Epidemiology Classically speaking n n Epi upon among

 Demos = people Ology = science")







 of a specified disease at a")





 for disease in analytic")




















, exposed controls")
 Non-Smokers (less than 5 ) Case with lung cancer")







 2916 (b) 3000 (a+b)")

 n n It is ratio of incidence of the disease among")
 n n n This is defined as amount or proportion of")









 case detection, (ii) control of spread")






 Control (with out oral cancer) Gutka chewer 20 (a)")

, incidence (I) & duration (D) in epidemiology A. I=PD")



- Slides: 72
Epidemiology
Classically speaking n n Epi = upon (among) Demos = people Ology = science Epidemiology = the science which deals with what falls upon people…. .
A Modern Definition n “The study of the distribution and determinants of health-related states in specified populations, and the application of this study to control health problems. " (Last J) Search for knowledge Apply in health service
Objectives of Epidemiology 1. To describe the distribution and magnitude of health and disease problems in the population. 2. To identify the etiological factors – risk factors in the population. 3. To provide the data essential to planning, implementation and evaluation of services for prevention, control and treatment of disease and to setting up of priorities for these services.
The ultimate aim of epidemiology is n to eliminate or reduce health problem or its consequences and n to promote health and well-being of society as a whole.
Purposes of Epidemiology 1. 2. 3. 4. 5. To investigate nature / extent of health-related phenomena in the community / identify priorities To study natural history and prognosis of healthrelated problems To identify causes and risk factors To recommend / assist in application of / evaluate best interventions (preventive and therapeutic measures) To provide foundation for public policy
Component: Disease Frequency- Rate and Ratio e. g Rate- incidence rate, prevalence rate etc Ratio- sex ratio, doctor-population ratio Distribution of Disease in community find causative factor Generate hypothesis Descriptive epidimiology
Determinants of Disease. To test hypothesis Analytic epidemiology Help in develop sound scientific program
Incidence n Number of new cases of a disease which come into being during a specified period of time. (Number of new cases of specific disease during a given period)/(population at risk during that period) x 1000 Importance: If incidence increasing, it may indicate failure or ineffectiveness of control measure of a disease and need for better/new health control measure.
Prevalence Number of current case (old and new) of a specified disease at a point of time n It help to estimate the burden of disease n Identify potentially high-risk populations. They are essentially helpful to plan rehabilitation facilities, manpower needs, etc. (Number of current case of a specified disease at a point of time)/(estimated population at the same point of time) x 100 n Point prevalence AND Period prevalence n
Relationship between incidence and prevalence n Prevalence =Incidence x Duration
Approach of an epidemiologist Asking questions n making comparisons ● Asking questions may provide clues to cause or aetiology of disease e. g. What is the event, what is its magnitude, where did it happen, when did it happen, who were affected, why did it happen? n
Making comparisons will help draw inferences to support asking questions. n This comparison may be: ● Between those with the disease and those without the disease; ● Those with risk factor and those not exposed to risk factor; n
Terms to know n n n Endemic: constant presence of a disease in a given population epidemic: outbreak or occurrence of one specific disease from a single source, in a group population, community, or geographical area, in excess of the usual level of expectancy pandemic: epidemic that is widespread across a country, or large population, possible worldwide
Epidemiology versus clinical medicine Epidemiology n n Unit of study is a defined population or population at risk Concerned with sick as well as healthy Investigator goes to the community identify source of infection, mode of spread, an Etiological factor, future trend or recommend control measures Clinical medicine n Unit of study is case n Concerned with only sick n n Patient comes to doctor Seeks diagnosis, derives prognosis, prescribes specific treatment
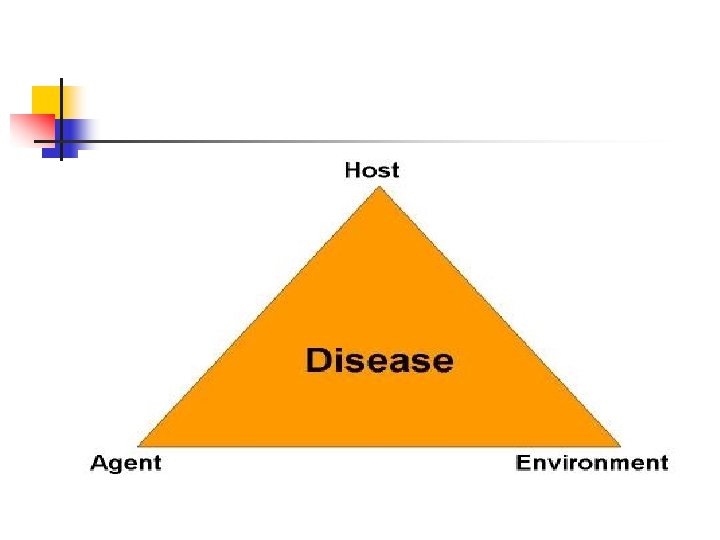
Three essential characteristics that are examined to study the cause(s) for disease in analytic epidemiology are. . . n n n Host Agent Environment
Host Factors n n n Behaviors Genetic predisposition Immunologic factors • Influence the chance for disease or its severity
Agents n n n Biological Physical Chemical • Necessary for disease to occur
Environment n External conditions • Contribute to the disease process
Epidemics arise when host, agent, and environmental factors are not in balance n n Due to new agent Due to change in existing agent (infectivity, pathogenicity, virulence) Due to change in number of susceptibles in the population Due to environmental changes that affect transmission of the agent or growth of the agent
EPIDEMIOLOGICAL METHODS. The methods he employs can be classified as: 1. Observational studies a. Descriptive studies b. Analytical studies – Case control studies – Cohort studies 2. Experimental/interventional studies – Randomized control studies – Field trials – Community trials
Descriptive observations pertain to the “who, what, where and when of healthrelated state occurrence”. However, analytical observations deal more with the ‘how’ of a health-related event occur. Randomized control trial (often used for new medicine or drug testing), field trial (conducted on those at a high risk of conducting a disease), and community trial (research on social originating diseases)
Descriptive Studies Steps in conducting a descriptive study. Descriptive studies form the first step in any process of investigation. These studies are concerned with observing the distribution of disease in populations. 1. Defining the population. 2. Defining disease under study. 3. Describing the disease. 4. Measurement of disease 5. Compare 6. Formulate hypothesis-
Defining the population. Defined population may be the whole population or a representative sample. n It can also be specially selected group such as age and sex groups, occupational groups, hospital patients, school children, small community, etc.
2. Defining disease under study. 3. Describing the disease. Disease is examined by the epidemiologist by asking three questions: ● When is the disease occurring—time distribution? ● Where is it occurring—place distribution? ● Who is getting the disease—person distribution?
A. Time Distribution n Short-term fluctuations. Common source epidemics - single exposure/point source—bhopal tragedy Propagated-infectious : Hep A n n Periodic fluctuations; Seasonal –measles (early spring) cyclic, , in pre-vaccinated era (peak 2 -3 yr) Long-term or secular trends; diabetes, CVD
B. Place Distribution n International variations: Cancer of stomach very common in Japan less common in US. oral cancer- India Breast cancer- Low-japan, high-western n National variations, e. g. Distribution of fluorosis,
n n Rural-urban differences, e. g. CVD, Mental illness more common in urban areas. Skin diseases, worm infestations more common in rural areas. Local distributions, e. g. Spot maps- John Snow in London to incriminate water supply as cause of cholera transmission in London.
cholera cases in proximity to water pump, 1854
C. Person Distribution Age: e. g. Measles is common in children, Cancer in middle age Degenerative diseases in old age. Sex: Women- Lung cancer-less Hyperthyroidism- more c. Social class- Diabetes, Hypertenson– upper class
4. Measurement of disease- Mortality/ Morbidity 5. Compare- Between different population, subgroups 6. Formulate hypothesis. On basis of all data epidemiologist form hypothesis.
Cross-sectional studies n n n Cross-sectional study is also called prevalence study. Cross-sectional study is the simplest form of observational study. It is based on single examination of cross-section of population at one point of time. If the sampling methodology is accurate, results can be projected to the entire population. They are more useful for chronic illnesses, e. g. hypertension. Cross-sectional studies save on time and resources, but provide very little information about natural history of disease and incidence of illness.
Case- control studies n n n It start from effect and then proceed to cause Both exposure and outcome have occurred before start of the study The study proceeds backwards from effect to cause
n n Select subjects based on their disease status. A group of individuals that are disease positive (the "case" group) is compared with a group of disease negative individuals (the "control" group). The control group should ideally come from the same population that gave rise to the cases.
Basic steps in a case-control study n 1. Selection of cases and controls n 2. Matching n 3. Measurement of exposure n 4. Analysis and interpretation.
n n A 2× 2 table is constructed, displaying exposed cases (A), exposed controls (B), unexposed cases (C) and unexposed controls (D). CASE CONTROLS EXPOSED A B UNEXPOSED C D To measure association is the odds ratio (OR), which is the ratio of the odds of exposure in the cases (A/C) to the odds of exposure in the controls (B/D), i. e. OR = (AD/BC).
Smokers (less than 5 ) Non-Smokers (less than 5 ) Case with lung cancer 33 (a) Control without lung cancer 55 (b) 2 (c) 27 (d) The first step is to find out 1. Exposure rates among cases =a/(ac) = 33/35 =94. 2% 2. Exposure rate among the controls =b/(bd) = 55/82 =67%
n n n If the exposure rate among the cases is more than the controls. We must see if the exposure rate among the cases is significantly more than the controls. This is done by using the chi-square test It is significant if p is less than 0. 05.
Odds ratio It is a measure of strength of association between the risk factor and outcome. n The derivation of the odds ratio is based on three assumptions: ● The disease being investigated is relatively rare ● The cases must be representative of those with the disease ● The controls must be representative of those without the disease. n
Odds ratio a. d/b. c 33 X 27/55 X 2 = 8. 1 n People who smoke less than 5 cigarettes per day showed a risk of having lung cancer 8. 1 times higher as compared to non-smokers.
n OR is > 1 - "those with the disease are more likely to have been exposed, " OR close to 1 then the exposure and disease are not likely associated. OR <1 -exposure is a protective factor in the causation of the disease.
n n Case control studies are usually faster and more cost effective Sensitive to bias (selection bias). The main challenge is to identify the appropriate control group; The distribution of exposure among the control group should be representative of the distribution in the population that gave rise to the cases.
Cohort Study n n It look at cause and proceed to effect study before the disease is manifest and proceed to study over a period of time for the disease to occur. Cohort means a group of people sharing a common experience. Cohort studies are often prospective studies, they can be retrospective also, or a combination of both prospective and retrospective components can be brought in.
n 1. 2. 3. 4. 5. Steps in a cohort study: Selection of study subjects Obtaining data on exposure Selection of comparison groups Follow-up Analysis.
CHD Develop CHD does not total develop Smoker 84 (a) 2916 (b) 3000 (a+b) Non-smoker 87 (C) 4913 (d) 5000 (c+d) Total 171 (a+c) 7829 (b+d) 8000 The incidence rates of CHD among smokers i. e. a/(a+b) =84/3000 =28 per 1000 The incidence rates of CHD among non-smokers i. e. =c/(c+d) =87/5000 =17. 4 per 1000
n Then, we must determine if the incidence rate among the smokers is significantly more than among the nonsmokers by using the chi-square test.
Relative risk (RR) n n It is ratio of incidence of the disease among the exposed and incidence among the non-exposed. RR (incidence of disease among exposed)/ (Incidence of disease among non-exposed) =a/(ab)/c/(cd) =28/17. 4 =1. 6 If RR is more than 1, then there is a positive association If RR is equal to 1, then there is no association Smokers develop CHD 1. 6 times more than nonsmokers.
Attributable risk (AR) n n n This is defined as amount or proportion of disease incidence that can be attributed to a specific exposure. It indicates to what extent the disease under study can be attributed to the exposure: (incidence of disease among exposed) - (incidence of disease among non exposed)/ (Incidence of disease among exposed) =28 -17. 4/28 = 10. 6/28 = 0. 379 = 37. 9% of CHD among the smokers was due to smoking.
Differences between case-control and cohort studies Case-control n n Proceeds from effect to cause Starts with the disease exposed Rate of exposure among exposed and those not and exposed is studied First approach to testing hypothesis Cohort studies ● Proceeds from cause to effect ● Starts with people to risk factor ● Tests frequency of disease among those exposed those not exposed ● Reserved for testing precisely define hypothesis
n Involves small number of subjects Less time and resources n Suitable for rare diseases n Yields odds ratio n n Cannot yield information about diseases one other than selected for ● Involves large number of subjects ● More time and cost intensive ● Difficult to conduct for rare diseases ● Yields incidence rates, RR, AR and population atributable risk ● Information about more than disease is possible
Randomized Control Studies Essential elements are: n Drawing up a strict protocol, n selecting reference and experimental populations, n randomization, n intervention, n follow-up n assessment of outcome.
n Randomization is a statistical procedure where participants are allocated into groups called study and control groups to receive or not to receive an experimental therapeutic or preventive procedure, intervention. Randomization is an attempt to avoid bias and allow comparability.
n Study designs include Concurrent parallel Crossover type of study designs. n In the former, study and control groups will be studied parallel whereas in the latter all the participants will have the benefit of treatment after a particular period because the control group becomes study group.
Types of randomized control studies are: n n Clinical trials, e. g. drug trials Preventive trials, e. g. trials of vaccines Risk factor trials, e. g. trials of risk factors of cardiovascular disease, e. g. tobacco use, physical activity, diet, etc. Cessation experiments, e. g. smoking cessation experiments for studying lung cancer.
What is bias? Bias is systematic error that comes in. n Bias on the part of participants if they know they belong to study group—participant bias n bias because of observer if he knows that he is dealing with study group—observer bias n bias because of investigator bias, if he knows he is dealing with study group. In order to prevent this, a technique called blinding is adopted. n
Concept of blinding n n n Single blind trial means participant will not know whether he belongs to study group or control group. In double blind studies, both the participant and the observer will not be aware. In triple blind study, the participant, observer as well as the investigator will not be aware
SCREENING n n Active search for apparently healthy people is called screening. It is defined as search for unrecognized disease or defect by rapidly applied tests, examinations or other procedures in apparently healthy individuals. Basic purpose of screening is to sort out from a large group of apparently healthy individuals—those likely to have disease, bring those apparently abnormal under medical supervision and treatment. Efforts to detect cancer before symptoms appear
n Four main uses of screening are: (i) case detection, (ii) control of spread of infectious diseases (iii) research purposes especially for studying the natural history of chronic diseases (iv) screening programs have lot of opportunities to educate people.
n n Iceberg phenomenon of a disease explains progress of disease from subclinical stages to overt manifestation. Floating tips represent what the dental surgeon see and hidden portion represents unrecognized disease. Its detection and control are challenges.
n n Iceberg phenomenon of a disease explains progress of disease from subclinical stages to overt manifestation. Floating tips represent what the dental surgeon see and hidden portion represents unrecognized disease. Its detection and control are challenges.
Q-1 Incidence of any disease can be known by: A. Longitudinal study. B. Cross-sectional study. C. Retrospective study. D. Case control study. n
Q-2 A study in which a particular individual is studied at different age is called as: A. Retrospective study B. Prospective study C. Cross sectional study D. Longitudinal study n
Q-3 When planning of the entire study is completed before data is collected analysed is cosidered as: A. Retrospective study B. Prospective study C. Cross sectional study D. Longitudinal study n
Q-4 Case control study is a part of: A. Descriptive epidemiology B. Experimental epidemiology C. Analytical epidemiology D. Serological epidemiology n
Q-5 Cases (Oral cancer ) Control (with out oral cancer) Gutka chewer 20 (a) 15 (b) Non Gutka chewer 15 (c) 20 (d) Odds ratio (OR) of getting oral cancer in gutka chewers is: 0. 44 1. 0 1. 7 2. 5
Q-6 Hypothesis is: A. A report. B. A synopsis. C. A theory. D. A supposition from an observation. n
Q-7 Relationship of prevalence (P), incidence (I) & duration (D) in epidemiology A. I=PD B. P=ID C. D=PI D. none n
Q-8 Constant presence of a disease in a given population A. Endemic B. Pandemic C. Epidemic D. Sporadic n
Q-9 Which one is not the step of descriptive study a. Describing the disease. 4. Measurement of disease 5. Blinding 6. Formulate hypothesis
Q-10 In descriptive epidemiology, Describing the disease in all except a. When is the disease occurring b. Where is it occurring c. Who is getting the disease d. How is the disease occure