Atherosclerosis CVS 1 Hisham Al Khalidi Atherosclerosis wmv














.")
 and smooth muscle cells (from the media)")




 Hemorrhage into a plaque, especially in the coronary arteries, may")
Superimposed thrombosis, the most feared complication, usually occurs on disrupted lesions")
Aneurysmal dilation may result from ATHinduced atrophy of the underlying media, with")
 Cerebral infarction (stroke) Aortic")

- Slides: 28
Atherosclerosis CVS 1 Hisham Al Khalidi
Atherosclerosis. wmv
Vessel wall structure
Atherosclerosis • A type of arteriosclerosis • Chronic inflammatory response in the walls of arteries • Slowly progressive • A build-up of fat (cholesterol) within the artery wall • Characterized by intimal lesions called: atheromas, atheromatous or fibrofatty plaques
Atherosclerosis Common sites • • • Abdominal aorta Coronaries Popliteal artery The internal carotid arteries The vessels of the circle of Willis
Atherosclerosis Risk factors
LDL Vs. HDL • LDL cholesterol : deliver cholesterol to peripheral tissues. • When too much LDL (bad) cholesterol circulates in the blood, it promotes atheroma formation in the arteries. LDLs contribute to heart disease because they carry large amounts of cholesterol.
LDL Vs. HDL • HDL, : is known as “good” cholesterol, because high levels of HDL seem to protect against heart attack. • it mobilizes cholesterol from developing and existing atheromas and transports it to the liver for excretion in the bile.
Atherosclerosis Contents • Important !
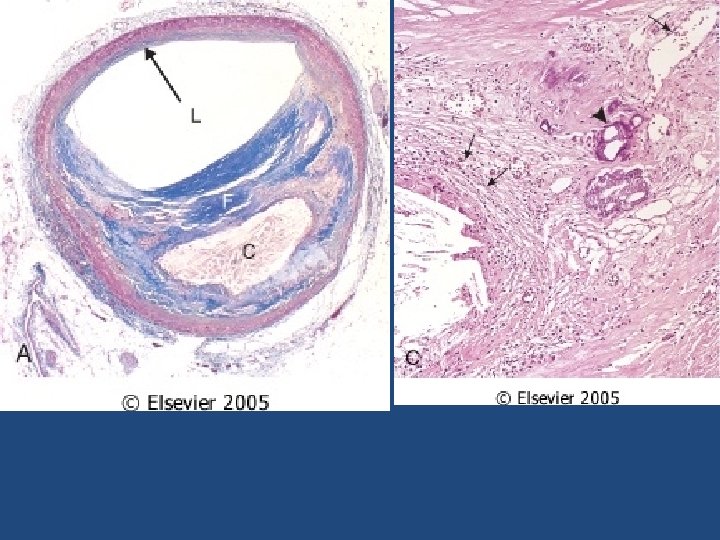
Atherosclerosis Pathogenesis • The main components of a fibrofatty plaques: – Lipids – Extracellular matrix – Cells, Proliferating smooth muscle cells
Atherosclerosis Pathogenesis response-to-injury hypothesis • Endothelial injury – Not completely understood – Nevertheless, the two most important causes of endothelial dysfunction are: • Hemodynamic disturbances • Hypercholesterolemia – Inflammation is also an important contributor. • Smooth muscle cell proliferation
Processes in the response to injury hypothesis. 1, Normal.
2, Endothelial injury with adhesion of monocytes and platelets (the latter to denuded endothelium).
3, Migration of monocytes (from the lumen) and smooth muscle cells (from the media) into the intima.
4, Smooth muscle cell proliferation in the intima.
5, Well-developed plaque.
Atherosclerosis Consequences
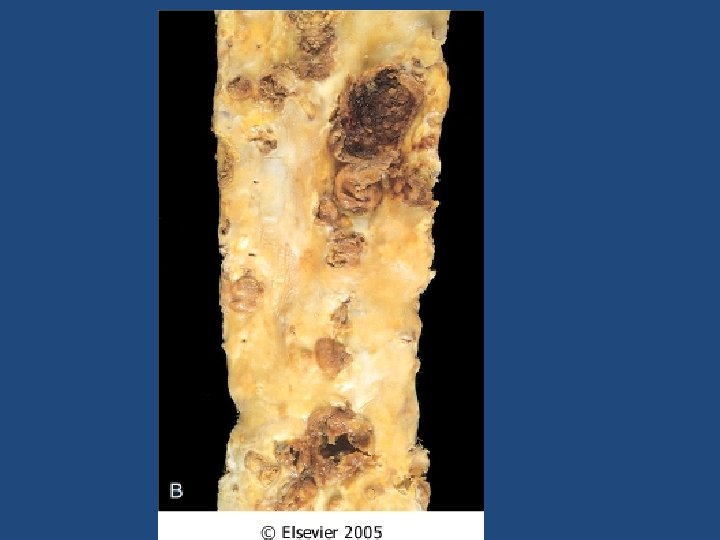
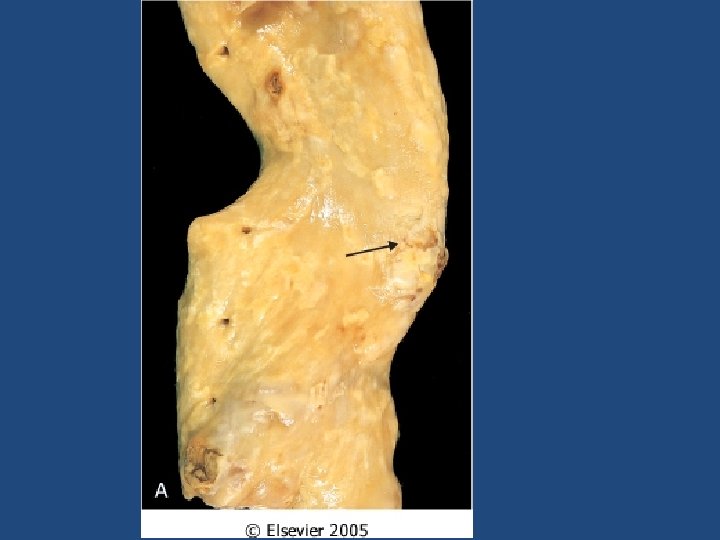
Atherosclerosis Complications The advanced lesion of atherosclerosis is at risk for the following pathological changes that have clinical significance: 1) Focal rupture, ulceration, or erosion of the luminal surface of atheromatous plaques may result in exposure of highly thrombogenic substances that induce thrombus formation or discharge of debris into the bloodstream, producing microemboli composed of lesion contents (cholesterol emboli or atheroemboli).
Atherosclerosis Complications • 2) Hemorrhage into a plaque, especially in the coronary arteries, may be initiated by rupture of either the overlying fibrous cap or the thinwalled capillaries that vascularize the plaque. A contained hematoma may expand the plaque or induce plaque rupture.
Atherosclerosis Complications • 3)Superimposed thrombosis, the most feared complication, usually occurs on disrupted lesions (those with rupture, ulceration, erosion, or hemorrhage) and may partially or completely occlude the lumen. Thrombi may heal and become incorporated into and thereby enlarge the intimal plaque.
Atherosclerosis Complications 4)Aneurysmal dilation may result from ATHinduced atrophy of the underlying media, with loss of elastic tissue, causing weakness and potential rupture 5) Calcifications.
Atherosclerosis Clinical Complications • • • Myocardial infarction (heart attack) Cerebral infarction (stroke) Aortic aneurysms Mesentric occlusion Peripheral vascular disease (gangrene of the legs)
Morphological changes that are seen on macro and microscopic levels in atherosclerosis • • • Calcification Hemorrhage Fissure Ulcer Thrombosis Neovascularization Medial thinning Cholesterol microemboli Aneurysmal dilatation