Chemotherapy induced nausea and vomitingupdate and implementation 2020














Receptor Antagonists Core stone of antiemetic regimens")
Receptor Antagonists pallonesetron Second generation of 5")


Receptor Antagonists Side effects headache- 40%– constipation")


 961 9")






 Antagonists for Acute Emesis AGENT Ondansetron")
 Dosing DEXAMETHASONE - Acute Emesis High Risk - Delayed Emesis -")




- Slides: 45
Chemotherapy induced nausea and vomitingupdate and implementation 2020 GOLPUR MICHAL, RN, MHA ONCOLOGY WARD SHEBA MEDICAL AENTER
Advances in both cytotoxic therapy and supportive care Patients undergoing Ct still suffer from CINV More then 50%patients undergoing HEC or MEC experience CINV Guidelines issued by oncological societies have stressed the importance of preventing CINV.
Nausea is more common then vomiting Difficulties to control Cause suffering and reduce the QOL Healthcare providers often underestimate the incidence of CINV – especially delayed v+n
Emetic risk groups – Adults - Single IV Agents
Emetic risk groups – Adults - Single IV Agents
Emetic risk groups – Adults - Single IV Agents
Emetogenic Potential: oral Agents
We need to tailor the appropriate entiemetic regimen to individual patients who could benift from brief or extanded xntiemetic coverage
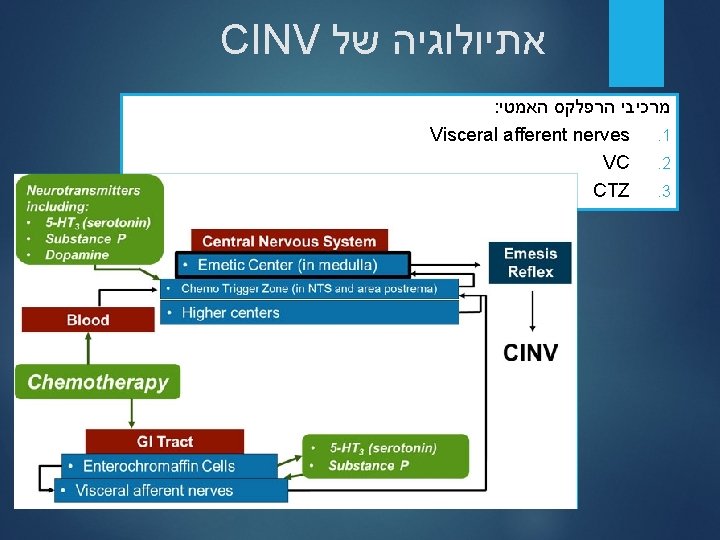
Physiology of Chemotherapy-Induced Emesis Adapted from: Grunberg S, et al. NEJM. 1993; 329: 1790 -1796.
Neurotransmitters and Antiemetics Dolasetron Granisetron Ondansetron Palonosetron Tropisetron and others Metoclopramide Haloperidol Dopamine / D 2 RAs Histamine Serotonin / 5 -HT 3 RAs Endorphins Emetic reflex Substance P / Aprepitant NK 1 RAs Acetylcholine Netupitant Rolapitant GABA Cannabinoids D 2, dopamine; GABA, gamma-aminobutyric acid; NK, neurokinin; Ras, receptor antagonists, 5 -HT 3: 5 -hydroxytryptamine 3 Gralla RJ, et al. J Clin Oncol. 1999; 17(9): 2971 -2994. Grunberg SM, et al. N Engl J Med. 1993; 329(24): 1790 -1796. Hesketh PJ. Support Care Cancer. 2001; 9(5): 350 -354.
TYPES OF CINV Acute-onset Occurs within a few minutes to several hours after the drug administration and resolves within the first 24 hours. the occurrence is influenced by the intrinsic and extrinsic factors and the environment in which the CT is administered mechanism of action- serotonin.
TYPES OF CINV Delayed-onset Develop more then 24 hours after CT and can last 6 to 7 days The maximal intensity depends on the type of CT(CISP reaches its maximal intensity 48 -72 hours after administration of CT mechanism of action- substance P
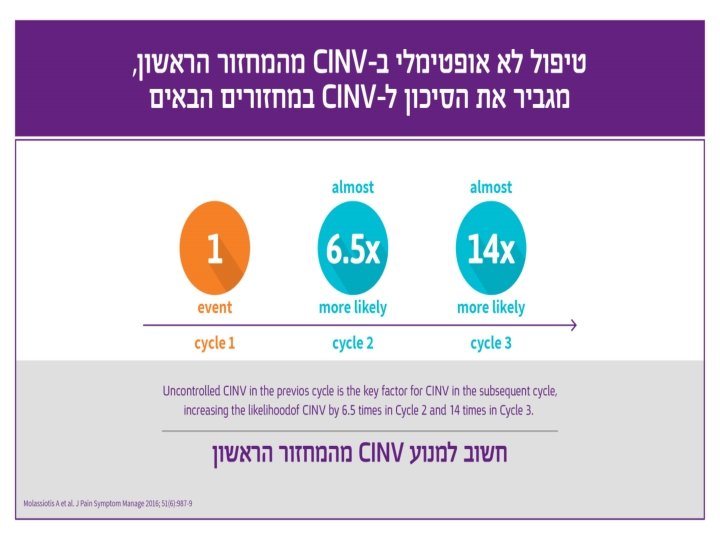
TYPES OF CINV Anticipatory Patients who are not well controlled during the first cycle of CT Occur before patients receive their next CT. Conditional response- occurs after a negative past experience with CT. 10 -33% of patients The most effective treatment is preventing Use the antianxiety agent lorezapam combined with antiemetics
TYPES OF CINV Breakthrough emesis Vomiting that occurs despite prophylactic treatment and requires “rescue” with antiemetic agents Refractory emesis Emesis that occurs during subsequent treatment cycles when antiemetic prophylaxis and/or rescue have failed in earlier cycles
types of Antiemetic therapies Serotonin (5 -HT 3)Receptor Antagonists Core stone of antiemetic regimens First generation Ondansetron(Zofran), Granisetron(K ytril) Exhibit the same emesis control Effective in controlling acute n+v
types of Antiemetic therapies Serotonin (5 -HT 3)Receptor Antagonists pallonesetron Second generation of 5 HT 3 RA 100 -fold higher binding affinity for 5 HT 3 RA Half-life of approximately 40 hours Prolong inhibition of 5 HT 3 R Prevent n+v in acute and delayed emesis
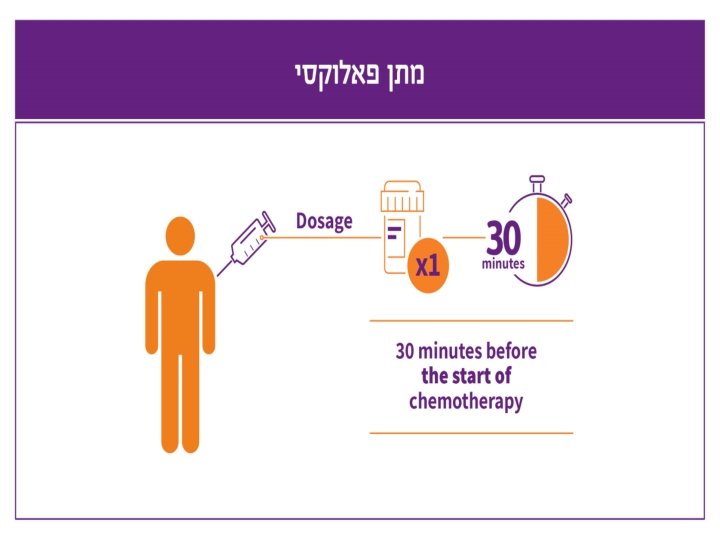
types of Antiemetic therapies Single dose of 0. 25 mg The preferred 5 HT 3 RA in MEC setting (ASCO, NCCN 2017) Approved for children older then 1 month- 20 Do not prolong QT interval
Palonosetron has a Longer Plasma Half-life and a Higher Binding Affinity to 5 -HT 3 Receptors 5 -HT 3 Antagonist t 1/2 (h) 5 -HT 3 Antagonist Binding Affinity (p. Ki) Palonosetron 40. 0 Palonosetron 10. 45 Ondansetron 4. 0 Ondansetron 8. 39 Dolasetron 7. 3 Granisetron 8. 91 Granisetron 9. 0 Dolasetron 7. 60 Tropisetron 8. 70 > Plasma t½ of palonosetron is ~4 -10 times longer than granisetron or ondansetron > > > In particular, palonosetron is: 30 -fold more potent than granisetron 100 -fold more potent than ondansetron 1. Constenla M. Ann Pharmacother 2004; 38: 1683. 2. Grunberg, SM and Koeller, JM. Exp Opin Pharmacotherapy (2003); 4 (12): 2297 -2303; 3. Siddiqui, MAA an Scott, LJ. Drugs (2004); 64 (10): 1125 -1132; 4. Tonini, G, Vincenzi, B and Santini, D. Exp Opin Drug Metab Toxicology (2005); 1 (1): 143 -149.
types of Antiemetic therapies Serotonin (5 -HT 3)Receptor Antagonists Side effects headache- 40%– constipation 3 -20% slows bowel movements Dizziness 10 -40 % Equaly effective in PO and iv administration
types of Antiemetic therapies NK 1 RECEPTOR ANTAGONISTS : MOA: Displacing substance P from its receptor and by that blocks the signal to emesis Reduce acute and delayed emesis For MEC and HEC Receptors for NK 1 are available in the CNS and in the GI track Oral aprepirant (EMEND) First agent approved Three days of oral therapy (D 1 -125, d 2 -3 80 mg)
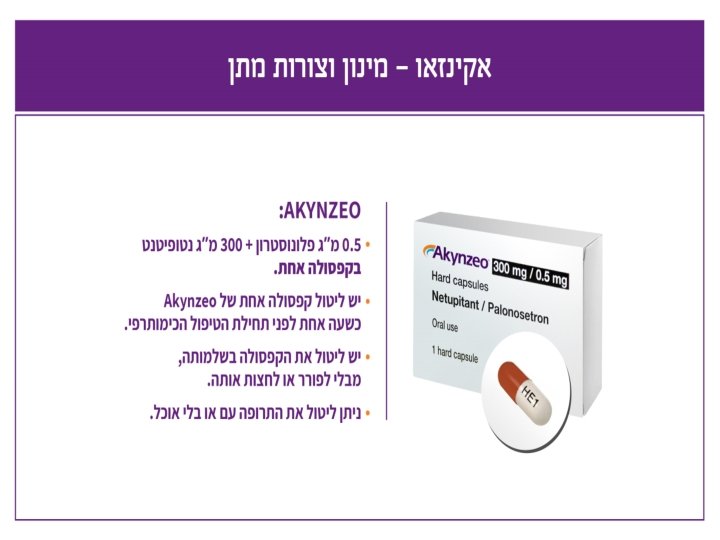
types of Antiemetic therapies NK 1 RECEPTOR ANTAGONISTS AKYNZEO First antiemetic combination agent developed Combination of highly selective NKI RA-netupitant and 5 ht 3 RA- palonesrtron. Approved for prevention of acute and delayed emesis in patients receiving HEC CT (+CARBOPLATIN AC) USA 2014 Approved for prevention of acute and delayed emesis in patients receiving MEC in selected patients with risk factors or who have failed previous therapy with 5 HT 3 RA + steroids.
Netupitant: Chemical structure and main features NETU 300 mg Aprepitant Half-life (h) 961 9 -132 Binding Affinity (p. Ki) 9. 03 high 2 90% Striatum Receptor Occupancy reached at Cmax YES 4 YES 2 Potent and selective NK 1 RA Competitively binds to and blocks activity of human substance P receptors which results in the prevention or alleviation of CINV High binding affinity, long half-life High and long-lasting (for up to 96 hours) brain receptor saturation after single oral dose NETU: netupitant; NK 1: neurokinin-1; RA: receptor antagonist ; PK: pharmacokinetics h: hours; p. Ki: the negative logarithm to base 10 of the equilibrium dissociation constant; Cmax: maximum plasma concentration * the first agent available in the NK 1 receptor antagonist drug class (Navari RM. Drugs. 2013; 73: 249– 262) 1. Lorusso V et al. Future Oncol. 2014 Oct 31: 1 -13; 2. Emend® (aprepitant) prescribing information, 2008; 3. Rizzi A et al. Peptides. 2012; 37: 86– 97; 4. Spinelli T et al. J Clin Pharmacol. 2014 Jan; 54(1): 97 -108.
types of Antiemetic therapies Benzodiazepines Lorazepam is a useful adjuvant because it decreases anxiety. Recommended for patients who are at risk for anticipatory N+V.
Drugs for treating nausea and vomiting Olnazpine -antipsycotic agent with high affinity for multiple dopamine (D 1, D 2, D 4), serotonin (5 HT 2 A, 5 HT 2 C, 5 HT 3), α 1 -adrenergic, H 1, and cholinergic (M 1– 5) receptors Dose: 5– 10 mg/day by mouth with lower starting dose 2. 5 mg Side effects: somnolence and weight gain. Dry mouth, constipation, increased appetite, agitation
BREAKTHROUGH CINV refractory N+V is challenging to reserve- preventing is the best method Routine around the clock administration of antiemetic Give additional agent from a different drug class Use several agent with a different MOA-(eg corticosteroids, olanzapine, haloperidol; lorazepam, metoclopramide) IV route is often required Adequate hydration should be ensured Electrolytes abnormalities should be assessed and corrected
BREAKTHROUGH CINV Assessment before administering the next cycle of CT Assessment for other possible non CT related reasons Use antacid therapy (H 2 BLOCKERS )with steroids
Classes of Antiemetic Agents and Their Primary Roles in the Prevention and Treatment of CINV Class (Drugs) Target /MOA 5 -HT 3 receptor antagonists Blocks binding of serotonin (dolasetron/ondansetron/granisetron/palonosetr on) Primary Role in CINV Acute CINV (day 1) Delayed CINV (days 2 -5): palonosetron only NK 1 receptor antagonists (aprepitant/fosaprepitant) Blocks binding of substance Delayed P Dopamine antagonists • Phenothiazines (prochlorperazineb) • Substituted benzamides (eg, metoclopramidea) • Butyrophenones (eg, haloperidola) Blocks binding of dopamine Breakthrough Corticosteroids (eg, dexamethasone) Unknown Acutea and delayeda Benzodiazepines (eg, lorazepam) Unknown Anticipatorya, breakthrougha Thienobenzodiazepine (eg, olanzapine) Targets multiple receptors including dopamine and serotonin Acutea, delayeda, breakthrougha
Antiemetic guidlines Several international organizations have developed evidence-based antiemetic guidelines that reflect the accumulating experience with the regimens. The guidelines include a rating system for CT based on intrinsic emetogenicity The recommendations for prophylactic treatment include drug doses.
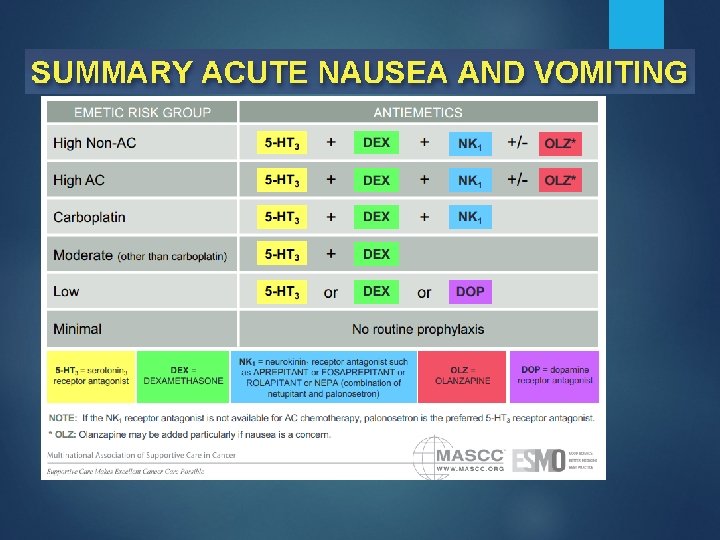
Recommended Doses of Serotonin Receptor (5 -HT 3) Antagonists for Acute Emesis AGENT Ondansetron Granisetron Dolasetron Tropisetron Palonosetron ROUTE ANTIEMETICS IV 8 mg or 0. 15 mg/Kg 5 HT 3 Oral IV 5 HT 3 Oral PALO IV Oral + DEX + APR 16 mg* 1 mg or 0. 01 mg/Kg + DEX 2 mg + (or. APR 1 mg**) + DEX 100 mg*** 5 mg IV 0. 25 mg Oral 0. 5 mg * Randomized studies have tested the 8 mg twice daily schedule ** The 1 mg dose preferred by some panelists *** Oral dosing recommended rather than IV due to potential QT interval prolongation
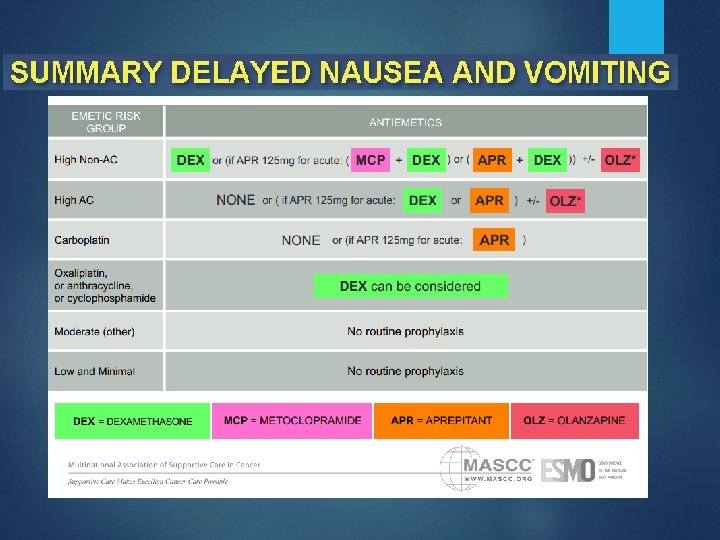
Recommended Corticosteroid* (dexamethasone) Dosing DEXAMETHASONE - Acute Emesis High Risk - Delayed Emesis - Acute Emesis Moderate Risk - Delayed Emesis Low Risk - Acute Emesis Dose and Schedule 20 mg once (12 mg when used with aprepitant or fosaprepitant)** 8 mg bid for 3 - 4 days (8 mg once daily when used with aprepitant or fosaprepitant) 8 mg once 8 mg daily for 2 - 3 days (many panelists give the dose as 4 mg bid) 4 - 8 mg once
Recommended NK 1 Receptor Antagonist Dosing*
Multiple-day CT CT that administered on consecutive days Prophylaxis is more complex Overlap between acute and delayed phase ANTIEMETIC THERAPY IS SELECTED BASED ON THE DRUG WITH THE HIGEST EMETIC RISK Repeated dose of Paloxi is possible if needed
Anti emetic protocols D 4 Dexamethasone 4 mg Dexamethasone 8 mg 5 כנ"ל יום To prevent hepatotoxicity D 3 Dexamethasone 8 mg Dexamethasone 8 mg Dexamethasone 6 mg Dexamethasone 8 mg Dexamethasone D 2 Dexamethasone 8 mg Dexamethasone 8 mg Dexamethasone 8 mg Dexamethasone D 1 Kytril 1 mg Dexamethasone 8 mg Tab. AKYNZEO Dexamethasone 12 mg Tab. AKYNZEO Dexamethasone 12 mg Kytril 1 mg Dexamethasone 8 mg Tab. AKYNZEO Dexamethasone 12 mg Dexamethasone 20 mg רמת אמטוגניות M פרוטוקול M FOLFIRI H FOLFIRINOX H VP CIS M VP CARBO H H CARBO AUC > 4 תלת שבועי FLOT H AC H VIDE H Cisplatin 20 -25 mg H Cisplatin > 30 mg M H Carbo Taxol ( )שבועי BEP M Yondelis FOLFOX
Thank you for your kind attention