Atherosclerosis Dr Abhirami S MBBS Atherosclerosis Atherosclerosis is
")
Atherosclerosis Dr. Abhirami. S (MBBS)

Atherosclerosis • Atherosclerosis is a specific form of arteriosclerosis (thickening & hardening of arterial walls) affecting primarily the intima of large and medium-sized muscular arteries and is characterized by the presence of fibrofatty plaques or atheromas. • The term atherosclerosis is derived from athero (meaning porridge) referring to the soft lipid-rich material in the centre of atheroma, and sclerosis (scarring) referring to connective tissue in the plaques.

Atheroma l Definition Atheroma is the accumulation of intracellular and extracellular lipid in the intima of large and medium sized arteries

Atherosclerosis l Definition The thickening and hardening of arterial walls as a consequence of atheroma

Arteriosclerosis l Definition The thickening of the walls of arteries and arterioles usually as a result of hypertension or diabetes mellitus

Atheroma - Macroscopic Features Fatty streak l Simple plaque l Complicated plaque l




Atheroma - Common Sites Aorta - especially abdominal l Coronary arteries l Carotid arteries l Cerebral arteries l Leg arteries l

ATHEROSCLEROSIS Normal Intima Medis Adventitis Atherosclerosis Proliferation of intimal connective tissue Lipid accumulation Tissue breakdown Factors such as high plasma cholesterol, smoking, hypertension, diabetes and family history are all associated with atherosclerosis.

Progression Of Atherosclerosis

Pathology and pathogenesis • Fatty streaks are thin, flat yellow intimal discolorations that progressively enlarge by becoming thicker and slightly elevated as they grow in length. • They consist of macrophages and smooth muscle cells that have become distended with lipid to form foam cells. • These occurs regardless of geographic setting, gender, or race. • They increase in number until about age 20 years, and then they remain static or regress. • There is controversy about whether fatty streaks, in and of themselves, are precursors of atherosclerotic lesions.

Pathology and pathogenesis • The fibrous atheromatous plaque is the basic lesion of clinical atherosclerosis. • It is characterized by the accumulation of intracellular and extracellular lipids, proliferation of vascular smooth muscle cells, and formation of scar tissue. • The lesions begin as a elevated thickening of the vessel intima with a core of extracellular lipid (mainly cholesterol, which usually is complexed to proteins) covered by a fibrous cap of connective tissue and smooth muscle. • As the lesions increase in size, they encroach on the lumen of the artery and eventually may occlude the vessel or predispose to thrombus formation, causing a reduction of blood flow.

Pathology and pathogenesis • The more advanced complicated lesions are characterized by – Hemorrhage – Ulceration – Scar tissue deposits • Thrombosis is the most important complication of atherosclerosis. • It is caused by slowing and turbulence of blood flow in the region of the plaque and ulceration of the plaque.
 Major Constitutional risk factors: i. Age")
Risk Factors in Atherosclerosis Major risk factors 1) Major Constitutional risk factors: i. Age ii. Sex iii. Genetic factors iv. Familial and racial factors 2) Major Acquired risk factors: i. Hyperlipidaemia ii. Hypertension iii. Diabetes mellitus iv. Smoking v. Hyperhomocysteinemia

Multiple Risk Factors for Atherothrombosis Lifestyle • Smoking • Diet • Lack of exercise Generalized Disorders • Age • Obesity Genetic Traits • Gender • Pl. A 2 Atherothrombotic Manifestations (MI, stroke, vascular death) Inflammation • Elevated CRP • CD 40 Ligand, IL-6 • Prothrombotic factors (F I and II) • Fibrinogen Systemic Conditions • Hypertension • Hyperlipidemia • Diabetes • Hypercoagulable states • Homocysteinemia Local Factors • Blood flow patterns • Shear stress • Vessel diameter • Arterial wall structure • % arterial stenosis

Xantholesma

Xanthoma

Corneal Arcus

Clinical Manifestations • The clinical manifestations of atherosclerosis depend on the vessels involved and the extent of vessel obstruction. • Atherosclerotic lesions produce their effects through: – narrowing of the vessel and production of ischemia; – sudden vessel obstruction caused by plaque hemorrhage or rupture; – thrombosis and formation of emboli resulting from damage to the vessel endothelium; • In larger vessels such as the aorta, the important complications are those of thrombus formation and weakening of the vessel wall. • In medium-size arteries such as the coronary and cerebral arteries, ischemia and infarction caused by vessel occlusion are more common. • Although atherosclerosis can affect any organ or tissue, the arteries supplying the heart, brain, kidneys, lower extremities, and small intestine are most frequently involved.

Progression of Atherosclerosis 1. Endothelial Injury: Ø Initial triggering event in the development of Atherosclerotic lesions Ø Causes ascribed to endothelial injury in experimental animals include mechanical trauma, haemodynamic forces, immunological and chemical mechanisms, metabolic agents like chronic hyperlipidaemia, homocystine, circulating toxins from systemic infections, viruses, hypoxia, radiation, carbon monoxide and tobacco products. Ø In man, two major risk factors are haemodynamic stress from hypertension and chronic hyperlipidaemia.

Progression of Atherosclerosis 2. Intimal Smooth Muscle Cell Proliferation Ø Endothelial injury causes adherence aggregation and platelet release reaction at the site of exposed subendothelial connective tissue. Ø Proliferation of intimal smooth muscle cells is stimulated by various mitogens released from platelets adherent at the site of endothelial injury. Ø These mitogens include PDGF, fibroblast growth factor, TGF-ά. Ø Proliferation is also facilitated by nitric oxide and endothelin released from endothelial cells.

Progression of Atherosclerosis 3. Role of Blood Monocytes Ø Though blood monocytes do not possess receptors for normal LDL, LDL does appear in the monocyte cytoplasm to form foam cell. Ø Plasma LDL on entry into the intima undergoes oxidation. Oxidised LDL formed in the intima performs following two important functions : Ø For monocytes, oxidized LDL acts to attract, proliferate, immobilise and activate them and is readily taken up by scavenger receptor on the monocyte to transform it to a lipid laden foam cell. Ø For endothelin, oxidized LDL is cytotoxic.

Progression of Atherosclerosis 4. Role of Hyperlipidaemia ØChronic hyperlipdaemia in itself may initiate endothelial injury and dysfunction by casing increased permeability. ØIncreased serum concentration of LDL and VLDL promotes formation of foam cells, while high serum concentration of HDL has anti-atherogenic effect.

Progression of Atherosclerosis 5. Thrombosis Ø Endothelial injury exposes sub-endothelial connective tissue resulting in platelet aggregation at the site besides proliferation of smooth muscle cells. Ø This causes mild inflammatory reaction which together with foam cells is incorporated into atheromatous plaque. Ø Lesions enlarge by attaching fibrin and blood cells causing thrombus formation which becomes a part of atheromatous plaque.

Atheroma - Common Sites Aorta - especially abdominal l Coronary arteries l Carotid arteries l Cerebral arteries l Leg arteries l

Atherosclerosis: A Progressive Process Normal Fatty Streak Plaque Occlusive Rupture/ Fibrous. Atherosclerotic Fissure & Plaque Thrombosis Unstable Angina MI Effort Angina Claudication Clinically Silent Increasing Age Courtesy of P Ganz. Coronary Death Stroke Critical Leg Ischemia

Atheroma - Coronary Artery


Atheroma - Clinical Effects l Ischaemic heart disease sudden death l myocardial infarction l angina pectoris l arrhythmias l cardiac failure l

Atheroma – myocardial infarction

Atheroma – myocardial infarction

Multiple Complex Coronary Plaques in Patients With Acute MI Multiple plaques detected Culprit lesion
")
Atheroma - Clinical Effects l Cerebral ischaemia transient ischaemic attack l cerebral infarction (stroke) l multi-infarct dementia l

Atheroma – cerebral infarction

Atheroma - Clinical Effects l Mesenteric ischaemia ischaemic colitis l malabsorption l intestinal infarction l

Atheroma – intestinal infarction


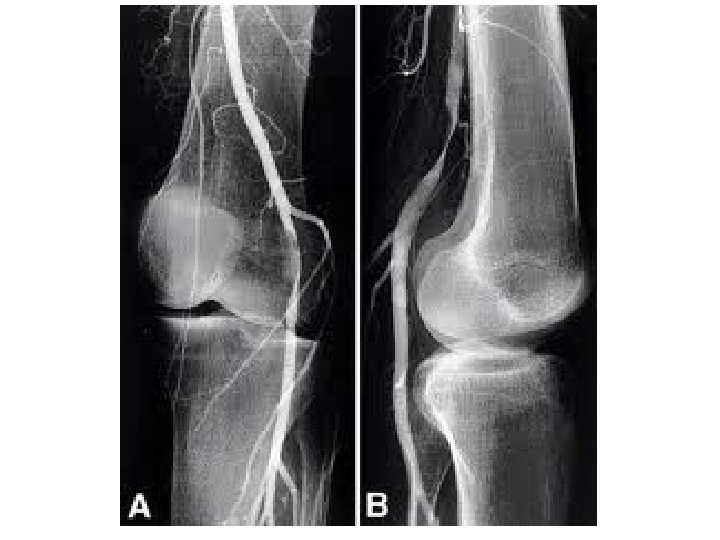
Atheroma - Clinical Effects l Peripheral vascular disease intermittent claudication l Leriche syndrome l ischaemic rest pain l gangrene l

Atheroma – peripheral vascular disease


- Slides: 47