The Future of Dentistry What is the ADAs


















 • • • Support financially (grants, scholarships) Creative Financing to")





 such")






- Slides: 35
The Future of Dentistry What is the ADA’s vision?
Mission • Guard the oral health of the public • Role: ▫ Improvement of the health of the public ▫ Promoting the art and science of dentistry
Vision statement • Improved health and quality of life for all through optimal oral health ▫ Socially responsible and culturally competent manner of improving health ▫ Commitment to the adoption of science-based practices ▫ Strong educational system ▫ Aggressive approach to health promotion, disease prevention, and access to care ▫ Closer collaboration among health professions ▫ Develop a global perspective and action plan to fulfill its responsibility as a world community
Oral Health Partnerships Recommendation #1 • Establish and support partnerships and alliances among dental, other healthcare professional, and public health organizations, as well as business and social service groups in order to improve oral health
Oral Health Promotion Recommendation #2 • Aggressively address the oral health needs of the public ▫ ▫ ▫ Water fluoridation and sealant programs Oral cancer prevention Special needs populations Oral and general health linkages Financing and reimbursement programs for oral health services for low-income and special needs ▫ Database development to predict oral health needs
Research and Education Capabilities Recommendation #3 • Strengthen and expand dentistry’s research and education capabilities ▫ Augment resources for research and education ▫ Enhance visibility of dental schools at academic health centers ▫ Strengthen interaction between research and education ▫ Develop new approaches to transfer of emerging scientific knowledge
Dental Workforce Recommendation #4 • Ensure development of a responsive, competent, diverse, and ‘elastic’ workforce ▫ Recruit and retain individuals in the profession ▫ Address the distribution and mobility of the dental workforce ▫ Increase availability and use of allied dental personnel, under appropriate supervision by dentists ▫ Establish and expand efforts to recruit and maintain dental research and education workforce
Financial Resources Recommendation #5 • Address fiscal needs of the practice, education and research sectors
Financial Resources Recommendation #6 • Formal Organization with ADA, ADEA, NIDCR and AADR
Financial Resources Recommendation #7 • Development of highly targeted, collaborative marketing and public relations initiatives
Access to care recommendations • Public funding should be expanded to provide resources that would cover basic dental services for the long-term unemployed • New programs should be developed in which individual employees could purchase insurance plans directly from risk pools if their employers don’t provide it
Access to care recommendations • Effective incentives should be offered to attract dentists to underserved • National Health Service Corps should be expanded to provide dental care in underserved areas • Publicly funded or subsidized dental program should be developed for people with disabilities
Access to care recommendations • Outreach programs at state and local levels should be developed to meet the needs of patients unable to receive dental care in traditional dental offices • Tax-deferred dental/medical savings accounts should be established in which the balances accrue over time and can be used by the elderly as needed during their retirement
Licensure and Regulation Recommendations • National board exams, regional clinical exams should evolve to reflect the change in dental disease patterns and clinical practice patterns
Licensure and Regulation Recommendations • Dental profession should support a study to address the issues of continuing competency • The profession should strive for approaches aimed at evaluating the clinical competency of a dental practitioner by simulated methods or post -treatment case review
Licensure and Regulation Recommendations • The profession should maintain the role of dentists as the ultimate authority for the diagnosis of, treatment planning for, and delivery of care for oral disease • Dental profession should establish unity of all examining bodies
Licensure and Regulation Recommendations • Encourage all licensing boards to develop guidelines and procedures that allow for the exam of educationally-qualified specialists in their areas without requiring concurrent examination for a general dentistry license • Intensify efforts to achieve licensure by credentials in all states
Licensure and Regulation Recommendations • Continue to be vigilant and proactive in identifying and researching potential hazards that might impact the safety of patients, the dental workforce and environment • Remain proactive in advocating scientifically valid solutions to identified hazards • Division of Governmental Affairs and Constituent Dental Societies must remain vigilant and vigorous ensuring the voice of dentistry is heeded in regulatory discussions
Educational Recommendations (30 total) • • • Support financially (grants, scholarships) Creative Financing to build relationships Counseling for debt management after school Fundraising for alma maters Regionalization to collaborate (electronic distance learning) • New technology and scientific advances • Discuss educational expansion with local community and stakeholders
Statement Release February 2011 • Breaking Down Barriers to Oral Health for All Americans: The Role of the Workforce • To sum it up: we need to come together and quite using statistics to back our own agendas ▫ We got in to this profession because we wanted to help people. Let’s work together to make it happen
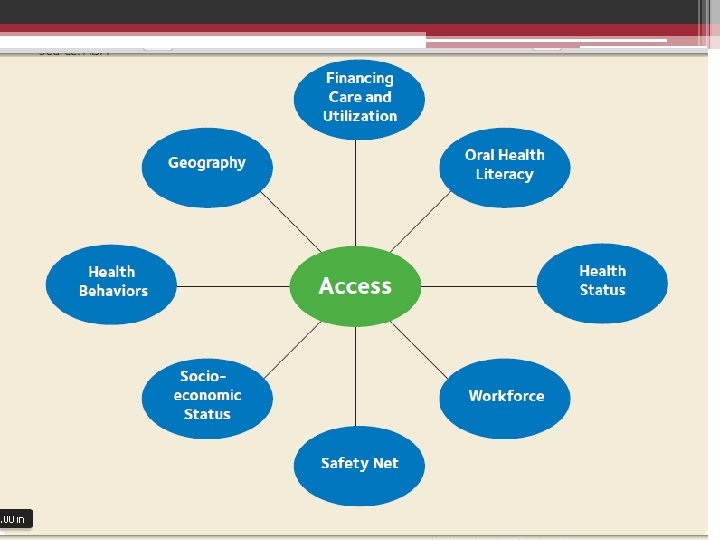
Solving access to care • Not a single fix issue • Multi-faceted approach to fix the issue ▫ Workforce is just one part of the problem – not so much a lack of workers, but an unequal distribution of them • Language barriers and cultural barriers are also a part of it • Education (or lack of it) in the public about oral health and the workforce is also a problem
Community Dental Health Coordinator • The ADA proposed the CDHC to come from their own community where they will return and work • Based on ADA’s key principles: ▫ Education ▫ Disease prevention ▫ Maximizing the existing system
CDHC training • Recruited from the same communities that have access to care problems ▫ Limited English proficiency ▫ Poverty areas ▫ Lack of awareness about basic oral hygiene • 18 month training program • 12 month didactic + 6 month internship ▫ All didactic done online through Rio Salado College �In person training session throughout to test students’ skill levels
ADA says NOT a mid-level provider • It is not a mid-level provider because they are not asked to drill and fill • They will: ▫ ▫ ▫ Screen Fluoride Sealants Temp fillings “Simple” teeth cleanings
“Simple cleanings” defined • “(for example, selective scaling for periodontal type I (gingivitis) such as removing gross debris, stains and calculus using anterior and posterior hand scalers until the patient can receive treatment from a dentist or hygienist)”
Not CODA approved nor standards developed • Commission on Dental Accreditation is part of the ADA, but there are not standards yet…. . • They will work under direct supervision or REMOTE supervision of a dentist ▫ ▫ ▫ Head Start programs Clinics Schools Churches Senior Citizen Centers
ADA opposes other models • The ADA opposes the other models of providers because they are able to perform ‘surgery and irreversible’ procedures • ADA policy emphasizes the dentist’s role as the leader of the dental team who performs examinations, diagnoses, treatment planning and surgical/irreversible procedures that are defined as the cutting or removal of hard or soft tissue • “If your only tool is a hammer, every problem looks like a nail, ” (ADA, 2011) speaking against the Dental Therapist, ADHP, and DHAT (Alaska model)
ADA: “Breaking Down Barriers” conclusion • “Expending precious resources on workforce experiments that ignore the experience and inarguable success of the existing delivery system would be a costly trip down the wrong road. ”
How does the ADA compare? A national call to action ADA • Change perceptions of oral health • Overcome barriers by replicating effective programs • Build the science base and accelerate science transfer • Increase Oral Health Workforce Diversity, Capacity, and Flexibility • Increase Collaborations • Oral health partnerships • Oral health promotion • Research and education capabilities • Dental workforce • Financial resources • Collaborations between dental practice, research and education • Collaborative marketing and public relations
What about ADA and ADHA? ADA ADHA • Oral health partnerships • Oral health promotion • Research and education capabilities • Dental workforce • Financial resources • Collaborations between dental practice, research and education • Collaborative marketing and public relations • • • Research Education Practice and Technology Licensure and Regulation Public Health Government
So… • If ADA and ADHA have some of the same overarching goals…. Could we (educational institutions, new students) be the catalyst to start the conversation? Or has the war gone on too long?