MAHA diagnosis and management Kathryn Boyd Consultant haematologist

MAHA: diagnosis and management Kathryn Boyd Consultant haematologist April 2016

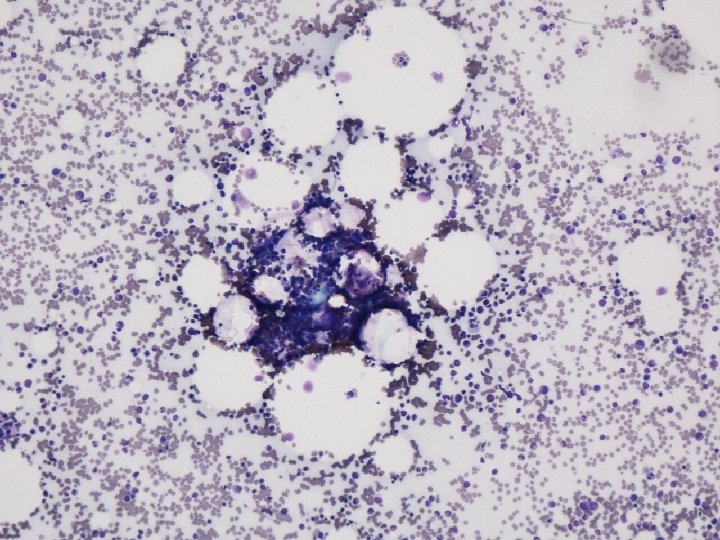
Photo blood film

Patient P: presentation on 18/01/2015 • LP, 47 yr old lady • Hb 98 g/l, WBC 4. 1, plat 21 x 10 9/l, , Retics 6%, • 2 days vomiting, nose bleed, dyspnoea, orthopnoea, leg swelling • PH: breast cancer in 2005, metastatic since 2010, last chemo 18 Nov 2014 gemcitabine and carboplatin • OE: Tachycardia, Pleural effusions, peripheral oedema, hypertension • Creatinine 301 mmol/l, e. GFR 14 ml/min, BNP 25 164

Photo blood film

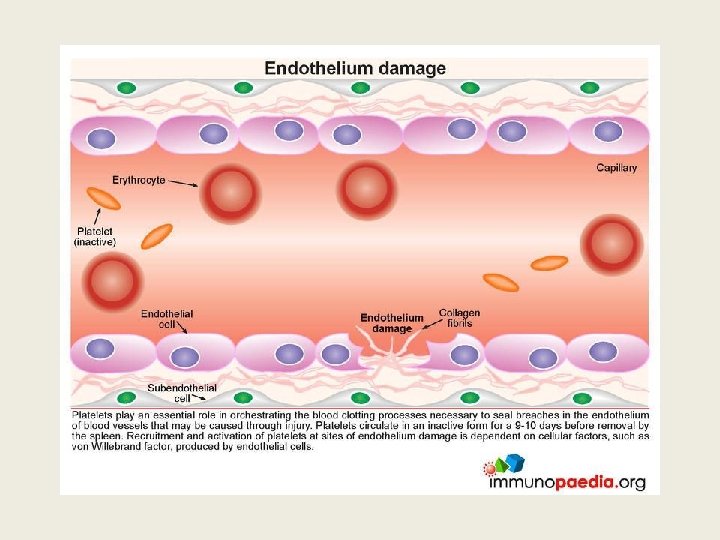
Schistocytes are evidence of fragmentation haemolysis Cardiac: prosthetic valves, patches, grafts, leaks around valves Arteriovenous malformations: Kasabach-Merritt syndrome, malignant haemangioendotheliomas Microangiopathy (MAHA): destruction of RBC’s in pathologically altered small blood vessels

MAHA: a clinical syndrome • Fragmentation haemolysis • main pathological lesions in microcirculation - deposition of fibrin strands often with DIC - platelet adherence and aggregation - vasculitis - tumour plugs in vessels • Vascular abnormalities may be generalized or confined to sites/organs
 • Thrombocytopenia • Clinical or")
Thrombotic Micro-angiopathies The Triad • Micro-angiopathic haemolytic anaemia (MAHA) • Thrombocytopenia • Clinical or histological effects of microvascular thrombosis Classification • Thrombotic thrombocytopenic purpura : TTP • Haemolytic Uremic syndrome: HUS • Atypical haemolytic uremic syndrome: a. HUS • Other Thrombotic microangiopathies: TMA’s DIC, HELLP, Systemic malignancies Autoimmune disorders Malignant hypertension Preeclampsia Systemic infection

Patient P: Why develop TMA ? Clinical history: • symptoms severe for 2 days but progressive over 3 months • metastatic breast cancer for 5 yrs • gemcitabine and carboplatin 3 mths ago Investigations: • Onset of uremia and cytopenias

Hb 120 100 80 60 Hb 40 20 0 Sept Oct Nov-02 Dec-01 Dec-02 Jan-12

Platelets 250 200 150 Platelets 100 50 0 Sept Oct Nov-02 Nov-11 Dec-01 Dec-12 Jan-01 Jan-12 Jan-18 Jan-20

Creatinine 500 450 400 350 300 250 Creatinine 200 150 100 50 0 Sept Nov Dec Jan-02 Jan-18 Jan-21 Jan-23

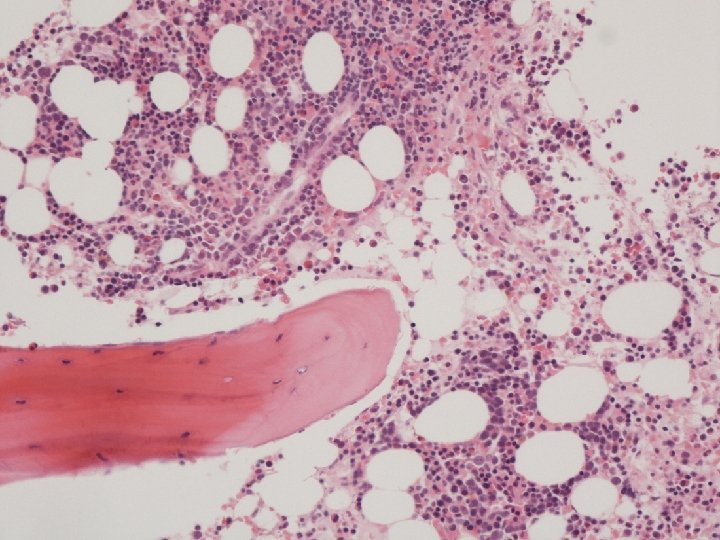
Further investigations LDH 1353 Haptoglobins absent DC negative PT 11, APTT 30, Fib 4. 4, D dimer 2. 2 Urine alb 1120 mg, creat 5. 36, ratio 209 CT pleural effusions, consolidation, ground glass shadows in lungs, patchy medullary pattern in rib cage, large liver with patchy left lobe • Bone marrow biopsy: Infiltrate? • • •

Bone marrow

Summary of Patient P: 47 yr old lady • 3 month history of progressive cytopenia and renal impairment since chemotherapy given 4 mth ago for metastatic breast cancer. • Presents with nose bleed and severe fluid overload causing heart failure. • Micro-angiopathic Haemolytic anaemia, Thrombocytopenia and renal failure • Conclusion: TMA • What type: TTP, a HUS, TMA Assoc with Cancer or chemo

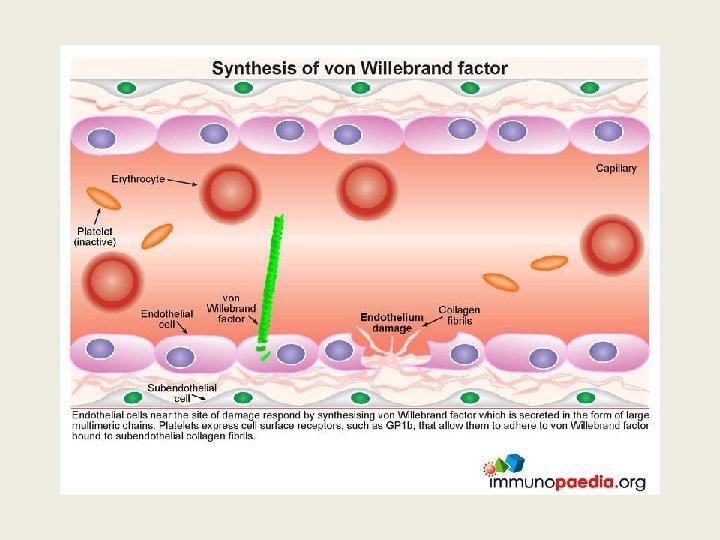
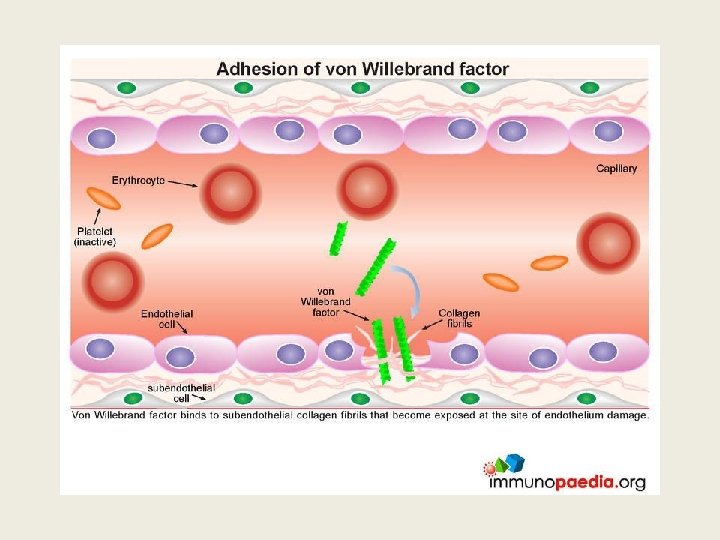
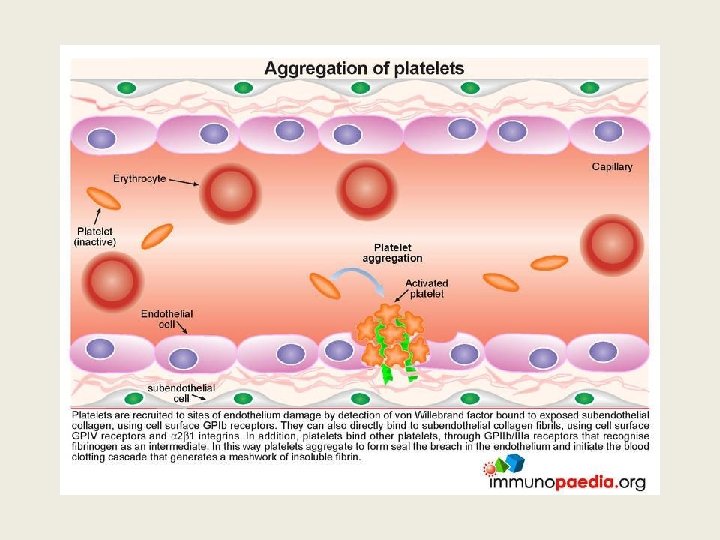
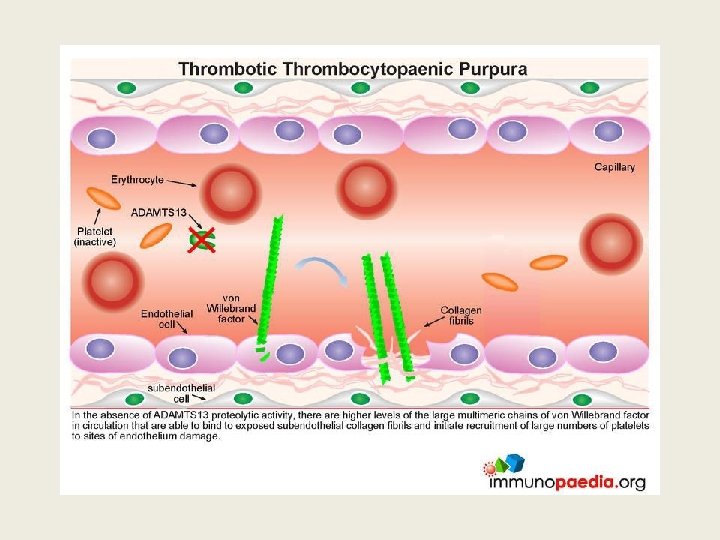
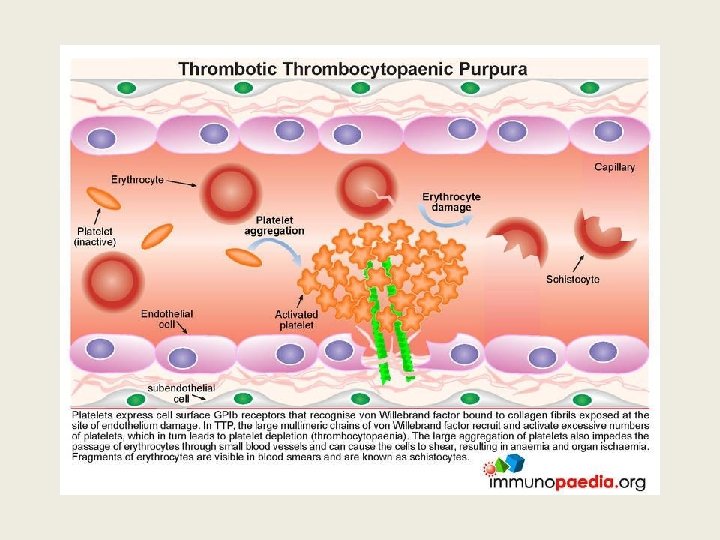
TTP ? Thrombotic thrombocyopenic purpura Ø Acute syndrome of MA haemolytic anaemia, thrombocytopenia and evidence for microthrombi: • Often Neurological or cardiac symptoms/signs • Usually mild proteinuria, mild renal impairment • Microthrombi are platelet and VWF rich Ø Deficiency of ADAMTS 13, a metalloprotease, often due to autoantibodies or congenital

TTP: ADAMTS 13 activity <10% • Metalloprotease which cleaves VWF • Deficiency leads to persistence of unusually large v. WF multimers. • Acquired: Autoantibody to protease • Congenital: ADAMTS 13 gene mutation • FRET (Flourescent resonance energy transfer), ELISA assays available as kits • TEST for enzyme activity and Antibody presence
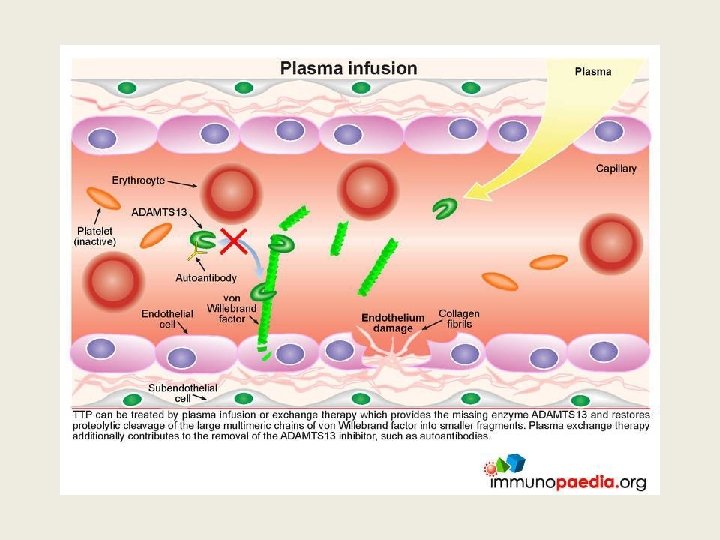

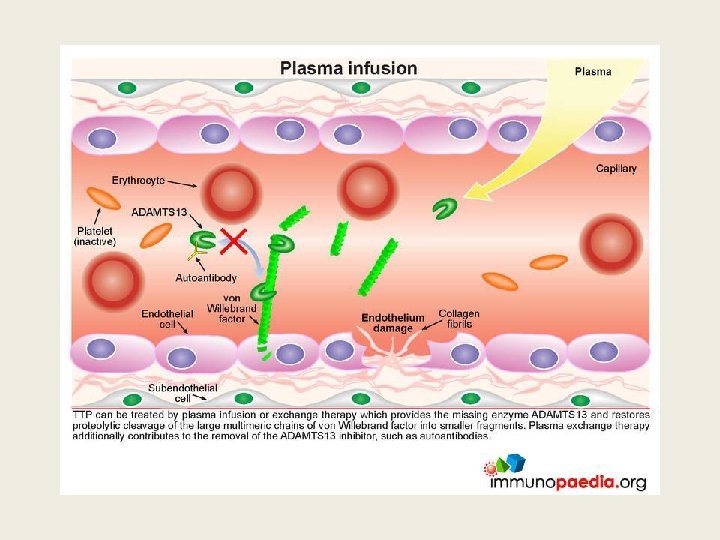
Importance of recognizing TTP early • Untreated TTP has 100% mortality, 50% occurring within 24 hr of diagnosis • Plasma exchange (PEX), corticosteroids, and use of rituximab achieves >90% survival • NB avoid platelet transfusion as it can aggravate the disease

Suspect TTP: Urgent referral for plasma exchange • TTP must be considered in all patients presenting with thrombotic MA • TTP is life threatening with 50% deaths within 24 hr of diagnosis • Diagnosis based on clinical history, examination and blood film. • ADAMTS 13 assay: activity or antibody assay, Not emergency tests, used to confirm and monitor TTP

How I treat TTP and HUS. Marie Scully and Tim Goodship. BJH Jan 2014

Atypical HUS ? Triad of thrombocytopenia, MAHA and renal failure in 100% of cases (HUS: diarrhoea positive syndrome due to Shigalike toxin producing E coli ) • Excessive complement activation on the surface of the renal microvacsulature • Sporadic and familial • 60% have inherited or acquired abnormality of complement system including mutations

a. HUS diagnostic criteria Exclusion • Shiga toxin assoc HUS • Secondary causes ü Drugs, ü Cobalamin deficiency ü Infection, HIV, Strep p ü Transplantation ü SLE, APLs, scleroderma ü ADAMTS 13 Antibodies or deficiency Inclusion • Renal biopsy showing a TMA And /or • Classic triad of MAHA, Thrombocytopenia and renal failure

Plan for Patient P • • Urgent referral for discussion of PEX TTP: not acute, renal failure, HUS : no diarrhoea, not acute, not oliguric a. HUS: triad present, but not acute and underlying metastatic cancer • PEX not useful in malignancy /chemo related MAHA • • PEX not indicated immediately given clinical history Give FFP immediately: to provide ADAMTS 13, Check ADAMTS 13 assay Heart failure and BP management

Diagnosis for Patient P: TMA • Not TTP: ADAMTS 13 activity is >10% • Not HUS: no diarrhoea • Not a. HUS: underlying metastatic malignancy and gemcitabine chemotherapy • Secondary TMA Management ü manage fluid overload causing heart failure, ü Unfractionated heparin by IV infusion to provide inhibition of complement pathway.

Progress of Patient P • Improved fluid balance and slow rise in platelets, • At 2 weeks fit for discharge : Std Heparin 5000 units sc bd • At 4 weeks fluid overload causing more SOB, • At 5 mths (5/5/2015): well, enjoying life Hb 94, wbc 5, plat 171, Creatinine 259, e. GFR 19, Darbepoietin alpha renal dose Enoxparin 20 mg daily Frusemide 40 mg daily

Hb 100 90 80 70 60 50 Hb 40 30 20 10 0 jan Feb Mar April May

Platelets 200 180 160 140 120 100 Platelets 80 60 40 20 0 Jan feb march April May

Creatinine 500 450 400 350 300 250 Creatinine 200 150 100 50 0 Jan Feb March April May

TMA: malignancy or drug related • LP: general well being @5 mths • MAHA secondary to metastatic malignancy less likely. • MAHA secondary to chemo more likely and reported after Gemcitabine, also carboplatin and mitomycin c.

Gemcitabine and MAHA • 0. 02 – 2. 2 % of patients treated • Renal failure, hypertension, fluid overload anaemia described in case reports • Mechanism uncertain: direct damage to endothelial cells ? • Therapy: stop chemo, steroids no benefit and PEX no use. • Eculizumab a Mo. Ab that inhibits C 5, licensed for atypical HUS and in report, 3 of 4 Gem related MAHA cases showed response. Ustwani OA et al JGastro oncol 2014, 5 (1).

How I treat TTP and HUS. Marie Scully and Tim Goodship. BJH Jan 2014

Patient P’s progress • Anaemia resolved with Darbepoietin Alpha • Thrombocytopenia resolved: enoxaparin prophylaxis substituted and then stopped. • LP remained well until Oct 2015: pain in left hypochrondrium: liver mets enlarged • Over next 3 months progressive liver decompensation, femoral DVT, • No recurrence of TMA • Died Feb 2016: metastatic breast cancer

Thank you

How I treat patients with TTP. James George BLOOD, 18 NOVEMBER 2010 VOLUME 116, NUMBER 20

How I treat refractory thrombotic thrombocytopenic purpura. Farzana A. Sayani and Charles S. Abrams Blood March 2015
- Slides: 44