Acute Coronary Syndrome Nicholas Shaw ACS STEMI New




















 • Antiplatelets – aspirin (300 mg)")
 Clopidogrel (or ticagrelor) Beta blockers")

- Slides: 26
Acute Coronary Syndrome Nicholas Shaw
ACS • STEMI – New onset LBBB • NSTEMI • Unstable angina
Risk Factors for ACS • • Smoking Obesity Dyslipidaemia Hypertension • • • Age Male Ethnicity Family history CKD
Stable Angina • Cardiac chest pain precipitated by exercise • Caused by atheroma, but also: anaemia, AS, tachyarrhythmias, HOCM • Eases with rest / GTN • 4 classes: – – I: angina on strenuous exercise II: Slight limitation of ordinary activities III: difficulty climbing stairs IV: unable to carry out any physical activity • Risk of progression to ACS (1% non-fatal MI/year)
Angina investigations • • • ECG Ecercise ECG FBC – anaemia Glucose – diabetes Lipids – dyslipidaemia TFTs - thyrotoxicosis
Angina Management • Lifestyle modification • Modifying risk factors • Medication – Aspirin – Beta blockers – Calcium channel blockers – Statins – Nitrates • Surgical – PTCA, CABG
Unstable Angina • Presence of angina without precipitating cause / at rest • Spectrum with stable angina and NSTEMI
Presentation of ACS • Typical chest pain – Male – Left sided chest pain – Radiating to left arm – Radiating to neck • Atypical chest pain – – – Right sided chest pain Abdominal pain Female Diabetic Elderly Silent MI • • • Cool Clammy Nausea Dyspnoea Pulmonary oedema Confusion Palpitations Collapse Death
Differential Diagnosis • • Musculoskeletal chest pain Pulmonary embolus Aortic dissection Gastric reflux
Diagnostic criteria of acute MI • 2/3 of: – ECG changes – Chest pain – Rise in cardiac enzymes
Investigations • ECG • Bloods – FBC – U&E – Trop T • CXR – Cardiomegaly – Pulmonary oedema – Widened mediastinum
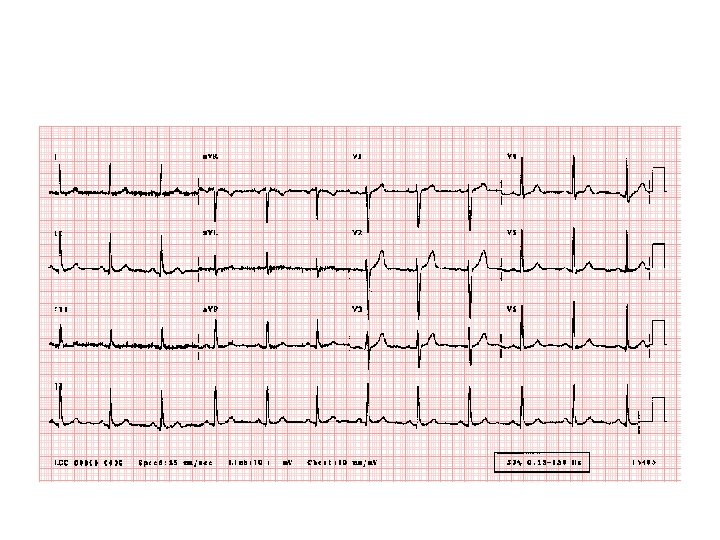
NSTEMI • Subocclusive thrombus • ECG changes: – ST depression – T wave inversion
NSTEMI
ECG Leads High lateral Septal Inferior Lateral Anterior
Arteries Affected Location of MI Artery Lateral Anterior Septum Inferior Posterior Right Ventricle Left circumflex LAD RCA RCA
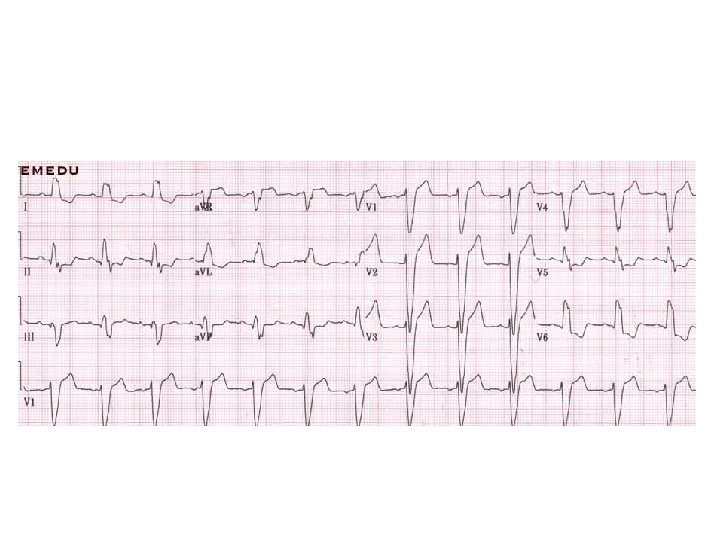
• Anterior MI • • • ST elevation is maximal in the anteroseptal leads (V 1 -4). Q waves are present in the septal leads (V 1 -2). There is also some subtle STE in I, a. VL and V 5, with reciprocal ST depression in lead III. There are hyperacute (peaked ) T waves in V 2 -4. These features indicate a hyperacute anteroseptal STEMI
• Tombstoning
• Posterior MI
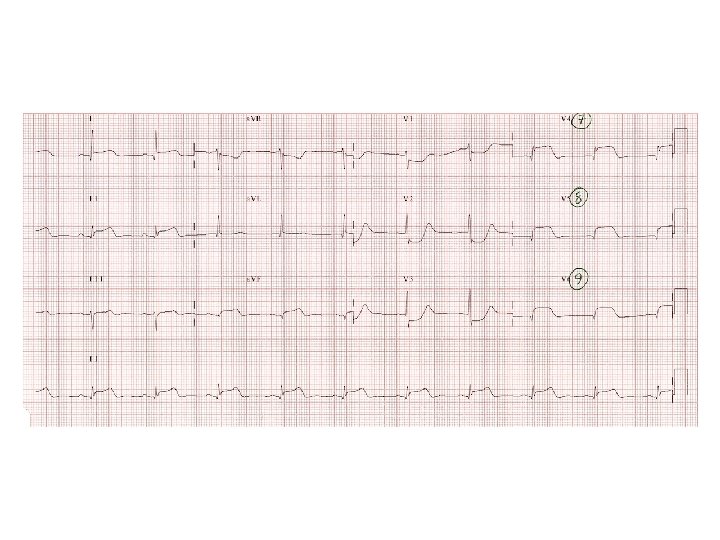
• Inferior MI
STEMI • - ST elevation > 1 mm in two or more limb leads and/or • - ST elevation > 2 mm in two or more consecutive precordial leads and/or • - Left Bundle Branch Block (LBBB) which is known or suspected to be of new onset and in the presence of cardiac symptoms
Treatment of STEMI • Morphine • Antiemetics (metoclopramide) • Antiplatelets – aspirin (300 mg) and ticagrelor (180 mg) • IV access • Bloods • Primary Coronary Intervention • Thrombolysis (t. PA / streptokinase)
Further inpatient management • • Education Echocardiogram (LV function) Clopidogrel (or ticagrelor) Beta blockers ACE-I Statins Risk factor modification
Late Complications • • • Dresslers syndrome Papillary muscle rupture Fibrosis Aneurysm Heart failure Death