Spine made easy Spondylolisthesis Waleed Awwad MD FRCSC







.")
















































- Slides: 58
Spine made easy Spondylolisthesis Waleed Awwad. MD, FRCSC Assistant professor consultant spine surgeon
History
Spondylolisthesis • Displacement of one vertebra in relation to another vertebra below • Incidence: • Affects 5 -7% of US population • 85% at L 5 • 10% at L 4 • Natural history: • Progression observed in children • Adults, 8 -30% present after 4 th decade
Spondylolysis Spondylolisthesis
Classification • Etiology: • Wiltse classification • Marchetti-Bartolozzi classification • Severity: • Meyerding classification
Marchetti-Bartolozzi classification I. Developmental • • High dysplastic with lysis or with elongation Low dysplastic with lysis or with elongation II. Acquired • • Traumatic (due to acute or stress fracture) After surgery (caused by direct or indirect surgery) Pathological (due to local or systemic pathology) Degenerative (found in primary or secondary degenerative conditions)
Wiltse classification
Wiltse classification • Type I dysplasia (congenital).
Dysplastic changes • Proximal sacral rounding • Trapezoidal L 5 • Vertical sacrum • Junctional kyphosis • Compensatory hyper-lordosis
Wiltse classification • Type II isthmic.
Wiltse classification • Type III degenerative.
Wiltse classification • Type IV post traumatic.
Wiltse classification • Type V pathological.
Wiltse classification • Type VI iatrogenic
Meyerding grading system
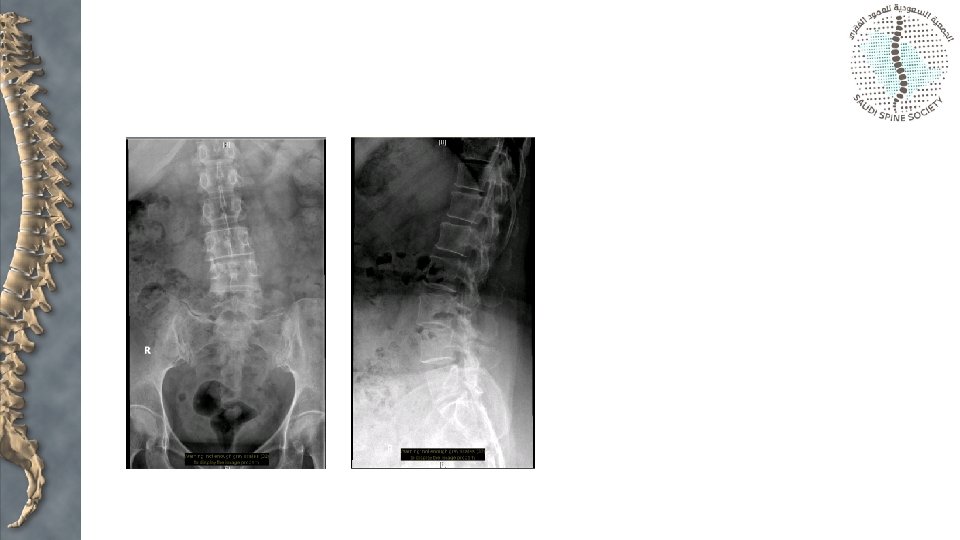
Assessment • X-rays: • Anteroposterior • Lateral • Oblique views
Assessment • X-rays: • Anteroposterior • Lateral
Assessment • X-rays: • Anteroposterior • Lateral • Oblique views Pedicle “eye” Ascending process (ears) Transverse process (nose) Spondylolysis (collar) Descending process (legs)
Assessment • X-rays: • • Anteroposterior Lateral Oblique views CT scan
Assessment • X-rays: • • • Anteroposterior Lateral Oblique views CT scan Bone scan
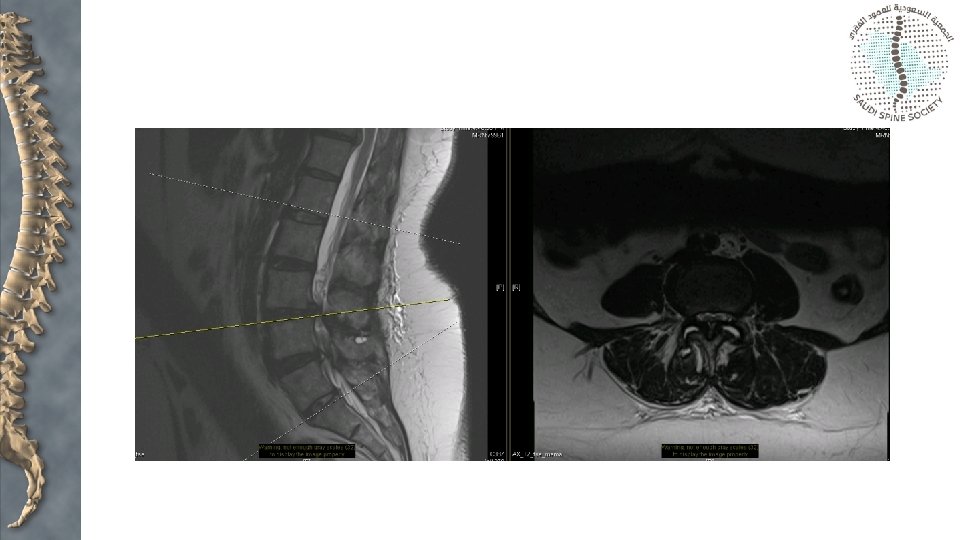
Assessment • X-rays: • • • Anteroposterior Lateral Oblique views CT scan Bone scan MRI
Spinal canal stenosis: facet joint orientation “Sagittal” “Coronal”
Spinal canal stenosis: facet joint orientation • Facet orientation > 45 degrees is 25 times more likely to develop degenerative spondylolisthesis most commonly at L 4/5 • Women: Men = 5: 1 • African-American women > Caucasian women
Spinal canal stenosis: facet joint orientation Buttress Sagittal orientation of facet joints
Spinal canal stenosis: facet joint orientation Buttress Decompression and removal of this buttress can create instability when load is applied
Spinal canal stenosis: facet joint orientation Coronal orientation of the facet joints enables decompression of neural elements without creating instability
Spinal canal stenosis: synovial cysts • Indicates presence of significant joint and synovial pathology • Need to excise synovium or immobilize the segment in order to prevent recurrence
Spinal canal stenosis: facet joint fluid or gas Fluid Gas Fluid or gas in the facet joint of a patient indicates the presence of instability
Spinal canal stenosis: facet joint fluid or gas Supine Standing
Spinal canal stenosis: intervertebral disc height
Spinal canal stenosis: intervertebral disc height
Spinal canal stenosis: intervertebral disc height Undercutting facetectomy
Spinal canal stenosis: intervertebral disc height Expect loss of disc height over time
Spinal canal stenosis: intervertebral disc height Adequate decompression initially Recurrence of foraminal compromise over time
Spinal canal stenosis: intervertebral disc height
Assessment—Meyerding Classification
Assessment—slip angle Standard method of measurement Method used when inferior end plate of L 5 is irregular
Measurement • Slip angle
Measurement • Slip angle • Normally Negative or 0
Measurement • Sacral inclination • Normally > 30 degrees
Measurement • Pelvic incidence • • • PI = PT + SS Mean children 47 degrees Mean adults 57 degrees Low PI loss of lordosis High exaggerated lordosis
Low PT High SS High PT Low SS
Sagittal alignment • Stance • Gait • Head over pelvis • Hips and knees
Risk factors for progression • • • Young age (progression is rare after 20 years) Female Ligamentous laxicity > 50% slippage > 10% slip angle L 5 - S 1 instability Trapeaoidal L 5 Dome- shaped upper sacrum Less likely to progress with decreased disk space and an Anterior sacral lip
Treatment • Majority can be managed nonoperatively: • • • NSAIDS Physical therapy Pars interarticularis injection Facet injections above defect (communicates with defect) Nerve root blocks for root symptoms
Treatment • Indications for Surgery: • Persistant back pain which interfere with activities of daily living • Symptomatic with failed conservative treatment • Significant progression • Grade III or higher with >55 degrees slip angle • Neurologic deficits • Acute traumatic
Treatment • Surgery may be indicated to treat persistent radiculopathy and/or back pain when origin of pain is localized to the spondylolisthesis level • PLF results in good outcome if fusion in situ performed • Where reduction is undertaken, 360 o fusion preferred
Surgical options • Fusion in situ and decompression • Decompression and reduction • Posterior lateral fusion and anterior column support
Gill laminectomy • Nerve root decompression • Removal of lamina of the affected level • May lead to increased instability • Radicular symptoms may persist unless decompression is accompanied by fusion to stabilize the segment in order to prevent ongoing neural irritation
High grade • Gaines resection • Sacral osteotomy • Fibular strut - Bohlman • Increased risk of neurological compromise (L 5 nerve root) with attempted reduction
Take-home messages • The majority of patients with a spondylolysis or listhesis are asymptomatic • Initial treatment should focus on activity modification and core stabilization • Surgery indicated for patients with: • Failure of nonoperative treatment • Significant or progressive deformity • Neurological compromise • The aim of surgery is to: • Decompress neural elements and preserve function • Reduce lumbosacral kyphus • Achieve fusion