The critical role and criteria in diagnostic measurements






, fluoroscopy • Image bone, limited soft tissue •")


 • Describe anatomy in position when imaged postural •")







 translation")





(ed) ligaments • Kowalski HM, Cohen WA, Cooper P, Wisoff")
 MRI")


 of the intervertebral angulations and translations")

















- Slides: 46
The critical role and criteria in diagnostic measurements when connective tissue is weak Myles Koby DDS MD
EDS • Affects entire body • High levels of associated pain • Ligamentous laxity • Failure under “normal” loading • Muscles activity • Abnormal motion – position – posture - function
Why Image • Confirm clinical diagnosis • Define extent of problem • Exclude other conditions • Numeric value / objective criteria • Repeatable • Follow condition/ progression • Assess therapy
Why image • Imaging heralded medical and surgical advances last 50 years • High speed film changers • Angiography -- blood vessels • Contrast agents • CAT scans • MRI • Facilitates early therapy • Permit observation/ conservative therapy over emergent surgery
Neuroimaging • Impingement cervical medullary junction • Abnormal alignment • anterolistheisis, retrolistheisis • Abnormal motion • Bone deformity
Imaging Methods • X-ray films (radiographs), fluoroscopy • Image bone, limited soft tissue • CAT scan computed tomography • Image bone, soft tissue evaluation fair to good • MRI • Soft tissue display good to excellent, • bones not directly imaged, (inferred by soft tissue)
Position and motion measurements • Six degrees for freedom • Complex motion • Front to back/ anterolisthiesis • Lateral side to side / roll • Pitch /angulation • Yaw /rotation
Cranio-cervical Junction (Skull base spine) • Describe anatomy in position when imaged postural • Bones • Clival axial angle • Grabb-Oakes measurement • Harris measurements • (horizontal, vertical)
Measurements at the Cranio-Cervical Junction Clival axial angle • Normal range 150 -170 degrees
• Henderson FC, Wilson WA, Mott S, Mark A, Schmidt K, Berry JK, et al. Deformative stress associated with an abnormal clivo-axial angle: A finite element analysis. Surg Neurol Int. 2010; 1: 30 • Smoker WR. Craniovertebral junction: Normal anatomy, craniometry, and congenital anomalies. Radiographics. 1994; 14: 255– 77 • Lee BCP, Deck MDF, Kneeland JB, Cahill PT MR imaging of the craniocervical junction. AJNR 1985; 6: 209 -213
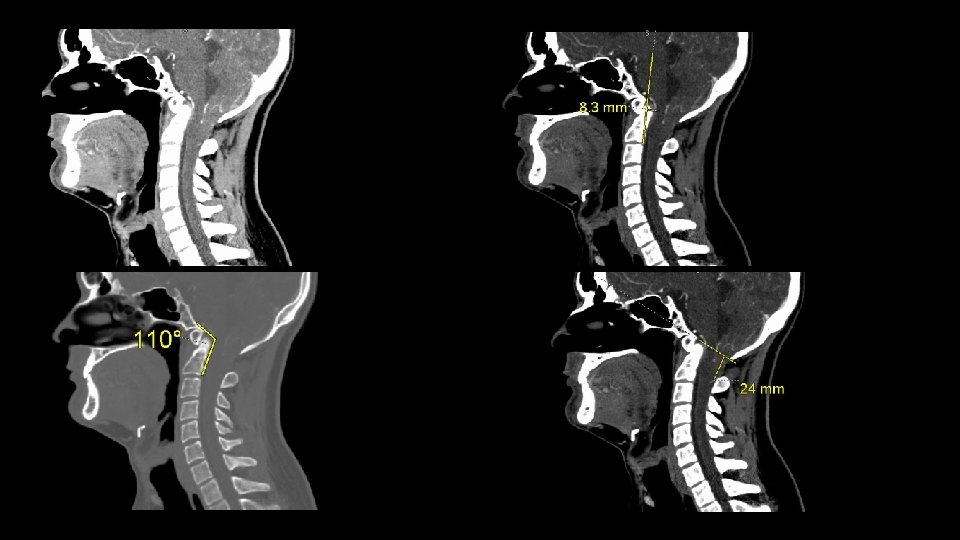
Grabb-Mapstone-Oakes measurement
Grabb-Mapstone -Oakes measurement 0. 7 cm or less normal Greater than 0. 9 cm suggests utility of anterior correction prior to posterior decompression (and stabilization) Recognized following Chiari decompression without correction of anterior impingement (stabilization)
Syrinx
• Grabb PA, Mapstone TB, Oakes WJ. Ventral brain stem compression in pediatric and young adult patients with Chiari I malformations. Neurosurgery. 1999; 44: 520– 7 ; discussion 527 -8 • Heiss JD, Suffredini G, Smith R, De. Vroom HL, Patronas NJ, Butman JA, et al. Pathophysiology of persistent syringomyelia after decompressive craniocervical surgery. Clinical article. J Neurosurg Spine. 2010; 13: 729– 742.
Harris horizontal measurement • • Basion-axis interval Relationship of skull base - C 1 Anterior-posterior (Front to back) Brainstem / spinal cord stress
Harris measurement measures distraction and (pathological) translation
• Harris measurement 1. 2 cm or greater implies ligamentous failure More than 0. 1 cm difference flexion -> extension abnormal • Rojas : normal is 0. 85 cm or less
Harris JR, Carson GC, Wagner LK. Radiographic diagnosis of traumatic occipitovertebral dissociation: Normal occipitovertebral relationships on lateral radiographs of supine subjects. AJR Am J Roentgenol. 1994; 162: 881– 6 Harris JH, Jr, Carson GC, Wagner LK, Kerr N. Radiologic diagnosis of traumatic occipitovertebral dissociation: 2: Comparison of three methods of detecting occipitovertebral relationships on lateral radiographs of supine subjects. AJR Am J Roentgenol. 1994; 162: 887– 92 Rojas CA, Bertozzi JC, Martinez CR, Whitlow J (2007) Reassessment of the craniocervical junction: normal values on CT. AJNR 28: 1819– 1823
Cervical spine • C 1 -C 2 Atlas axis • Rotation ~50% of total @ C 1 -C 2 • Measurements -> ligamentous failure -> instability
Rotation C 1 -C 2 • Normal 37 degrees or less • Indirect evaluation ligament function • 41 -44 pathologic instability • Pain • • • Nerve Blood vessels Ligaments Muscles Bone
Atlantoaxial instablity due to fail(ing)(ed) ligaments • Kowalski HM, Cohen WA, Cooper P, Wisoff JH. Pitfalls in the CT diagnosis of atlantoaxial rotary subluxation. AJR Am J Roentgenol 1987; 149: 595 -600. • White, A. A. ; Panjabi, M. M. The basic kinematics of the human spine: A review of past and current knowledge. Spine 3: 12– 20, 1978. • Muniz AE, Belfer RA. Atlantoaxial rotary subluxation in children. Pediatr Emerg Care 1999; 15: 25 -29 • Phillips WA, Hensinger RN. The management of rotatory atlanto-axial subluxation in children. J Bone Joint Surg Am 1989; 71: 664 -668. • Crook TB, Eynon CA. Traumatic atlantoaxial rotatory subluxation. Emerg Med J. 2005; 22: 671– 2.
Cervical spine flexion extension (bending) MRI
Segmental instability
The average motion between flexion and extension is 13° per level, with a range of 8 to 17°the average motion between flexion and extension is 13° per level, with a range of 8 to 17°tion between flexion and extension is 13° per level, with a range of 8 to 17° White, A. A. ; Panjabi, M. M. The basic kinematics of the human spine: A review of past and current knowledge. Spine 3: 12– 20, 1978.
Historical comparison of reported mean values (standard deviation) of the intervertebral angulations and translations for cervical flexion and extension at each spinal level Intervertebral C 2/3 Level movement C 3/4 Level C 4/5 Level C 5/6 Level C 6/7 Level Angulation (degrees) Bhalla and Simmons 9 (1) 15 (2) 23 (1) 19 (1) 18 (3) 12 18 20 20 15 Dvorak et al. 12. 0(3. 0) 17. 2 (3. 9) 21. 1 (3. 5) 22. 6 (4. 2) 21. 4 (3. 7) Panjabi et al. 6. 2 (2. 3) 7. 7 (5. 0) 10. 1 (4. 9) 9. 9 (4. 8) 7. 1 (4. 0) Frobin et al. 8. 4 (3. 4) 15. 2 (4. 7) 17. 0 (5. 5) 17. 9 (6. 6) 11. 4 (6. 8) 9. 9 (4) 15. 2 (3) 16. 9 (4) 15. 8 (4) 13. 5 (5) 13. 5 (4. 8) 17. 3 (7. 4) 22. 6 (7. 9) 19. 1 (6. 6) 18. 0 (9. 1) Frobin et al. 1. 00 1. 72 1. 89 1. 21 0. 30 Reitman et al. 1. 73 2. 26 2. 41 1. 86 0. 99 Pickett et al. 1. 56 2. 16 2. 45 2. 05 1. 14 1. 4 (0. 3) 2. 1 (0. 5) 2. 5 (0. 6) 2. 2 (0. 6) 1. 3 (1. 0) Penning Reitman et al. Wu et al. Translation (mm) Wu et al.
Instability cervical spine • 20 degrees or greater • 0. 35 cm motion • Symptomatic
Anterolistheisis • Greater than 0. 3 cm abnormal
Anterolistheisis • Greater than 0. 3 cm abnormal
Motion total 0. 53 cm @ C 5 -C 6
Total 25. 5 degrees @ C 5 -C 6
Instability C 4 -C 5
Instability C 4 -C 5
Motion Instability 29 degrees motion Dystonia pain ? post traumatic?
Reitman CA, Mauro KM, Nguyen L, Ziegler JM, Hipp JA. Intervertebral motion between flexion and extension in asymptomatic individuals. Spine. 2004; 29: 2832– 2843 Anderst WJ, Donaldson WF 3 rd, Lee JY, Kang JD. Continuous cervical spine kinematics during in vivo dynamic flexion-extension Spine J. 2014 Jul 1; 14(7): 1221 -7. Pickett GE, Rouleau JP, Duggal N. Kinematic analysis of the cervical spine following implantation of an artificial cervical disc. Spine. 2005; 30: 1949– 1954. Dvorak J, Froehlich D, Penning L, Baumgartner H, Panjabi MM. Functional radiographic diagnosis of the cervical spine: flexion/extension. Spine. 1998; 13: 748– 755. White, A. A. ; Panjabi, M. M. The basic kinematics of the human spine: A review of past and current knowledge. Spine 3: 12– 20, 1978.
Wu SK, Lan HC, Kuo LC, Tsai SW, Chen CL, Su FC. The quantitative measurements of the intervertebral angulation and translation during cervical flexion and extension. Eur Spine J. 2007 Sep; 16(9): 1435 -44. Epub 2007 Apr 27. Axelsson P, Karlsson BS. Intervertebral mobility in the progressive degenerative process. A radiostereometric analysis. Eur Spine J. 2004; 13: 567– 572. Bhalla SK, Simmons EH. Normal ranges of intervertebral joint motion of the cervical spine. Can J Surg. 1969; 12: 181– 187. Penning L. Normal movements of the cervical spine. Am J Roentgenol. 1978; 130: 317– 326. Dvorak J, Froehlich D, Penning L, Baumgartner H, Panjabi MM. Functional radiographic diagnosis of the cervical spine: flexion/extension. Spine. 1998; 13: 748– 755. Panjabi MM, White AA, John RM. Cervical spine mechanics as function of transaction of components. J Biomech. 1975; 8: 327– 336. Frobin W, Leivseth G, Biggemann M, Brinckmann P. Sagittal plane segmental motion of the cervical spine: a new precision measurement protocol and normal motion data of healthy adults. Clin Biomech. 2002; 17: 21– 31.
Limitations of studies • Method of evaluation • Imaging method • Technique • Passive vs active • Patient population • Live vs cadaver • Age, gender • Hypermobility in control not evaluated • Sample size
Limitations of studies • Trauma series • Rheumatoid arthritis • Down syndrome
Thank you
White, A. A. ; Panjabi, M. M. The basic kinematics of the human spine: A review of past and current knowledge. Spine 3: 12– 20, 1978 A. ; Panjabi, M. M. The basic kinematics of the human spine: A review of past and current knowledge. Spine 3: 12– 20, 1978
Kinematics of the Spine. In White AA, Panjabi MM, eds: Clinical Biomechanics of the Spine, 1990