SPSP Acute Adult Early Warning Scoring A digital






























- Slides: 32
SPSP Acute Adult Early Warning Scoring: A digital solution in this digital age Wednesday 25 th November 2020 Gavin Simpson, Consultant Critical Care & Anaesthetics, NHS Fife Scott Hamilton, Associate Improvement Advisor, HIS
Meeting participation During the meeting please have your microphone on mute and video turned off to avoid distraction for you and also to minimise the likelihood of slowing down the technology. To take part in discussions use the chat box or raise your hand wait to be invited to speak, please then: • unmute your mic • turn on your video (if you are happy to do so) • after speaking please re-mute and turn your video off
Trouble Shooting Any technical issues, please contact: Sarah Hatton via • MS Teams chat • Email: sarah. hatton 4@nhs. scot • Phone: 07866130719
Aims of the session • Sharing the experience of NHS Fife, implementing Electronic Early Warning Scoring • Reflecting on the implementation challenges and outline the key successes. • Open forum to answer questions on implementing Electronic Early Warning Scoring
Follow us on Twitter @spsp_Acute. Adult #spsp. Det. Pat
Know the Score Triage Deteriorating Patient Observations Taken Clinical Help Called For Medical Response
Analogue Observations Audit 2012 Potential observations 18, 807 in 274 patients • 60% of all observations were done • 55% of observation sets complete • 8% of observations miscalculated Correct full sets of observations completed and scored correctly • 49% only
Reasons for No Response • • 42% did not receive appropriate clinical response from staff despite most (69. 2%) recognising patient met criteria for activating RRS, and (75. 8%) ‘quite’, or ‘very’ concerned about their patient. predominantly sociocultural reasons for failure to activate the RRS.
30 25 20 Time in hours from 1 st trigger until transferred > 26 hours 15 10 5 0 Ed Greenwood 2014
e - Track and Trigger Helping Prevent Adverse Events
Track Trigger Alert
• Automatic calculation of Early Warning Scores removes human error • NEWS 2 • Maternity (MEWS) • Paediatrics (PEWS) • ED • Automatic charting of all observations and trends – time saving, clearly readable, data available anywhere, anytime • No risk of damage or loss on wards like paper charts • Auto-escalations to clinicians removes the need to bleep doctors from crowded nurses’ stations
• User-friendly interface • Time-saving • Highlights priority patients to identify deterioration in early stages • Nursing data that is captured is available across the hospital immediately, and accessible on various devices • e-Observations • Nursing Care Plans & Tasks • e-Assessments • SEPSIS • AKI
FLAGS NOCC DNACPR NFA 4 AT REGIMES T 2 RF PROFILES FREQUENCY OBSERVATIONS Specific Profiles eg – Post op Biopsy Endoscopy
• Can define individual parameters • Returns to baseline after defined period • History record • Avoid Alert Fatigue • Patient centred
• Highlights clinical deterioration in patients • Mobile as well as desktop – access anywhere • Customised nursing views to ensure users are best enabled to provide safest care
Safety Huddle
Reflections
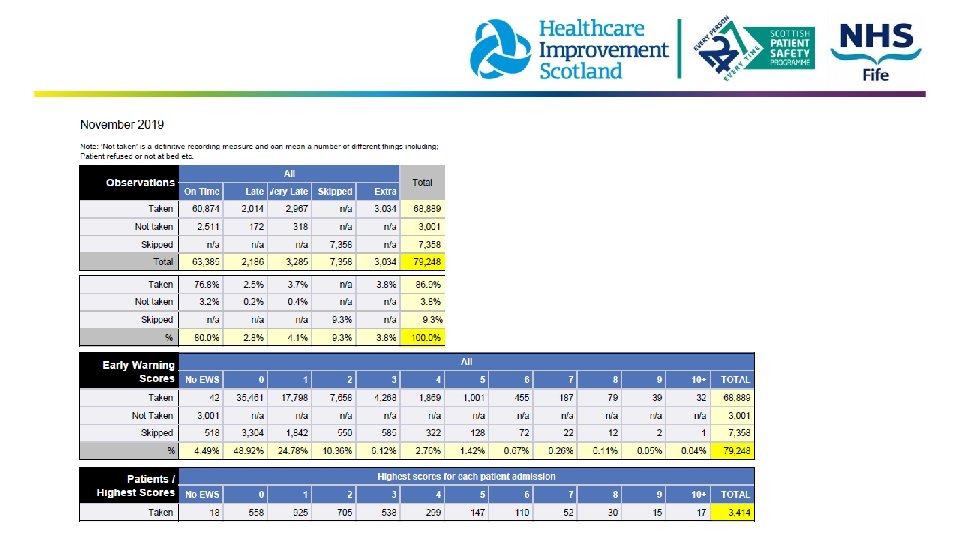
Efficient and Transparent • Refreshes every minute • Patient – Nursing Time debate • Ensuring charts viewed • Big Screens in clinical areas • 16, 000 sets obs/ week • Observations = 2667 / hours week nursing • Optimise by 5% and save 6400 hours / year • Automated Obs machines
Observations Completed Accurately on Time 83. 2% 52 % Over 80, 000 sets obs per month. .
Chain Length Time to TRIAGE OR CLINICAL IMPROVEMENT 280 260 244 min 240 220 200 180 160 172 min 140 120 100 30 % Improvement
Manchester
No increased mortality for patients admitted out-of-hours compared to in-hours. Fall in risk of death over the study period. International Symposium on Intensive Care and Emergency Medicine, Brussels 2015
BMJ Quality and safety Oct 2015
Overview Tips • PATIENTRACK is a tool; • Deteriorating patients process needs to be good • Project must be clinically led • Leadership at ward level • Senior management support • Wi-fi coverage assessment • Mobile technology important • Processes for broken kit • Analytics requires resource • Back up procedures for down time • Hard alerting input from telecoms/system build/testing • Process for handsets receiving texts; • Ownership of those • Similar to the arrest bleep
Next Time? Different: • Alerting. Plan for making this work. • Quicker roll out from the start. Clinical buy in and organisation support – then it went quickly. Training: • Champions in wards. • System is intuitive and can be picked up quickly. • 2 weeks per ward area support hands on ward-based training. • Covid - done remotely 1: 1 with cascade training between peers. Passwords: • Process for locum, bank staff, student nurses. • Rotating medical staff induction process for receiving logins. • Generic accounts with view only access - can view charts.
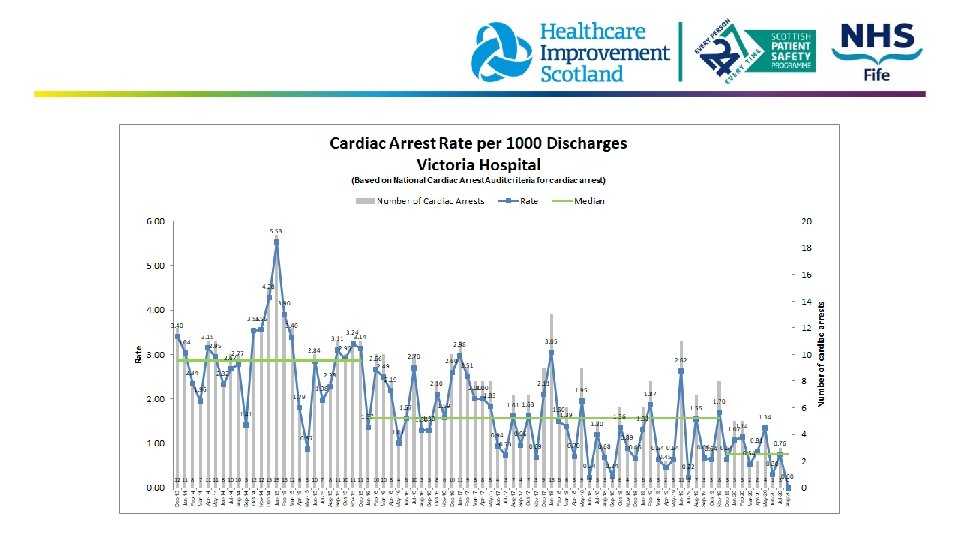
Electronic Track & Trigger benefits • • • Improved Observations Better Communication View sick patients Easy process audit Reduced Cardiac Arrests
Questions?
Evaluation and Thank You
Other References 1. 2. 3. 4. 5. 6. 7. Lang A, Simmonds M, Pinchin J, et al. The Impact of an Electronic Patient Bedside Observation and Handover System on Clinical Practice: Mixed-Methods Evaluation. JMIR Med informatics. 2019; 7(1): e 11678. doi: 10. 2196/11678 R. P, S. W, R. W, et al. Implementing an electronic observation and early warning score chart in the emergency department: a feasibility study. Eur J Emerg Med. Published online 2016 Jones S, Mullally M, Ingleby S, Buist M, Bailey M, Eddleston JM. Bedside electronic capture of clinical observations and automated clinical alerts to improve compliance with an Early Warning Score protocol. Crit Care Resusc. 2011; 13(2): 83 -88 Prytherch DR, Smith GB, Schmidt P, et al. Calculating early warning scores—A classroom comparison of pen and paper and hand-held computer methods. Resuscitation. 2006; 70(2): 173 -178. doi: 10. 1016/j. resuscitation. 2005. 12. 002 Subbe CP, Duller B, Bellomo R. Effect of an automated notification system for deteriorating ward patients on clinical outcomes. Crit Care. 2017; 21(1). doi: 10. 1186/s 13054 -017 -1635 -z Bates DW, Zimlichman E. Finding patients before they crash: The next major opportunity to improve patient safety. BMJ Qual Saf. 2015; 24(1): 1 -3. doi: 10. 1136/bmjqs-2014 -003499 Schmidt PE, Meredith P, Prytherch DR, et al. Impact of introducing an electronic physiological surveillance system on hospital mortality. BMJ Qual Saf. 2015; 24(1): 10 -20. doi: 10. 1136/bmjqs-2014 -003073