Abnormal Uterine Bleeding H Delshad MD Endocrinologist Research
")
Abnormal Uterine Bleeding H. Delshad MD Endocrinologist Research Institute for Endocrine Sciences (SBUMS)

Causes of abnormal bleeding by age

Causes of abnormal bleeding by age Reproductive years Anovulation Pregnancy Cancer Polyps, Fibroids, Adenomyosis Infection Bleeding diathesis Endocrine dysfunctions Systemic disorders Medications

Anovulation • PCOS : common cause of abnormal bleeding in the adolescent with chronic anovulation • Obesity, menstrual irregularity, insulin resistance, and/or signs of hyperandrogenism (hirsutism, acne, clitoromegaly) • PCOS also should be considered in girls with prolonged menstrual irregularity and/or severe DUB, even in the absence of hirsutism or acne.

Bleeding diathesis • Menorrhagia that occurs at regular intervals or at the onset of menses is often related to a bleeding diathesis. • The prevalence of bleeding disorders among adolescents hospitalized for Menorrhagia ranges from 5 to 28 percent

Bleeding diathesis Consider the diagnosis of a bleeding diathesis in adolescents who present with: ● Extremely heavy first menses ● Bleeding requiring blood transfusion ● Refractory menorrhagia and concomitant anemia
 • Platelet dysfunction")
Bleeding diathesis • von Willebrand disease • Idiopathic thrombocytopenic purpura (ITP) • Platelet dysfunction • Thrombocytopenia secondary to malignancy or treatment for malignancy • Medications: anticoagulant or platelet inhibitors

Erik Adolf von Willebrand ● Menorrhagia
")
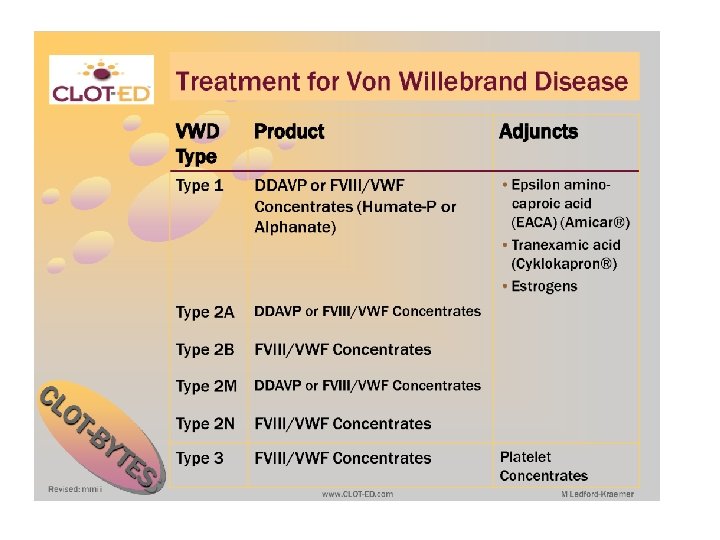
von Willebrand disease: Diag. • von Willebrand panel: ▪ Plasma von Willebrand factor (VWF) antigen ▪ Plasma VWF activity (ristocetin cofactor activity) ▪ Factor VIII activity • The von Willebrand panel: Should be obtained when the patient is not taking hormones, because exogenous estrogen may elevate VWF into the normal range
, Primary immune thrombocytopenic purpura Autoimmune thrombocytopenic purpura ●")
Bleeding diathesis Idiopathic thrombocytopenic purpura (ITP), Primary immune thrombocytopenic purpura Autoimmune thrombocytopenic purpura ● Thrombocytopenia with normal bone marrow and the absence of other causes. ● The acute form often follows an infection and has a spontaneous resolution within 2 months. ● Chronic ITP persists longer than 6 months without a specific cause.

Endocrine dysfunctions ● Cushing, s Syndrome ● Thyroid Dysfunction ● Hyperprolactinemia

Cushing, s Syndrome ● Women with Cushing, s syndrome may have unstable or no menstrual periods. ● Menstrual abnormalities correlate with increased serum cortisol and decreased serum estradiol concentrations, but not with serum androgen concentrations. ● The menstrual irregularities may be due to suppression of secretion of Gn. RH by hypercortisolemia.

Thyrotoxicosis • Hyperthyroidism occurring before puberty has been reported to delay sexual maturation and the onset of menses. • Amenorrhea was one of the earlier of the known clinical changes associated with hyperthyroidism, as reported by von Basedow in 1840. • A number of other changes in the menstrual cycle, including Oligomenorrhea, Hypomenorrhea, and Anovulation has been frequently reported.

Thyrotoxicosis • Benson and Dailey : 221 hyperthyroid patients 58% Oligomenorrhea or Amenorrhea 5% Polymenorrhea. • Gerasimos E. & Krassas : 214 thyrotoxic patients 24 Hypomenorrhea 15 Polymenorrhea 5 Oligomenorrhea 2 Hypermenorrhea None had amenorrhea. Menstrual disturbances are lower than has previously been described Nowadays, thyroid disturbances are diagnosed much earlier when the symptoms are still mild.

Thyrotoxicosis • Gerasimos E. & Krassas : smoking aggravates the development of menstrual disturbances in thyrotoxicosis. • 50% of the thyrotoxic patients with abnormal menstruation were smokers, compared with 19% of the thyrotoxic patients with normal periods. • Patients with menstrual disturbances had higher total T 4 levels and that the levels were higher in smokers with abnormal periods.

Thyrotoxicosis Causes of the menstrual disturbances: • Biochemical and hormonal abnormalities • Nutritional disturbances • Emotional disturbances Menstrual irregularities sometimes preceded identified thyroid dysfunction.

Thyrotoxicosis Hormonal changes: SHBG • Metabolic clearance rate of E 2 • Plasma estrogen x 2 -3 • Production rate of Testosterone and Androstenedione ● ● ● Mean LH in both the follicular and luteal phases Baseline FSH levels

Hypothyroidism Menstural disturbances : • Oligomenorrhea • Amenorrhea • Polymenorrhea • Menorrhagia (E 2 breakthrough bleeding secondary to anovulation ) • Defects in hemostasis: factors VII, VIII, IX, and XI, may also contribute to Polymenorrhea and Menorrhagia.
 had menstrual irregularities,")
Hypothyroidism • Scott and Mussey : 50 hypothyroid patients 28 (56%) had menstrual irregularities, mainly Metrorrhagia or Menorrhagia, alone or combined. • Joshi et al: 22 patients with hypothyroidism 15 (68. 2%) had menstrual irregularities in comparison with 6 (12. 2%) of 49 controls. 8 = Oligohypomenorrhea 2 = Amenorrhea 5 = Polymenorrhea and Menorrhagia.
 had irregular")
Hypothyroidism • Krassas GE, et al. 171 hypothyroid women 40 (23. 4%) had irregular cycles : ● 17 Oligomenorrhea, ● 6 Hypomenorrhea, ● 5 Amenorrhea, ● 12 Hypermenorrhea/menorrhagia. ● None had Polymenorrhea or Hypermenorrhea.

Hypothyroidism • Metabolic clearance of Androstenedione and Estrone • Peripheral aromatization • Binding activity of SHBG • Plasma concentrations of both testosterone and E 2 • Their unbound fractions

Hypothyroidism • Gonadotropin levels are usually normal. • Blunted or delayed LH response to Gn. RH has been reported in some female patients with hypothyroidism. • TRH increases the secretion of TSH and PRL.

Hyperprolactinemia • Usually results in Amenorrhea and Galactorrhea • Some affected women may develop anovulatory bleeding prior to amenorrhea.

33 -yr-old woman with prolactin 147 ng/ml on OCP until she was 28 yr old, She has tried for pregnancy since 2 years ago without success. She denied using any potential drug that could induce hyperprolactinemia. Her menstruation is regular without gallactorrhea. To restore her fertility, treatment for hyperprolactinemia was suggested. Do you agree with this suggestion? Sellar MRI depicting normal pituitary gland ; coronal views without (A) and with (B) gadolinium enhancement
- Slides: 29