CPC as Cinema The Producers starring Drs Troy


![The Setting • Polysubstance abuse [nicotine, alcohol, iv cocaine, pot] • Bipolar disorder •](https://slidetodoc.com/presentation_image_h2/3fbe9d29998b2d7c1f9c889aa281e2ef/image-3.jpg "The Setting • Polysubstance abuse [nicotine, alcohol, iv cocaine, pot] • Bipolar disorder •")



![Toxicology studies • Opiates (expected, hydrocodone) - [ not cause of her liver disease]](https://slidetodoc.com/presentation_image_h2/3fbe9d29998b2d7c1f9c889aa281e2ef/image-7.jpg "Toxicology studies • Opiates (expected, hydrocodone) - [ not cause of her liver disease]")


 • Liver, acute fulminant process • Brain")

 • •")

 PROS: • • demographics history of Grave’s very high AST/ALT presentation")

 apical blood bile ? ceruloplasmin vesicles apoceruloplasmin murr 1 ATP 7 b")

 • HEPATIC •")
 •")
 • Fatty infiltration")











 •")
 Nefazodone-induce acute liver failure and hepatic encephalopathy 2) Carbamazepine-induce")










- Slides: 45
CPC as Cinema • “The Producers”, starring Drs. Troy Wadsworth and Nilam Soni • “Clueless”, starring Mark Feldman • “The Sting”, starring Dr. Dale Odell
The Plot: 45 year old divorcee with acute delirium • associated with hepatic • disease (jaundice, • • abnormal liver chemistries and asterixis). Asterixis (liver flap) Hepatic failure Respiratory acidosis Uremia Cerebrovascular disease
The Setting • Polysubstance abuse [nicotine, alcohol, iv cocaine, pot] • Bipolar disorder • Taking at least 6 other drugs: – hydrocodone and acetaminophen for back pain – risperidone, citalopram, carbamazepine, nefazodone – she is prone to drug OD if depressed • Grave’s disease treated with RAI twice- currently on T 4
Her exam findings • GENERAL: icteric, • ABDOMEN: mild RUQ overweight tenderness; 8 cm liver; no ascites/splenomegaly • VITALS: afebrile; + tilt • EXTREMITIES: no edema • HEENT: dry mucosae; blood in mouth and on • NEURO: alert but chin; poor dentition agitated and disoriented; asterixis • CHEST: normal
Laboratory test abnormalities • Liver: bili 5. 5, ALT 3, 539, AST 2, 233, AP 253, NH 3 59, PT/INR 26. 3/2. 1, Alb 3. 0, TP 6. 2, Glob 3. 2, platelets 274 K, Hgb 12. 3 • Other: Anion gap 14; K 3. 2, P 2. 3, TSH 0. 06 u. IU/m. L (all low). • Renal/urine: BUN 49, Creatinine 3. 3, ratio 15: 1, small bilirubin, SG 1. 023, 17 WBC, 8 RBC, mod bacteria, + nitrite, urobilinogen > 8 mg/d. L (normal, 0. 1 -1. 0 mg/d. L)
High Urine Urobilinogen our patient has liver disease, hemolysis, or both
Toxicology studies • Opiates (expected, hydrocodone) - [ not cause of her liver disease] Aspirin - [ not cause of her gap acidosis] • APAP • • Carbamazepine- slightly toxic range signs of toxicity: clumsy, unsteady, confused, dizzy, drowsy – ? due to OD, liver failure with metabolism, or drug-drug interaction with nefazodone • Nefazodone-induced carbamazepine toxicity. Am J Psychiatry 153: 733, 1996 • Cabamazepine-nefazodone interaction in healthy subjects. J Clin Psychopharmacol 20: 46 -53, 2000 – ? role of carbamazepine in causing liver failure
Why this looks like acute liver failure • Short history of encephalopathy • No ascites, splenomegaly, spider angiomas, or laboratory signs of chronic liver disease (e. g. , thrombocytopenia, anemia) • Slightly low albumin, markedly depleted hepatic-derived clotting factors
Half lives of certain proteins synthesized in the liver • • • Albumin: 18 days Fibrinogen (factor I): 3 -5 days Prothrombin (factor II): 2 -5 days Factor X: 1 -2 days Factor IX: 18 -24 hours Factor VII: 8 -12 hours
Systems involved (when considering her differential diagnosis) • Liver, acute fulminant process • Brain (hepatic encephalopathy vs other) – Neurologic: falls, dysarthria – Psychiatric: bipolar disorder • Kidneys – acute renal failure. presumably – abnormal urinary sediment
Causes of acute liver failure in US and other Western nations • • Acetaminophen hepatotoxicity Acute viral hepatitis (B > A>> others) Unknown causes (cryptogenic) Other, known causes 34% 25% 19% 12% • AIH, Wilson disease • Budd-Chiari, AFLP, liver cancer, liver ischemia, Reye’s • Other drugs (non-APAP) or toxins • Drugs • Toxins: mushrooms, CCl 4, sea anemone sting 10%
Five factors predicting high mortality in patients with fulminant hepatic failure (non-acetaminophen) • • • Negative serologic tests for HAV and HBV Age < 10 or > 40 * Jaundiced > 7 days before encephalopathy Prothrombin time (PT) > 50 seconds Total serum bilirubin > 17. 6 mg/d. L 1 factor 80% mortality without OLT 3 factors, or PT > 100 seconds >95% mortality [O’Grady et al. King’s College (London) data base of 588 patients with fulminant hepatic failure. Gastroenterology 97: 439, 1989]
Acute viral hepatitis A-E PROS: CONS: • most common cause of • all tests for A-E icteric illness with viruses were negative high transaminases • HCV RNA not given; • history of IVDU and however, severity of tattoos liver disease with encephalopathy is un • anti-HCV is not highly common with acute C sensitive for acute C
Autoimmune hepatitis (AIH) PROS: • • demographics history of Grave’s very high AST/ALT presentation with liver failure is possible in AIH CONS: • no ANA, ASMA mentioned • normal serum globulins • other organ systems involved
Wilson disease • Autosomal recessive; 1/30, 000 in all ethnic groups; 1 in 90 carry a mutated Wilson disease gene (ATP 7 b) • ATP 7 b (13 q 14) codes for a trans-Golgi P-type ATPase, with 6 copper binding sites • Gene is expressed in liver, kidney, and placenta • Mutations in ATP 7 b lead to copper accumulation in liver, kidney, brain, and cornea • > 200 mutations have been reported, most in single families, but certain mutations have been reported in many families, such as H 1069 Q, found in 40% of Caucasians • Hepatic expression of ATP 7 b facilitates copper excretion into bile and copper attachment to apoceruloplasmin and genesis of ceruloplasmin for transport to tissues
COPPER (unabsorbable) apical blood bile ? ceruloplasmin vesicles apoceruloplasmin murr 1 ATP 7 b WILSON Liver Cell Golgi network atox 1 chaperone COPPER sinusoidal Ctr 1 Diet Upper GI absorption portal vein (Alb-Cu, His-Cu) periphery (His-Cu)
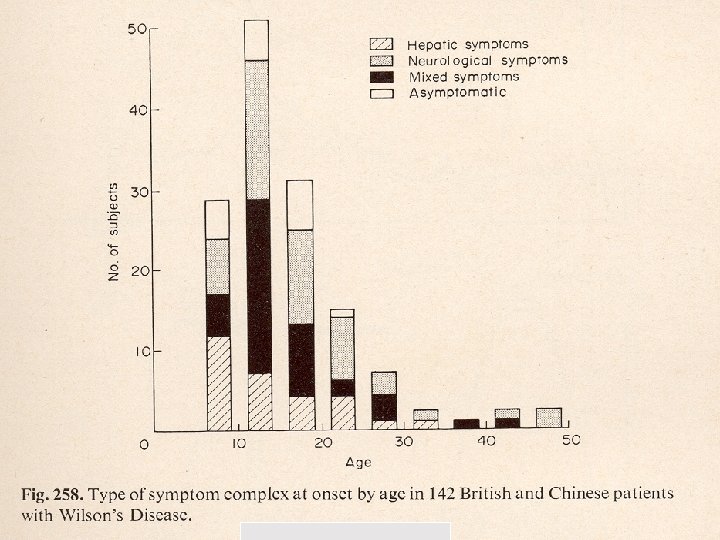
Wilson disease: presentations • Progressive neurological disorder, without clinically prominent liver disease – as described by Wilson (1912), an American-born neurologist practicing in Britain who called the disease progressive lenticular degeneration • • Liver disease only, fulminant ( F > M ) or chronic Psychiatric illness Isolated acute hemolysis Combinations of the above
Proposed Classification (Ferenci et al. Liver Int’l 23: 139 -142, 2003) • HEPATIC • H 1 acute, fulminant • H 2 chronic • NEUROPSYCHIATRIC • N 1 with liver disease, usually chronic • N 2 without symptomatic liver disease • NX liver disease not investigated
Psychiatric issues in patients with Wilson disease (Arch. Gen. Psychiatry 46: 1226, 1984) • Prevalence around 20% • More common in adults than in adolescents and children • Depression is the most common problem • Others include bipolar, neuroses, phobias, compulsive behaviors, aggressive behavior, antisocial behavior
Other occasional features of Wilson disease • Calcium bilirubinate gallstones (hemolysis) • Fatty infiltration of the liver • Renal abnormalities – – – – Microscopic hematuria Proteinuria Hypophosphatemia due to phosphaturia Glycosuria Hypouricemia due to uricosuria Renal tubular acidosis Aminoaciduria Renal stones / nephrocalcinosis
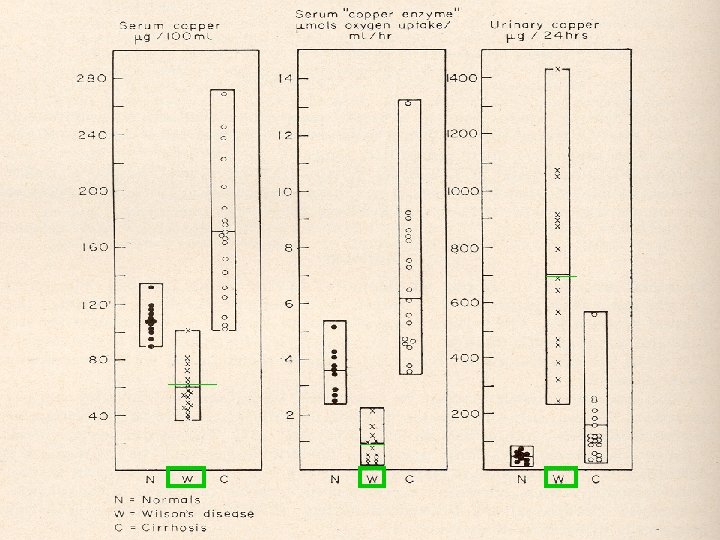
Tests in Wilson disease • No single test is 100% sensitive or specific • Slit lamp exam if K-F rings not visible to naked eye – Present in 50% of hepatic cases – Present in 98% of neuropsychiatric cases – “Sunfower” cataracts in ant. lens (green/gray) • Ceruloplasmin in 67 -80% of hepatic cases (low normal in others due to acute phase reactant) • Serum copper low unless hemolysis • Urine copper high in adults • Hepatic copper > 250 ug/g dry weight with minimal overlap with cholestatic liver diseases such as PBC, PSC • Mutation analysis not widely available, too slow for fulminant cases, but useful if mutation in proband is known
THE KAYSER - FLEISCHER CORNEAL RING
Her sister: clinical heterogeneity despite genetic homogeneity ? … patients homozygous for specific alleles (e. g. , H 1069 Q) reveal little correlation between age at onset, clinical features, biochemical parameters, or disease activity. … clinical heterogeneity seen among affected siblings and identical twins supports that additional genetic and environmental factors contribute to the outcome in any given patient. Tao and Gitlin. Hepatology 37: 1241 -1247, 2003.
Therapy of Wilson disease • Low Copper diet – liver, kidney, nuts, chocolate, shellfish, and mushrooms • Chelation – Penicillamine [3 -mercapto-D valine](+ 50 mg pyridoxine/day) – Trientene • Reduced GI absorption – zinc p. o. induces intestinal metallothionein which prefers Cu to Zn, binds Cu but does not transport it, and is then eventually shed into feces • Chelation plus reduced GI absorption – Ammonium tetrahydromolybdate (experimental); may be safer and better CNS-tolerated than penicillamine • Antioxidants, such as alpha-tocopherol (vitamin E) • Liver Transplantation – Fulminant presentation, mortality without OLT 100% – Severe chronic disease unresponsive to medical therapy
Wilson disease PROS: • Fulminant hepatic failure presentation • Sister died age 14 of fulminant disease • Concomitant neuropsychiatric and renal abnormalities CONS: • Many classic features of Wilson disease are lacking in this patient
Classic features of H 1 Wilson disease LACKING in this patient • Onset of fulminant liver disease before age 40 and usually much earlier • AST is usually > ALT, often 4: 1 • AST and ALT are usually < 1500 • Alkaline phosphatase is usually normal or even low • Disproportionately high serum bilirubin from acute hemolysis
Some drugs and herbals causing acute liver failure DRUGS: HERBALS: Isoniazid Halothane Sulfonamides Phenytoin Valproic acid Troglitazone Carbamazepine Nefazodone Jin Bu Huan (Anodyne) Chinese herbal teas Chaparral others
Carbamazepine and liver damage • Abnormal LFTs, jaundice with cholestatic or hepatocellular pattern have been reported (PDR) • Cases of granulomatous hepatitis and vanishing bile ducts have been reported as well • Some cases are part of immunoallergic reaction, while others are idiosyncratic • Most cases have been in children and the elderly, and some have associated with renal failure • Many case reports with some fatalities
Nefazodone and liver damage • Selective 5 -HT 2 RA, • Several published reports of • Non-selective inhibitor hepatotoxicity since of serotonin and 1999, with one case norepinephrine rethat was re-challenged uptake by nerves • Severe injury with very high serum transaminases and jaundice
Nefazodone hepatotoxicity case age sex dose/d time co-Rx chlorazepate 1 a 54 F 200 28 wk 2 a 16 F 400 14 wk 3 a 57 F 200 25 wk 4 b 27 M 400 ? ? ? 5 c 73 F 400 5 wk lorazepam ? ? ? Carbamazepine, others Our pt 45 F 500 Dxs BP, T 3 on Rx a, Annals Int Med; b, Med J Australia; c, Dig Dis Sciences [all 1999]
Nefazodone, continued Signs/ss outcome 1 J, HE Dead 34 1760/ 2040 2. 1 29 2 J OLT 23 1296/ 1345 4. 3 25 3 J, HE Well 12 955/ 1626 3. 0 13 4 N, V Well 3 453/ 1172 5 J, pain Dead 17 1318/ 834 Case BR Our pt J, HE ? ? ? 6. 6 AST/AL T 2233/ 3539 Alb PT, s 15 3. 0 26
Histopathology of nefazadone hepatotoxicity • Initial injury in zone 3 (center of lobule) • Collapse of liver architecture, apoptosis, and confluent necrosis which spreads from center of lobule to its periphery • Diffuse hepatocyte ballooning • Lymphocytic infiltration • Nodules surrounded by fibrosis (may progress to cirrhosis) • Canalicular cholestasis with periportal pseudoglandular formation ( ductular proliferation)
Final list of possibilities 1) Nefazodone-induce acute liver failure and hepatic encephalopathy 2) Carbamazepine-induce acute liver failure 3) Wilson disease with fulminant liver failure 4) 5) 6) 7) Autoimmune hepatitis Acute viral hepatitis from HSV, EBV, HCV Ingestion of a toxin, eg Amanita phalloides Hepatic replacement with unsuspected cancer
What was the “diagnostic” procedure? • Liver biopsy after FFP, with copper stain and copper content if histologic features compatible with Wilson – NOTE: she should be referred to OLT facility • • Slit lamp exam, 24 hr urine copper output ANA, ASMA, good response to steroids HCV RNA – unlikely Hepatic imaging showing hepatic metastatic disease- unlikely
CPC as cinema. It’s show time!
Thyrotoxicosis, with hepatic dysfunction PROS: • liver disease occurs in thyrotoxicosis • has history of Grave’s refractory to RAI • Current TSH is low CONS: • liver disease usually not this severe • no clinical signs of hyperthyroidism • she was taking exogenous thyroid hormone, perhaps in excess • also may have sick euthyroid syndrome with low TSH
Choledocholithiasis PROS: • has gallstones on US • US may miss CBD stones CONS: • transaminases too high • encephalopathy • US shows no dilation of biliary system • urinary urobilinogen
Budd-Chiari syndrome PROS: CONS: • acute presentation with • absence of abdominal abnormal liver tests pain and tenderness and liver failure • no hepatomegaly • no ascites • no known risk factors
Alcoholic hepatitis PROS: • history of alcoholism • fattly change on US CONS: • • • no recent alcohol use blood alcohol negative transaminases too high ALT > AST no hepatomegaly
NAFLD / NASH • • PROS: CONS: not currently drinking obese fatty liver on US ALT > AST • liver is not large • encephalopathy rare • transaminases too high
BILIARY BLOCKAGE Via blood bilirubinuria Urobilinogen low or absent Kidney X BR Blood/RES BR-MG Liver BR-DG X BR + 2 Gluc X Bile Intestine stercoobilinogen acholic Feces
Heme biliverdin BR 1 2 3 Blood/RES urobilinogen BR-MG Liver 3 BR-DG Bile portal vein bacteria BR + 2 Gluc Urobilin (yellow) oxidation UROBILINOGEN Kidney bacteria Intestine stercobilinogen oxidation stercobilin Feces 1, heme oxidase; 2, biliverdin reductase; 3, bilirubin UDP glucuronyltransferase