Family Medicine Resident School Lecture 4517 Ashley Crum












 § Mechanism § FOOSH with forearm")





 § Mechanism § Young patients - high")
 § extra-articular § <5")























 § CT scan for displacement")

 or Intra-articular (75%) § Exam: § Diffuse tenderness § Ecchymosis §")







- Slides: 71
Family Medicine Resident School Lecture 4/5/17 Ashley Crum, MD Emergency Medicine/Sports Medicine Fellow
§ Identify common fractures in upper and lower extremities § Treatment § Urgent vs Non-urgent referal
§ Try to understand the mechanism of injury from the history § Always do a neurovascular exam before and after any manipulation § Do not push for ROM testing if you suspect a fracture until you have x-rays
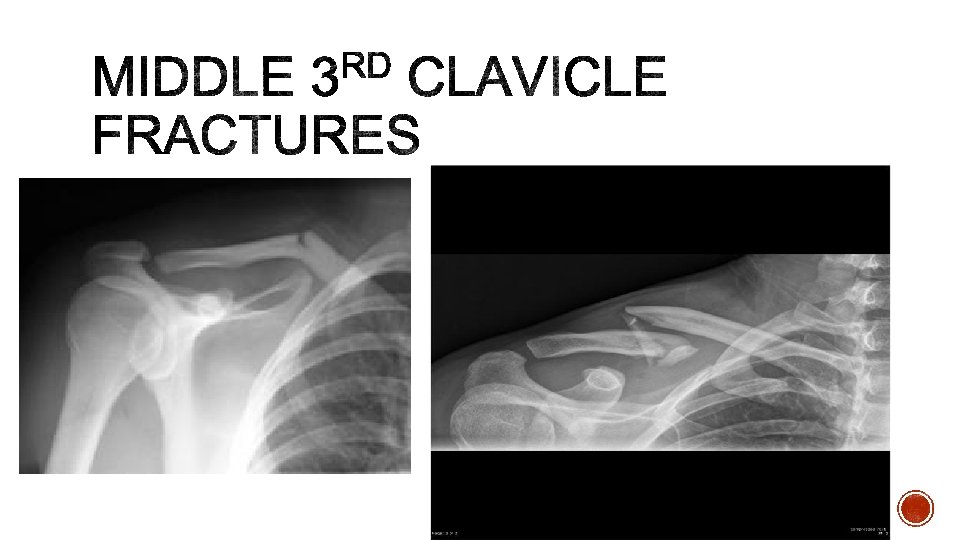
§ 4% of all fractures § Mechanism: § direct blow to lateral aspect of shoulder § fall on an outstretched arm or direct trauma § Exam: § Deformity present with decreased ROM § Imaging: § X-rays § CT (to better characterize fracture or vascular structures
§ Sling immobilization with gentle ROM exercises at 2 -4 weeks and strengthening at 6 - 10 weeks § Non-displaced middle third § Most pediatric § Stable lateral third § Operative § Open § Non-union symptomatic § Skin tenting § Vascular injury § Unstable fractures (posterior medial third, most lateral third § Ortho referral: Non-emergent for most
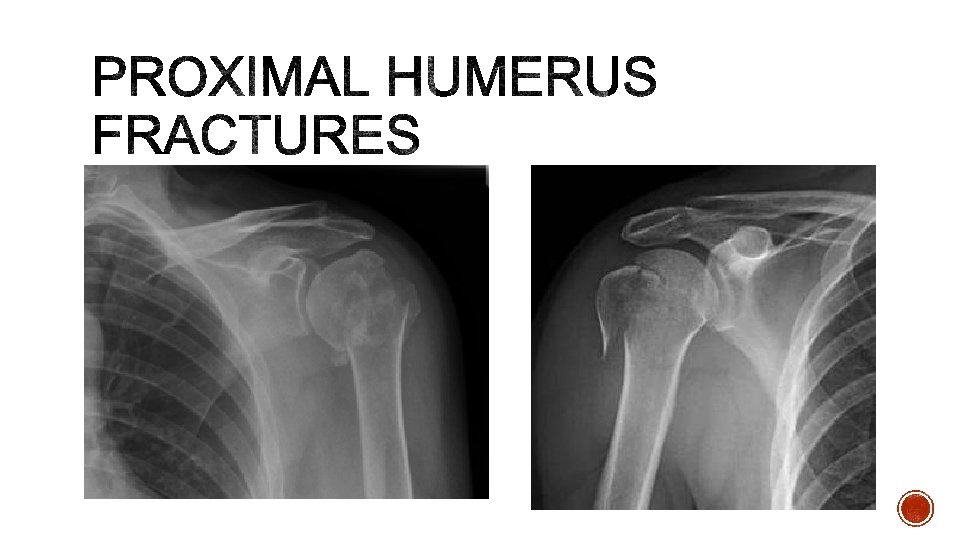
§ 4 -6% of all fractures § Mechanism: § Low energy falls in elderly/osteoporosis § High energy mechanism in young § Neurovascular injury more likely § Exam: § Decreased ROM § Pain over proximal humerus § Neurovascular § Imaging: § X-rays What is the most common nerve injury and why?
§ Sling immobilization followed by progressive rehab at 14 days § minimally displaced surgical neck fracture § greater tuberosity fracture displaced < 5 mm § Surgical management § Greater tuberosity fracture displaced >5 mm § Displaced surgical neck fractures § Compacted fractures with good bone quality § Ortho referral: § Urgent follow up (may call to review x-ray with) § Emergent if vascular compromise
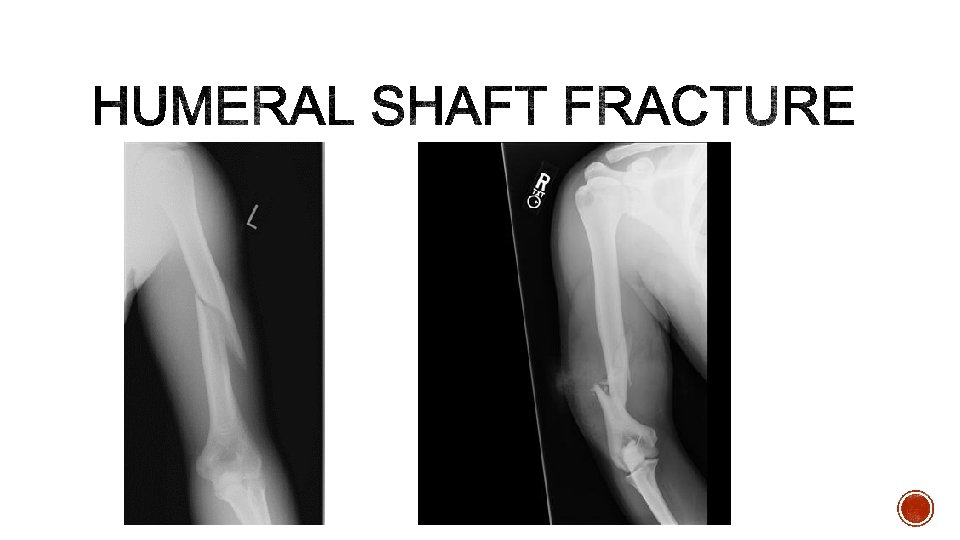
§ 3 -5% all fractures § Mechanism: § Same as proximal humerus § Exam: § Swelling, deformity § What nerve must be examined and how do you test it? § Imaging: § X-ray humerus and above and below
§ Coaptation splint followed by functional brace § Most fractures, depending on displacement § 2 -10% risk of non-union § Surgical § Open fracture § Vascular injury § Neurological injury § Ortho referral: non-urgent in most cases
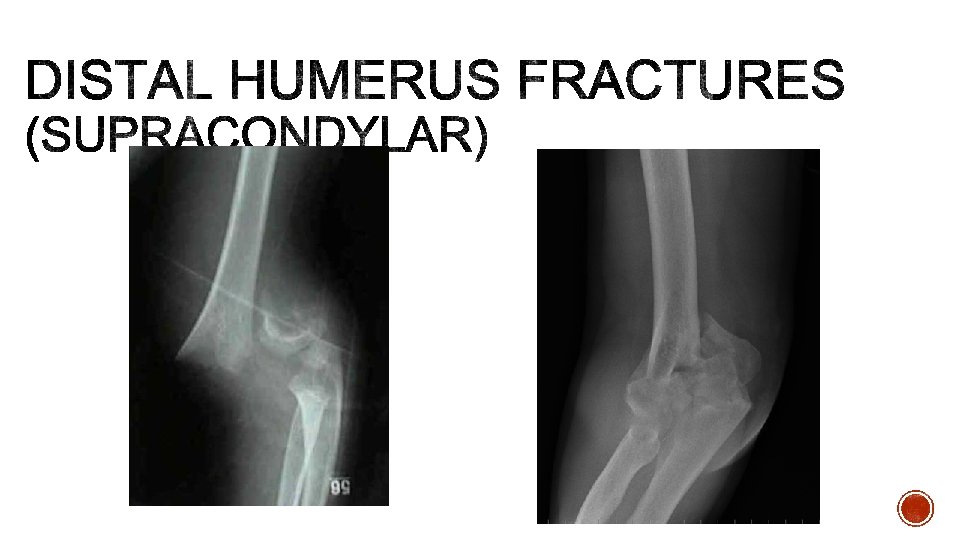
§ Extension type 95 -98%% § Flexion type <5% § Mechanism § Fall on outstretched hand § Exam § Won’t move elbow § Must check nerves, vascular (5 -17% compromised) § How do you check AIN function? § Imaging § X-rays (what is the sign of occult fracture? )
§ Gartland Classification § Long arm posterior splint then long arm casting with less than 90° of elbow flexion § Type 1 and some type 2 § Operative § Neuro/vascular compromise § Severe swelling § Floating elbow § Brachialis sign § Ortho referral: usually urgent or emergent
§ Lateral epicondyle fracture § Medial epicondyle fracture
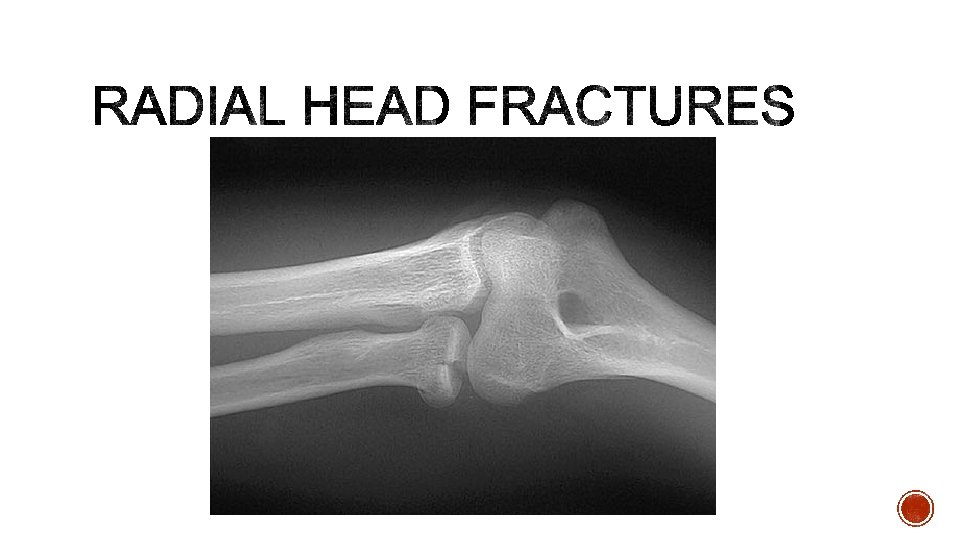
§ Most common elbow fractures (20% elbow injuries) § Mechanism § FOOSH with forearm pronated § Exam: § Tender along lateral aspect of elbow § Check all ROM § Ligament stability § What other joint should be examined? ? § Imaging: § X-rays What does this image demonstrate?
§ Short period of immobilization followed by early ROM § Isolated, minimally displaced, no mechanical blocks § Can get elbow stiffness with prolonged immobilization § Surgical § Mechanical block § Other injuries § Ortho Referral: close follow up for most
§ Comprised of a comminuted fracture of radial head +dislocation of the DRUJ +interosseous membrane disruption The DRUJ injury may be missed leading to permanent wrist pain and stiffness.
§ Definition § distal 1/3 radius shaft fx AND § associated distal radioulnar joint (DRUJ) injury § Mechanism § direct wrist trauma dorsolateral aspect § fall onto outstretched hand with forearm in pronation § Exam § Tenderness at fracture site § Check pronation/supination for instability § Stress to DRUJ causes wrist or midline pain § Imaging § X-ray forearm, elbow, wrist
§ Is Operative § Better outcomes with sooner rather than later surgery § Ortho referral § Would call for recommendations at time of presentation
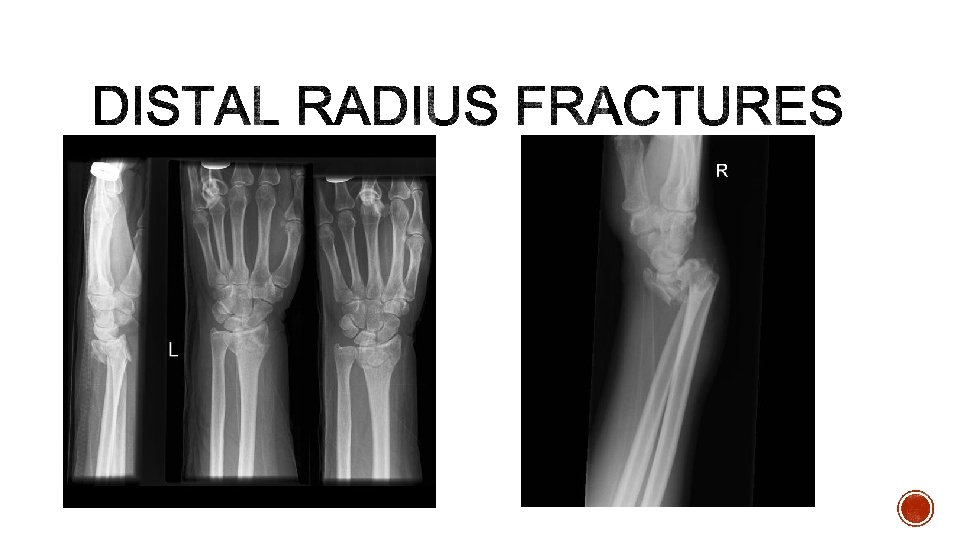
§ Most common orthopaedic injury (50% intraarticular) § Mechanism § Young patients - high energy § older patients - low energy / falls § Colles: FOOSH with a pronated forearm in dorsiflexion § Smith: backward fall on the palm of an outstreched hand causing pronation of upper extremity while the hand is fixed to the ground § Exam § Deformity, neurovascular § Imaging § X-rays
§ Closed reduction and cast immobilization (finger trap is helpful) § extra-articular § <5 mm radial shortening § dorsal angulation <5° or within 20° of contralateral distal radius § Surgical § radiographic findings indicating instability § Ortho Referral: need close follow up after reduction and splint. May need them to help you with a reduction
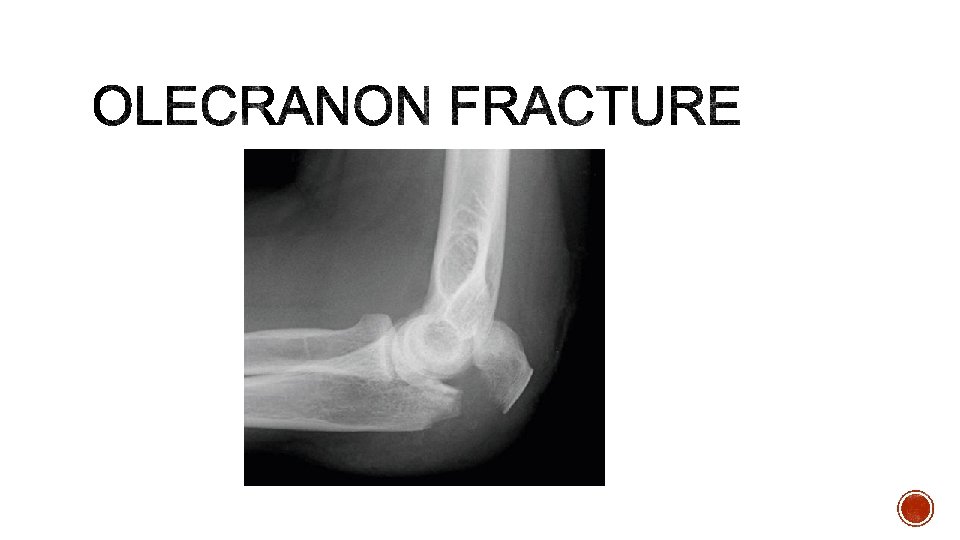
§ Bimodal distribution § Mechanism § direct blow: comminuted fracture § fall onto outstretched upper extremity § transverse or oblique fracture § Exam § Check extensor mechanism § Deformity of posterior elbow § Imaging § X-ray (need a true lateral)
§ Immobilization with early ROM at one week § Non-displaced fractures or low demand elderly individual § Splint in 45 -90% § Surgical § Complex fractures § Ortho referral: close outpatient follow up (unless very complex, problems with extensor mechanism)
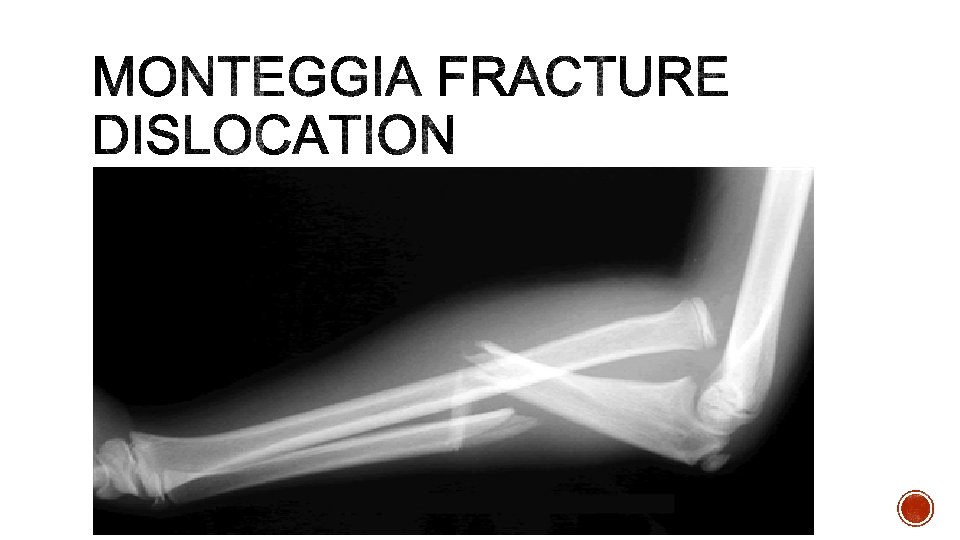
§ Proximal 1/3 ulnar fracture with associated radial head dislocation/instability § More common in children (4 -10 years old) § Mechanism: FOOSH § Exam § May not be obvious, check skin integrity § ROM loss with dislocation § What nerve could be affected? § Imaging § X-ray elbow, forearm, wrist
§ Adult: usually operative § Pediatric: usually closed reduction, immobilization § Can have PIN neuropathy which resolves over time § Ortho Referral: § If possible check with ortho prior to reduction
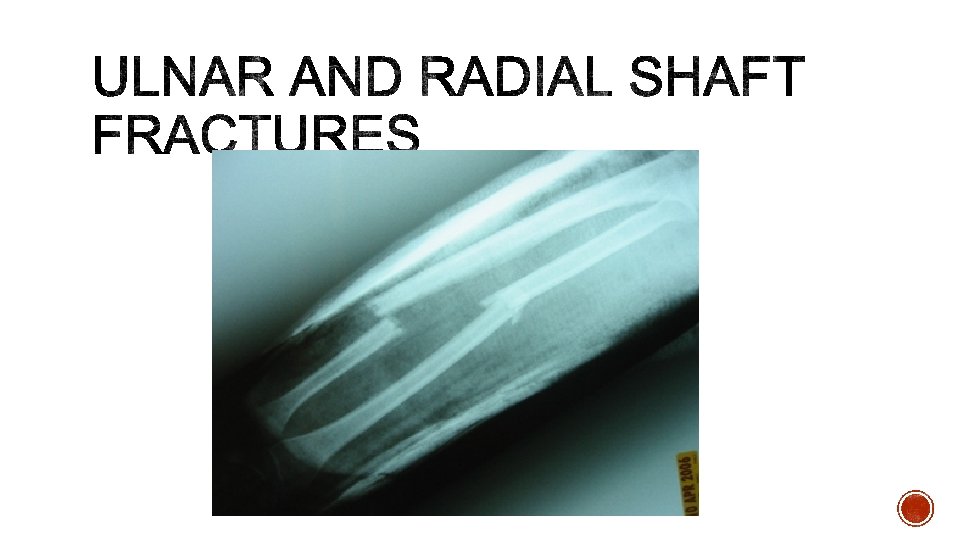
§ Mechanism § Direct trauma, athletic injury, fall from height § Exam § Large deformity § May need to check compartments § Imaging § X-rays § Treatment: § functional fx brace with good interosseous mold for non-displaced ulnar fractures § Surgical: radial fractures, displaced ulnar fractures § Ortho Referral: Urgent if surgical or outpatient if non-displaced
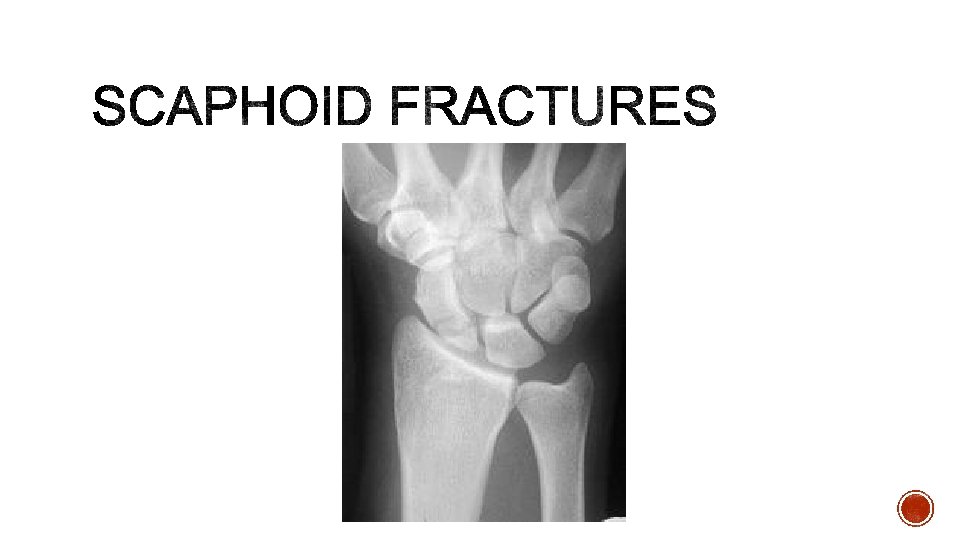
§ Most common carpal bone fracture § 15% of acute wrist injuries (waist 65% of time) § Mechanism § Axial load across hyper-extended and radially deviated wrist § Exam § Anatomic snuff box tenderness, pain with resisted ROM § What is major blood supply? § Imaging § X-ray: can get scaphoid view § Bone scan and MRI more sensitive
§ Thumb spica cast immobilization § Stable, non-displaced fractues § Surgical § Displaced fractures § Ortho referral: close outpatient follow up
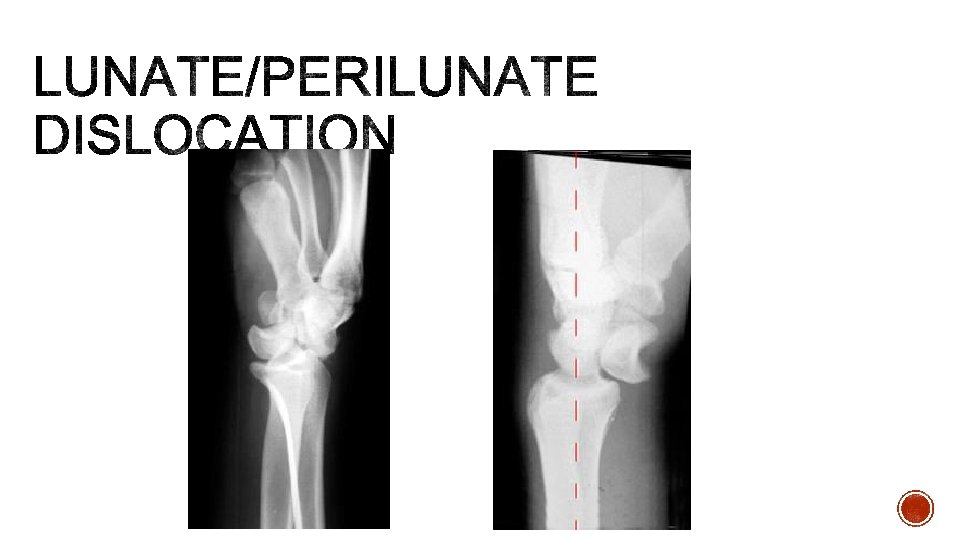
§ Missed 25% of the time on initial presentation § Perilunate: lunate stays in position while carpus dislocated § Lunate: lunate force volar or dorsal while carpus remains aligned § Mechanism § Traumatic, wrist extended and ulnarly deviated § Exam § Pain and deformity of wrist § Median nerve symptoms in 25% of patients § Imaging § X-rays
§ Always needs surgery § Emergent reduction prior to surgery can be done § Ortho referral: Urgent/Emergent
§ Most common variant of base of thumb fractures § Intra-articular fracture/dislocation of base of 1 st metacarpal characterized by volar lip of metacarpal based attached to volar oblique ligament (stays attached to trapezium) § Mechanism § Axial force applied to thumb § Exam § Pain at the base of 1 st metacarpal § Imaging § X-rays
§ Closed reduction & cast immobilization: non-displaced § Surgical: displaced § Ortho Referral: Urgent follow up § Epibasal thumb fracture
§ Common in Males § Mechanism § Direct blow to hand or rotational injury with axial load § Exam § Deformity, exam for signs of rotation, break in skin § Imaging § X-ray § Treatment: usually immobilization, surgical if very angulated or shortened § Ortho referral: close follow up for cast
§ Deformity caused by disruption of the terminal extensor tendon distal to DIP joint § Mechanism: direct blow to tip of finger causing forced flexion of DIP § Exam: finger tip rest at 45% flexion § Imaging: xrays § Treatment § Extension splinting for 6 -8 weeks with progressive flexion at 6 weeks § Ortho Referral: non-urgent outpatient
§ Avulsion injury of FDP from insertion at base of distal phalanx § Zone I flexor tendon injury § Mechanism: gripping with extension force § Exam: pain over volar distal finger § Imaging: x-ray § Management: Surgical, can splint prior to surgery (<3 weeks) § Ortho Referral: Needs urgent follow up
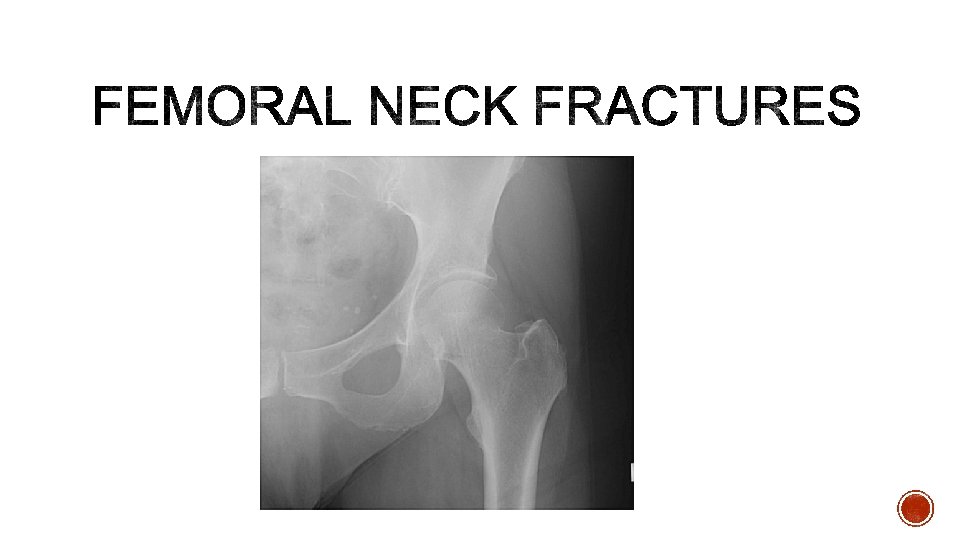
§ Increasingly more common due to aging population § Mechanism: falls in elderly, trauma in younger § Exam: § Displaced: leg in external rotation and abduction, with shortening § Impacted and stress fractures no obvious clinical deformity § Imaging: x-ray (MRI for occult) § Management: § Non-operative if not ambulatory prior to fracture § Operative otherwise § Ortho referral: Emergent if surgical
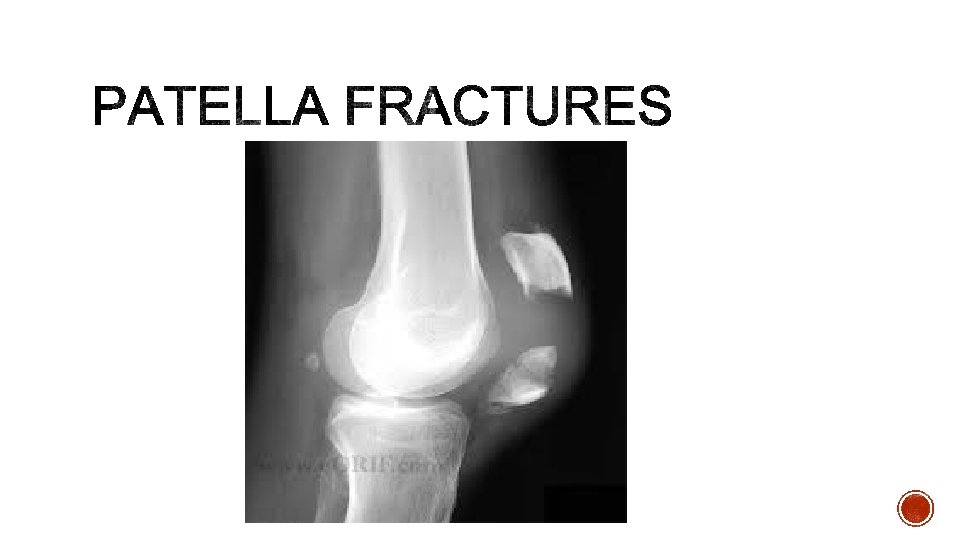
§ Check extensor mechanism § Management § knee immobilized in extension (brace or cylinder cast) and full weight bearing § intact extensor mechanism § nondisplaced or minimally displaced fractures § vertical fracture patterns § Ortho Referral: Urgent follow up
§ Incidence increasing as survival rates after motor vehicle collisions increase § Mechanism: high energy axial load § (motor vehicle accidents, falls from height) § 75% have associated fibula fractures § Management: § Non-operative: minimal displacement § Surgical: Most fractures § Ortho referral: Emergent
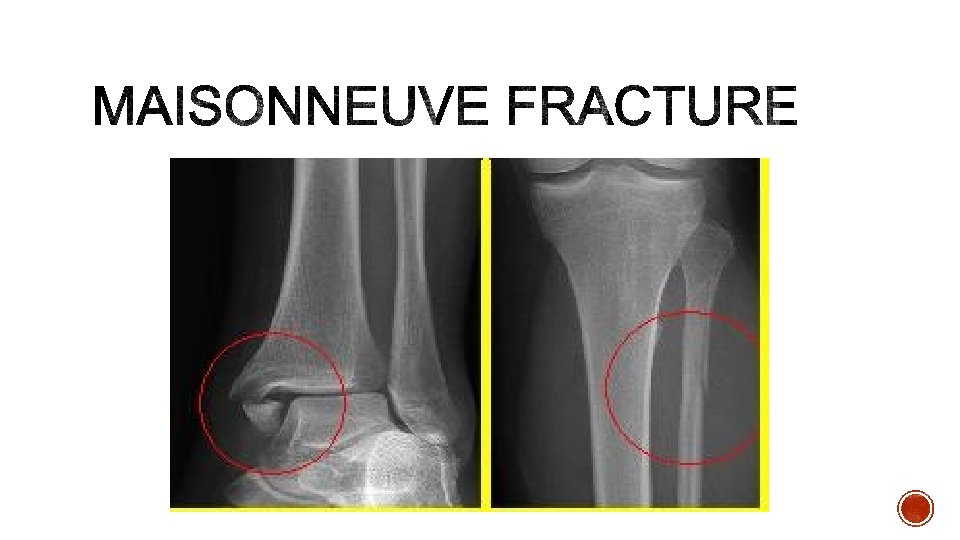
§ Mechanism § external rotation force to ankle w/ transmission of the force thru the interosseous membrane which exits thru a proximal fibular fracture § X-ray must obtain fibula § Management: § If stable can immobilize § Surgical for most § Ortho Referral: Urgent/Emergent
§ Mechanism: high energy in forced dorsiflexion with axial load § Hawkins classification § I: non-displaced § II: subtalar dislocation § III: subtalar and tibiotalar dislocation § IV: subtalar, tibiotalar, talonavicular dislocation (picture is type III)
§ Imaging: § X-ray: Canale View (optimal for neck) § CT scan for displacement § Treatment: § ALL cases require emergent reduction § Non-displaced: short leg cast 8 -12 weeks NWB for 6 weeks § Operative: all displaced fractures § Ortho referral: Emergent
§ Mechanism: traumatic axial loading § Avulsions can be due to different mechanisms (strong gastroc contraction or inversion plantar flexion) § Associated Injuries: § Extension to calcaneocuboid joint 63% § Vertebral injuries 10% § Contralateral Calcaneus 10% § High complication rate
§ Extra-articular (25%) or Intra-articular (75%) § Exam: § Diffuse tenderness § Ecchymosis § Shortened, widened, heel with a varus deformity § Imaging: § X-ray: reduced Bohler angle, increased angle of Gissane § CT is gold standard § MRI: for stress fractures
§ Treatment: § Stress fractures- cast with non-weight bearing for 6 weeks § Small extra-articular fracture with intact Achilles and small displacement and some intraarticular fractures –cast with non-weight bearing for 10 -12 weeks § All others are operative § Subtalar arthritis increased with non-operative management
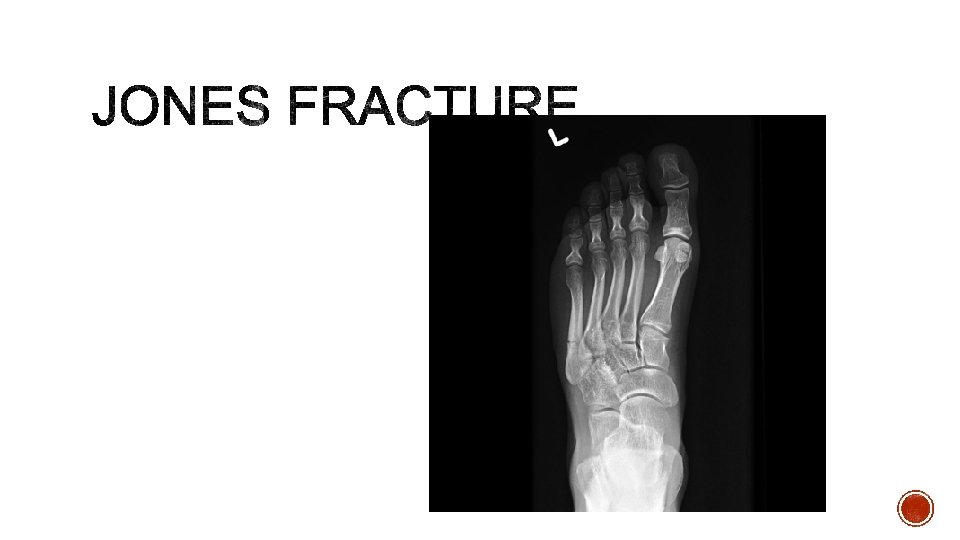
§ Metaphyseal-diaphyseal junction § Within 1. 5 cm distal to tuberosity of 5 th metatarsal § High risk of non-union § ED management § Splint § NWB § Treatment § Screw fixation § Prolonged immobiliazation and non-weightbearing
§ Avulsion fracture at base of 5 th metatarsal § Ankle inversion injury § Conservative treatment if non -displaced § WBAT
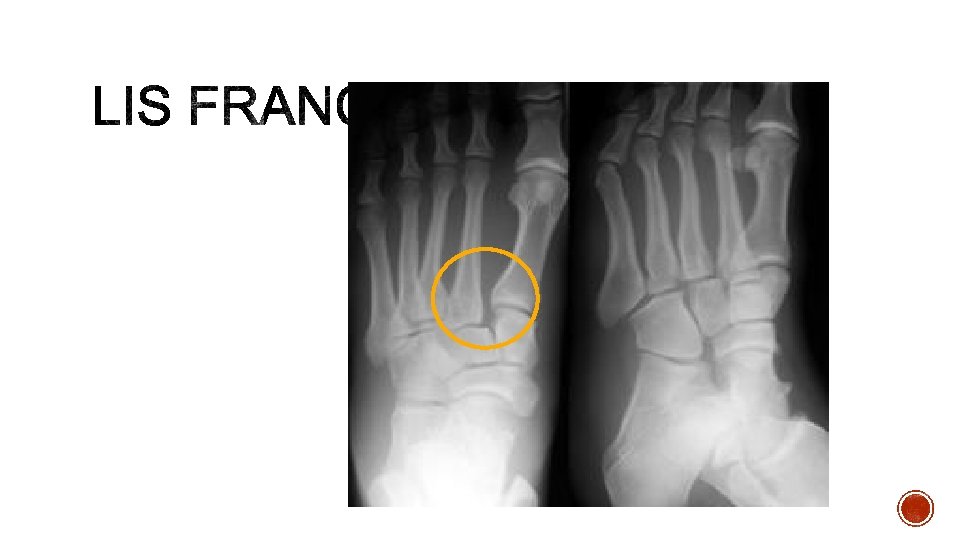
§ Axial load through a hyperplantar flexed foot § Injuries range from mild sprains to severe dislocations § Dislocations often associated with fractures § Metatarsal fractures in 95% § Tarsal fractures in 39%
§ Diagnostic clues § Midfoot swelling § Plantar bruising § Fleck sign § Avulsion of Lisfranc ligament from base of 2 nd metatarsal § Always consider compartment syndrome § Imaging: x-ray, always get stress views if you have high suspicion § MRI: for purely ligamentous injury § Treatment: § Cast for 8 weeks if non-displaced and no fracture § Surgery for most others
§ Clavicle: non-emergent § Boxers: non-emergent § Proximal Humerus: urgent/emergent § Mallet finger: non-emergent § Humeral shaft: non-emergent § Jersey finer: urgent § Supracondylar: urgent/emergent § Femoral neck: emergent § Radial head: non-emergent § Patella: urgent § Galeazzi: emergent § Pilon: emergent § Distal radius: non-emergent § Maisonneuve: urgent § Olecranon: non-emergent § Talar neck: emergent § Monteggia: emergent § Calcaneal: emergent § Ulnar/radial shaft: urgent § Jone’s: non-emergent § Scaphoid: non-emergent § Dancers: non-emergent § Lunate: emergent § Lis franc: urgent § Benett: urgent
§ Orthobullets. com § Radiopaedia. org § Wheelesonline. com