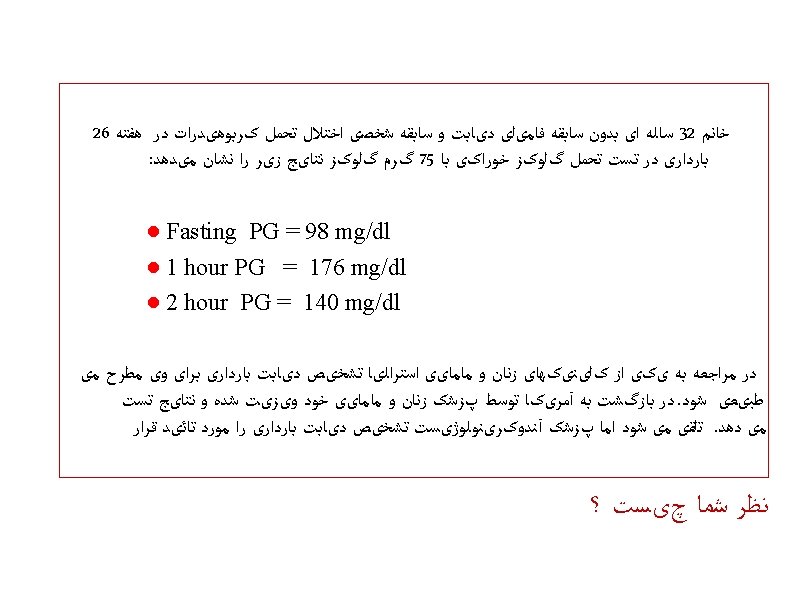
 : One step approach 75 -g")

 : Two step approach 1 - GCT : 50")


.")



 Postdoctoral Fellowship: Washington University, Biochemistry (1966) Residency: Michael")

- Slides: 29
Controversies in Diagnosis of GDM H. Delshad MD Endocrinologist
Controversies in Diagnosis of GDM • GDM & Controversy are old friends. • Lack of consensus for the diagnosis of GDM has been a problem ever since the existence of GDM was recognized. Who should be screened? When should be screened? How should be screened? What should be the diagnostic criteria? • A critical question is whether treatment of GDM improves outcomes.
Evolution of Diagnostic Criteria • • 1920 : Macrosomia with DM , Neonatal pancreatic islet hyperplasia 1924: Diabetic Gycosuria 1939 : Glycosuria and LGA 1945 : LGA and later DM 1952 : Maternal Hyperglycemia and Fetal Hyperinsulinemia, neonatal hypogly. 1957 : Elsie Carrington , used the term of Gestational Diabetes. 1961 : O, Sullivan study helped cement the link of GDM with later maternal DM n= 7061 high risk OGTT Family Hx. , Previous baby > 4 kg, 0. 86 % had DM Poor obstetric Hx. , BS ≥ 130 mg/dl on GCT 5 years later 28. 5% of 137 studied had DM
Evolution of Diagnostic Criteria • 1964: O, Sullivan & Mahan established criteria for the OGTT in pregnancy n= 752 100 -g, 3 -h OGTT 8 -years follow-up Mean and SD were derived for each of 4 whole blood glucose ( Fasting , 1 , 2 , 3 h) An increasing likelihood of subsequent DM Mean+1 SD Mean+2 SD Mean+3 SD 7% 16% 40% Theoretic diagnostic criteria were calculated based upon 2 abnormal values defined as : Mean plus 1 , 2 or 3 SD Two abnormal values (mean+2 SD) accepted thresholds for diagnosis of GDM Fasting 1 -hour 2 -hour 3 -hour 90 165 145 135
Evolution of Diagnostic Criteria • 1979 : NDDG modified these number for venous plasma *GDM : 2 or more ≥ Fasting 1 -hour 2 -hour 3 -hour 105 190 165 145 (The original O, Sullivan & Mahan criteria were increased by 14%) Diabetes 1979; 28: 1039 -1057
Evolution of Diagnostic Criteria 1982 : Carpenter & Coustan provided their own modification of the numbers Somogyi-Nelson Vs. Glucose oxidase & Hexokinase Whole blood Vs. Plasma glucose Coustan ( -5 mg/dl + 14%) Carpenter *GDM : 2 or more ≥ Fasting 1 -hour 2 -hour 3 -hour 95 180 155 140 ADA & ACOG endorsed Carpenter and Coustan criteria Am J Obstet Gynecol 1982; 144: 768 -773
Evolution of Diagnostic Criteria • 1999 : WHO stated that diagnostic procedures and criteria for GDM should be the same as non- pregnant adult. 75 -g , OGTT: *GDM : 1 or more ≥ Fasting 1 -hour 2 -hour 3 -hour 126 - 140 -
Evolution of Diagnostic Criteria • 2006 : A review showed at least 9 different criteria for diagnosis of GDM among 12 set of recommendations across the world. • All the diagnostic criteria were based on the maternal risk of developing DM postpartum and not on pregnancy and perinatal risk. • Clinical outcomes are the best way to define diagnostic thresholds. • With this background of confusion the large HAPO study set out to confirm: ● The relationship between glucose and specific outcomes ● Facilitate identification of diagnostic criteria that could be applied worldwide.
Boyd E. Metzger The members of the HAPO Study Cooperative Research Group were as follows: North American Field Centers — Kaiser Foundation Hospital, Bellflower, CA: M. Contreras, D. A. Sacks, W. Watson (deceased); Prentice Women’s Hospital of Northwestern Memorial Hospital–Northwestern University Feinberg School of Medicine, Chicago: S. L. Dooley, M. Foderaro, C. Niznik; Metro. Health Medical Center–Case Western Reserve University, Cleveland: J. Bjaloncik, P. M. Catalano, L. Dierker, S. Fox, L. Gullion, C. Johnson, C. A. Lindsay, H. Makovos, F. Saker; Women and Infants’Hospital of Rhode Island–Brown University Medical School, Providence: M. W. Carpenter, J. Hunt, M. H. Somers; Sunnybrook and Women’s College Health Sciences Centre–University of Toronto, Toronto: K. S. Amankwah, P. C. Chan, B. Gherson, E. Herer, B. Kapur, A. Kenshole, G. Lawrence, K. Matheson, L. Mayes, K. Mc. Lean, H. Owen; European–Caribbean Field Centers — Queen Elizabeth Hospital–School of Clinical Medicine and Research, University of the West Indies, Barbados: C. Cave, G. Fenty, E. Gibson, A. Hennis, G. Mc. Intyre, Y. E. Rotchell, C. Spooner, H. A. R. Thomas; Royal Jubilee Maternity Hospital, Belfast, Northern Ireland: J. Gluck, D. R. Hadden, H. Halliday, J. Irwin, O. Kearney, J. Mc. Anee, D. R. Mc. Cance, M. Mousavi, A. I. Traub; St. Mary’s Hospital–Manchester University, Manchester, United Kingdom: J. K. Cruickshank, N. Derbyshire, J. Dry, A. C. Holt, F. Khan, C. Lambert, M. Maresh, F. Prichard, C. Townson; University Hospital–University Medical Center Utrecht, the Netherlands: T. W. van Haeften, A. M. R. van de Hengel, G. H. A. Visser, A. Zwart; Middle Eastern–Asian Field Centers — Rajavithi Hospital, Bangkok, Thailand: U. Chaovarindr, U. Chotigeat, C. Deerochanawong, I. Panyasiri, P. Sanguanpong; Soroka Medical Center–Ben-Gurion University, Beersheba, Israel: D. Amichay, A. Golan, K. Marks, M. Mazor, J. Ronen, A. Wiznitzer; Helen Schneider Hospital for Women, Rabin Medical Center–Sackler Faculty of Medicine, Tel-Aviv University, Petah-Tiqva, Israel: R. Chen, D. Harel, N. Hoter, N. Melamed, J. Pardo, M. Witshner, Y. Yogev; Australasian Field Centers — Mater Misericordiae Mothers’ Hospital–University of Queensland, Brisbane, Australia: F. Bowling, D. Cowley, P. Devenish-Meares, H. G. Liley, A. Mc. Ardle, H. D. Mc. Intyre, B. Morrison, A. Peacock, A. Tremellen, D. Tudehope; Prince of Wales Hospital–Chinese University of Hong Kong, Hong Kong: K. Y. Chan, N. Y. Chan, L. W. Ip, S. L. Kong, Y. L. Lee, C. Y. Li, K. F. Ng, P. C. Ng, M. S. Rogers, K. W. Wong; John Hunter Hospital, Newcastle, Australia: M. Edgar, W. Giles, A. Gill, R. Glover, J. Lowe, F. Mackenzie, K. Siech, J. Verma, A. Wright; KK Women’s and Children’s Hospital, Singapore City, Singapore: Y. H. Cao, J. J. Chee, A. Koh, E. Tan, V. J. Rajadurai, H. Y. Wee ,
HAPO Study n= 23, 316 15 centers in 9 different countries 2 -h 75 -g OGTT, at 24 -32 Followed prospectively for : ● Primary outcomes ● Secondary outcomes
HAPO study showed continuous associations between maternal PG and adverse pregnancy outcomes Odds ratios were for an increase in the glucose level of 1 SD (6. 9 mg per deciliter for the fasting plasma glucose level, 30. 9 mg per deciliter for the 1 -hr plasma glucose level, and 23. 5 mg per deciliter for the 2 -hr plasma glucose level).
Each of the 3 values in the OGTT had independent contribution to adverse outcomes, but there were no obvious thresholds at which risks increased Frequency of Primary Outcomes across the Glucose Categories
(International Association of Diabetes and Pregnancy Study Groups) ►Founded in 1998 ►Purpose : facilitate collaboration between the various national groups interested in GD ►It convened a meeting in Pasadena in 2008 and used HAPO data as the basis for a new GDM diagnostic thresholds. ►The diagnostic thresholds were based on glucose levels associated with an Odds ratio of 1. 75 for primary outcomes. The thresholds were : Fasting 1 - hour 2 - hour 92 180 153
Clinical Recommendations • All pregnant women should be screened for GDM • Screening is generally performed at 24 -28 weeks of gestation • Early pregnancy screening for undiagnosed T 2 DM is suggested in women with: ○ Previous medical Hx. of GDM ○ Known Impaired Glucose Metabolism Measure of glycemia Threshold for diagnosis ○ Obesity ( BMI ≥≥ 126 30 kg/m ²) Fasting plasma glucose mg/dl Hb. A 1 c ≥ 6. 5% ( DCCT/UKPDS standard ) Random plasma glucose 200 mg/dl + confirmation (FBS or Hb. A 1 c) Fasting PG ≥ 92 mg/dl but a value < 126 mg/dl = GDM
Clinical Recommendations IADPSG , ADA …. . (2010) : One step approach 75 -g glucose, 2 -hour OGTT , at 24 -28 weeks, Fasting 1 -h PG 2 -h PG 92 180 153 * GDM= 1 or more ≥ Diabetes Care 2010; 33: 676 -682
Clinical Recommendations ACOG : Two step approach 1 - GCT : 50 -g glucose, at 24 -28 weeks, any time of day • Plasma glucose 1 -hour later : ● <140 mg/dl = normal ● 140 – 199 mg/dl = OGTT ● ≥ 200 mg/dl = GDM 2 - 100 -g, 3 -hour diagnostic OGTT: Fasting 1 -h PG 2 - h PG 3 -h PG 95 180 155 140 * GDM= 2 or more ≥ Obstetric & Gynecology 2013; 137: 406 -416
Clinical Recommendations NIH ( 2013) : Two step approach 1 - GCT : 50 -g glucose, at 24 -28 weeks, any time of day • Plasma glucose 1 -hour later : ● <140 mg/dl = normal ● 140 – 199 mg/dl = OGTT ● ≥ 200 mg/dl = GDM 2 - 75 -g, 2 -hour diagnostic OGTT: Fasting 1 –h PG 2 – h PG 95 162 NIH Consens State Sci Statements. 2013 Mar 6; 29(1): 1 -31 * GDM= 1 or more ≥
Criticism of the IADPSG Criteria • IADPSG published recommendations for diagnosis and classification of hyperglycemia in 2010. • Subsequently, some commentaries and debate challenged this recommendation. • Frequency • Outcomes • Odds ratios • Reproducibility • Role of obesity • Cost benefits of treatment Boyd E. Metzger and IADPSG Consensus Panel Writing group: The diagnosis of gestational diabetes mellitus: new paradigms or status quo? The Journal of Maternal-Fetal and Neonatal Medicine, 2012; 25(12): 2564 -2569
Fig 1 Flowchart of article selection in trial. Horvath K et al. BMJ 2010; 340: bmj. c 1395 © 2010 by British Medical Journal Publishing Group
Fig 2 Maternal outcomes in pool A (Der. Simonian and Laird random effects model). Horvath K et al. BMJ 2010; 340: bmj. c 1395 © 2010 by British Medical Journal Publishing Group
Fig 3 Neonatal outcomes in pool A (Der. Simonian and Laird random effects model, except for perinatal and neonatal morality and birth trauma, which use Peto fixed effects model). Horvath K et al. BMJ 2010; 340: bmj. c 1395 © 2010 by British Medical Journal Publishing Group
Fig 4 Maternal outcomes in pool B (Der. Simonian and Laird random effects model, except for shoulder dystocia, which uses Peto fixed effects model). Horvath K et al. BMJ 2010; 340: bmj. c 1395 © 2010 by British Medical Journal Publishing Group
Fig 5 Neonatal outcomes in pool B (Der. Simonian and Laird random effects model, except for perinatal and neonatal morality and birth trauma, which use Peto fixed effects model). Horvath K et al. BMJ 2010; 340: bmj. c 1395 © 2010 by British Medical Journal Publishing Group
MD: State University of Iowa (1959) Postdoctoral Fellowship: Washington University, Biochemistry (1966) Residency: Michael Reese Medical Center, Medicine (1963) Internship: Michael Reese Medical Center (1960) Board Certification: Internal Medicine
Charles J. Pedersen