Pancreas Transplant Pathology A Surgeons Perspective Jon Odorico









")











 Early (<90 d) Late (>90 d) Number (POD) 8")
 occurs early and late after SPK • Approximately")








- Slides: 32
Pancreas Transplant Pathology: A Surgeon’s Perspective Jon Odorico M. D. , F. A. C. S. University of Wisconsin-Madison
Richard Lillehei and William Kelly – First successful pancreas transplant - December 16, 1966
Pancreas Graft Survival UW Experience SPK PAN 1 year rates SPK 88% P = 0. 03 PAN 87%
Outline • Diagnosis and treatment of acute rejection in pancreas transplantation at the University of Wisconsin • Antibody mediated rejection in SPK recipients • Chemokine expression in pancreas transplant biopsies
Algorithm for Workup of Elevated Enzymes Amylase/Lipase Early < 90 days CT Scan US guided Needle Core Biopsy Late > 90 days US + Needle Core Biopsy
Allograft Dysfunction – Indications for Biopsy • Hyperamylasemia (>100 U/L or greater than 2 fold increase) and hyperlipasemia • Decreased urinary amylase (≥ 50% baseline) • Mild hyperglycemia (2 consecutive fasting glucose >200) • Unexplained fever (>38. 5ºC) • Tenderness over graft site
Needle Core Biopsy of the Pancreas Why? • Serum Enzymes - non-specific and only 70% accurate • No 100% accurate serologic or urinary marker of acute rejection • Accurate diagnosis of rejection avoids unnecessary over immunosuppression • Diagnosis of other pathologies • Significant incidence of isolated pancreas rejection in SPK transplants ~5 -15%
Non-Rejection Causes of Elevated Enzymes • Enteric Drainage • pancreatic enzyme leak • enteric leak • peripancreatic infection • pancreatic pseudocyst • small bowel obstruction • Bladder Drainage • pancreatic enzyme leak • bladder anastomosis leak • peripancreatic infection • pancreatic pseudocyst • reflux pancreatitis
Elevated Normal Serum Amylase Biopsy Rejection No Rejection 48 18 6 7 Sensitivity = 89% Specificity = 28% Normal Accuracy = 70% N=79 PV+ = 73% PV- = 54%
0 1 2 3 4 Serum Creatininine (mg/d. L)
Real – time Ultrasound Guidance
Treatment of Acute Rejection in Solitary Pancreas Transplant Recipients UW Experience 67. 4 % 28. 3 % 184 192 195 P=NS 209 4. 3 % CS CS/AB Px
Management of Grade I Pathology and Outcomes – UW 1997 -2007 – 21 of 179 biopsies If something else is going on no antirejection treatment If no other imaging findings or suspected infections, then treat
Percutaneous Needle Core Biopsies UW Experience 1997 -2007 Complications 179 biopsies P = 0. 045 US or CT guided biopsy 57. 9 % percutaneous needle core Complication rate – 8 (4. 5%) No graft losses 145 194 18. 4 % 15. 8 % 7. 8 %
Summary • Serum enzyme markers are imperfect • Rejection grade correlates with outcome • Grade I pathology in setting of elevated enzymes and no other explanation probably represents early rejection • Subset of Grade I histopathology may benefit from early treatment
Surveillance or Protocol Biopsies ? ? What do the infiltrates mean? Are infiltrates pathological in all cases? When and how 57. 9 often? % P = 0. 045 Increasing evidence of the deleterious effect of subclinical rejection on CAN in kidney transplants Makes sense when there are poor serological 194 18. 4 % 15. 8 % markers of rejection and biopsy is safe , 145 i. e. heart, lung transplantation 7. 8 % ? Useful in Solitary Pancreas transplants; probably not necessary in SPK patients
C 4 d+ Kidney Transplant Rejection in Simultaneous Kidney Pancreas Transplantation: Differential Effects on Kidney vs. Pancreas Transplants LT Chin, M Samaniego, YT Becker, J Odorico, JD Pirsch, HW Sollinger Departments of Surgery and Medicine University of Wisconsin School of Medicine and Public Health Presented at ATC 2006
Antibody-Mediated Rejection in SPK • Evaluate effect of AMR on kidney and pancreas transplant function. – identified patients with AMR kidney – are pancreas transplants susceptible to circulating alloantibody ? – Does pancreas tx outcome parallel that of the kidney tx ?
Antibody-Mediated Rejection in SPK • Retrospective database review of all SPK transplants that presented with C 4 d+ rejection of the kidney allograft from October 2002 -October 2005. • N = 34
Antibody-Mediated Rejection in SPK • C 4 d deposition in the peritubular capillaries and kidney allograft dysfunction • All patients underwent kidney biopsies for elevated Cr ( Scr ≥ 25%).
Antibody-Mediated Rejection in SPK • Elevated serum amylase or lipase was used as a surrogate marker of pancreas allograft rejection. • No pancreas biopsies were performed. • Donor specific antibody (DSALuminex®) data were collected whenever available.
Antibody-Mediated Rejection in SPK (n=34) Early (<90 d) Late (>90 d) Number (POD) 8 (7 -38) 26 (95 -5603) Cellular rejection 2/8 (25%) 17/26 (65%) Elevated Amylase 2/8 (25%) 16/26 (62%)
Summary • AMR (C 4 d+) occurs early and late after SPK • Approximately 50% have associated cellular rejection • C 4 d positivity late post transplant is associated with worse kidney transplant outcomes • Pancreas function may be unaffected even in the presence of circulating alloantibody.
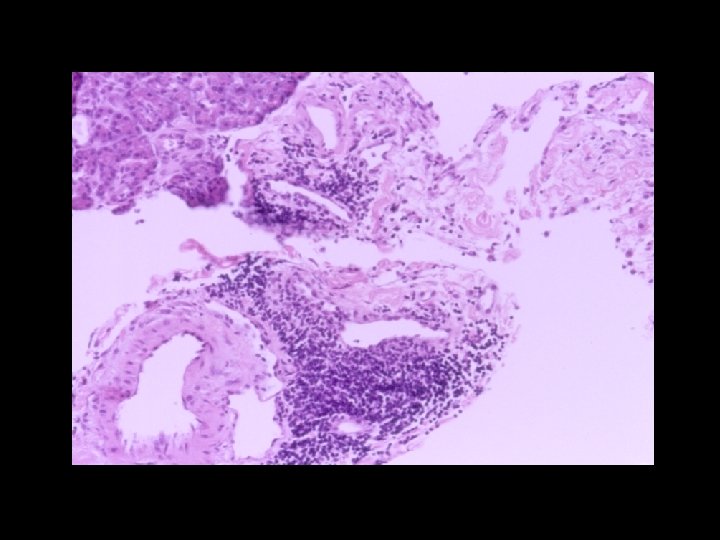
AMR Pancreas allograft Grade II C 4 d+ DSA to A 31 and B 31
AMR in Pancreas Allograft • Cell mediated rejection = venous endotheliitis, septal inflammation, lymphocytic infiltrate, eosinophilia • AMR= unknown but could be that antibody deposition and complement activation in microvasculature compromises blood flow to islets which are supplied by a capillary network much more dense than that of the surrounding exocrine tissue reference
AMR and Pancreas Transplantation • Increased expression of C 4 d has been noted in pancreas allograft biopsies undergoing acute rejection • Case report of patient with SPK undergoing AMR of both grafts with C 4 d capillary staining with serum positive for HLA Class II DSA
AMR of Pancreas Allograft • C 4 d deposition and AMR have been documented to occur in pancreas allografts • Interacinar capillaries stain positively • Standardized criteria for fulfillment of AMR in pancreas allograft should be established
Molecular Markers and Signaling Pathways of Acute Pancreatic Allograft Rejection Identified by Microarray Analysis Nathan R. Treff, Lynn M. Jacobson, Drew A. Roenneburg, Stuart J. Knechtle, Jon S. Odorico Division of Transplantation, Department of Surgery, University of Wisconsin School of Medicine and Wm. S. Middleton Memorial VA Hospital, Madison, WI
Chemokines and Rejection • Shown to play a role in human kidney, heart and hepatic allograft rejection • Also play a role in islet and pancreas allograft rejection in rodents • No studies to date have profiled the role of chemokines in human pancreatic allograft rejection 1. Fahmy NM, Yamani MH, Starling RC, Ratliff NB, Young JB, Mc. Carthy PM et al. Chemokine and chemokine receptor gene expression indicates acute rejection of human cardiac transplants. Transplantation 2003; 75: 72 -78. 2. Fahmy NM, Yamani MH, Starling RC, Ratliff NB, Young JB, Mc. Carthy PM et al. Chemokine and receptor-gene expression during early and late acute rejection episodes in human cardiac allografts. Transplantation 2003; 75: 2044 -2047. 3. Krukemeyer MG, Moeller J, Morawietz L, Rudolph B, Neumann U, Theruvath T et al. Description of B lymphocytes and plasma cells, complement, and chemokines/receptors in acute liver allograft rejection. Transplantation 2004; 78: 65 -12 4. Melter M, Exeni A, Reinders ME, Fang JC, Mc. Mahon G, Ganz P et al. Expression of the chemokine receptor CXCR 3 and its ligand IP-10 during human cardiac allograft rejection. Circulation 2001; 104: 2558 -2564.
Conclusions • Chemokines are upregulated in rejecting pancreatic allografts • IP-10 possible candidate marker of rejection • CXCR 3+ cells in both normal and rejecting allografts • Further study of chemokine signaling pathways in pancreas rejection, particularly Grade I and other non-rejection inflammatory states is recommended
Acknowledgements Tom Chin Millie Saminiego Jose Torrealba Stuart Knechtle Drew Roennenberg Anna Ibele Nathan Treff UW Biotechnology Center