LIVER TRANSPLANTATIONBASICS IN SURGERY DR CH MADHUSUDHAN M
, FRCS(Edin, UK) DEPARTMENT")
LIVER TRANSPLANTATIONBASICS IN SURGERY DR. CH. MADHUSUDHAN M. S, MCh(aiims), FRCS(Edin, UK) DEPARTMENT OF SURGICAL GASTRO ENTEROLOGY, OSMANIA GENERAL HOSPITAL, HYDERABAD
 is now established as the only definitive treatment")
Liver Transplantation • Liver transplantation (LT) is now established as the only definitive treatment for end stage liver disease (ESLD) • Starzl et al carried out 1 st human liver transplant in 1963 • Survival following liver transplant – 1 year survival: 87 – 93% – 3 year survival: > 75% . . . (http: //www. ustransplant. org The 2009 Annual Report of the OPTN and SRTR: Transplant Data 1999 -2008).

• A liver transplant is a surgical procedure performed to replace a diseased liver with a healthy liver from another person. • The liver may come from a deceased organ donor(DDLT) or from a living donor(LDLT). • An entire liver may be transplanted, or just a section. • Because the liver is the only organ in the body able to regenerate, a transplanted portion of a liver can rebuild to normal capacity within weeks.

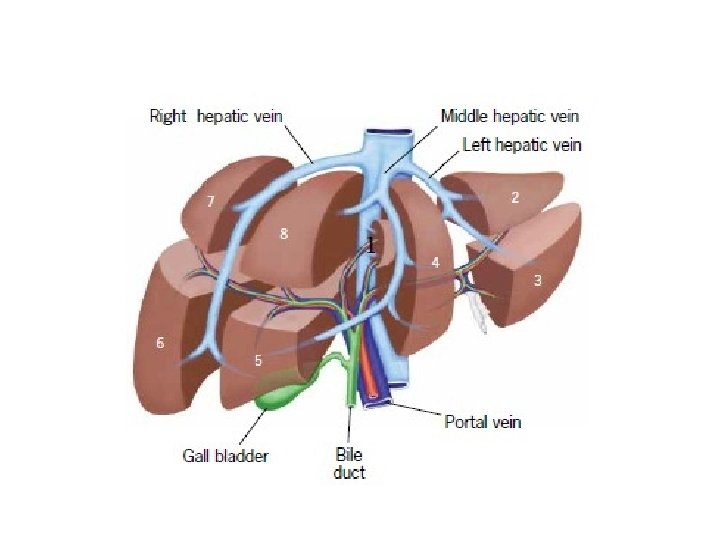
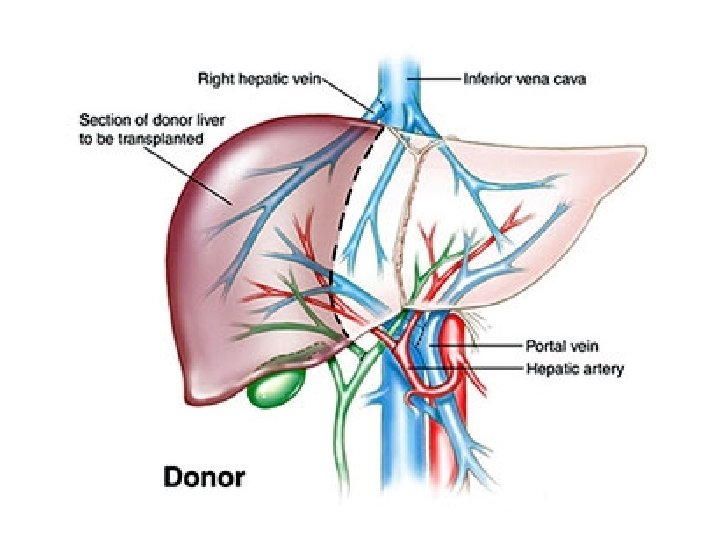
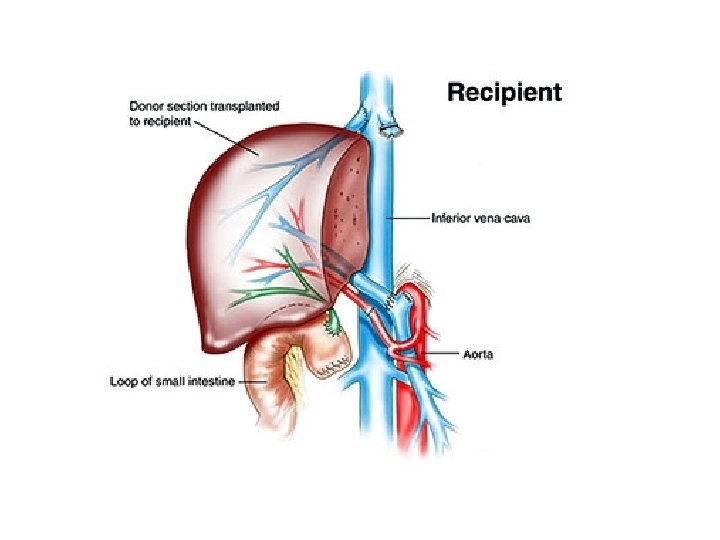
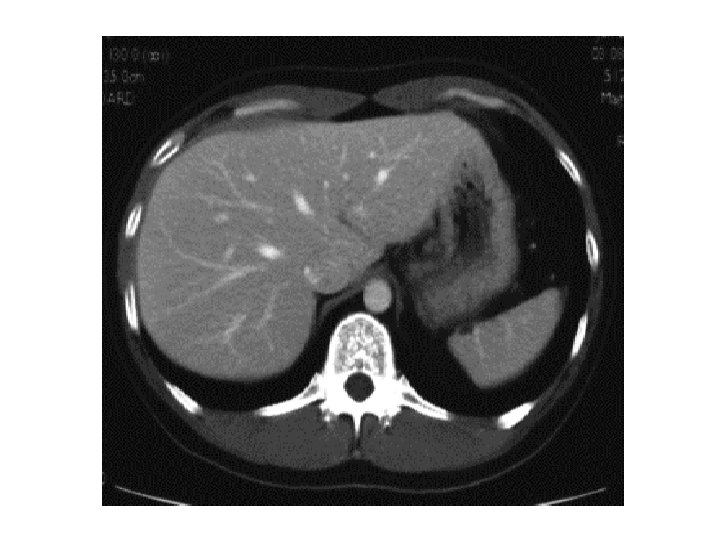
ANATOMY

ANATOMY
 (DDLT) • Living donor liver")
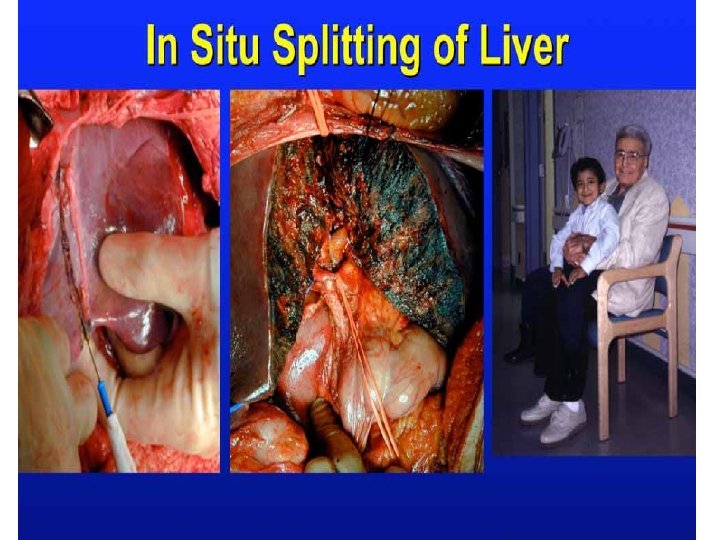
Types of liver transplantation • Disease Donor liver transplantation(cadaveric) (DDLT) • Living donor liver transplantation (LDLT) • Split liver transplantation • Reduced size transplantation • Auxiliary liver transplantation • DCD (Donation After cardiac deathcadaveric) • Hepatic cell transplantation

Types of Liver transplant • Orthotopic liver transplantation – Donor liver is transplanted in normal anatomic position – Commonly practiced • Heterotopic liver transplantation Donor liver is placed within abdominal cavity with patient’s native organ occupying the normal anatomic position § Problems with Heterotopic LT – difficult to accommodate an extra organ in abdomen with a complex blood supply – danger of multiple anastomosis leak, kinking or compromised

Stages of Operation in Liver Transplantation Preanhepatic/ dissection phase Dissection of structures of porta hepatis & mobilization of native liver Anhepatic phase Neohepatic phase begins when native liver is removed after transection of blood supply & occlusion of supra- and infra- hepatic IVC & implantation of donor liver involves the completion of several anastomoses, haemostasis, and closure.
")
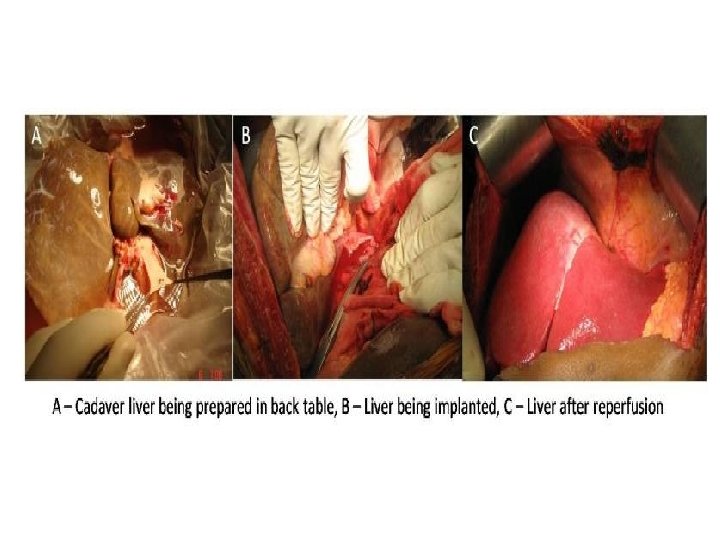
DDLT(Classical method)
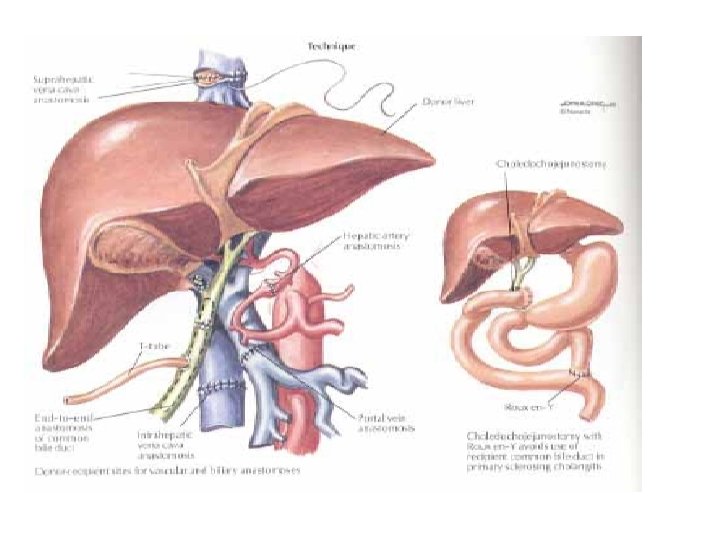

• New liver is implanted by one of two techniques: – Infra- Caval interposition – Piggy-back technique • Infra- Caval interposition – involves removal of the native liver along with intra-hepatic portion of IVC. – Complete vascular occlusion by clamping hepatic artery, portal vein, supra- and infra hepatic IVC: decreases venous return by as much as 50%. – Venous Bypass (VVBP) – When VVBP is not used: Test clamps applied on infra hepatic IVC. If patient tolerates, permanent clamps applied. • Before this step, maintain CVP b/w 10 -15 cm of Hg, cut down inhalation agent, use of small amount of vasoconstrictors
 • Diverts IVC & portal venous flow to axillary vein •")
Venous Bypass (VVBP) • Diverts IVC & portal venous flow to axillary vein • Initiated after cannulation of femoral & portal vein, & axillary or subclavian vein on left side • Continuous pump diverts blood from portal and femoral vein to suprahepatic veins. • Attenuates the decrease in preload, improves renal perfusion pressure, lessens splanchnic congestion, and delays the development of

Piggy-back Technique Allows removal of liver without removing a portion of the vena cava. One end of donor IVC is closed and other end is anastamosed to recipient IVC end to side. Temporary porto-caval shunt is performed to reduce the portal pressure. Adv. : improved haemodynamics Disadv. : surgically more difficult than caval

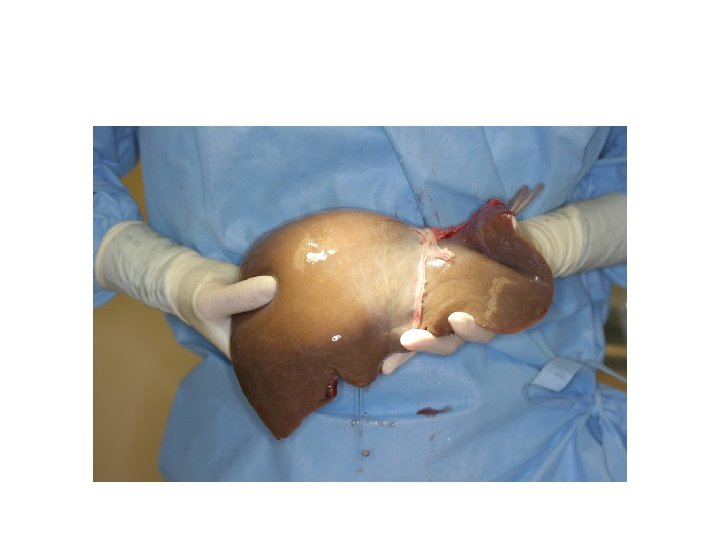
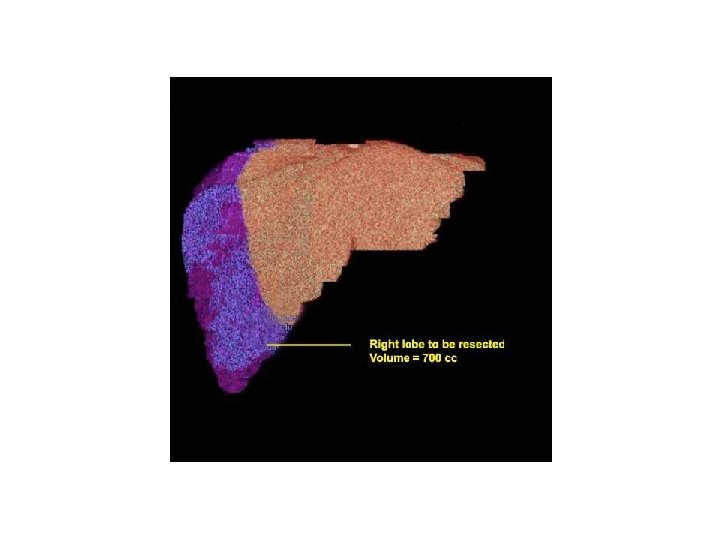
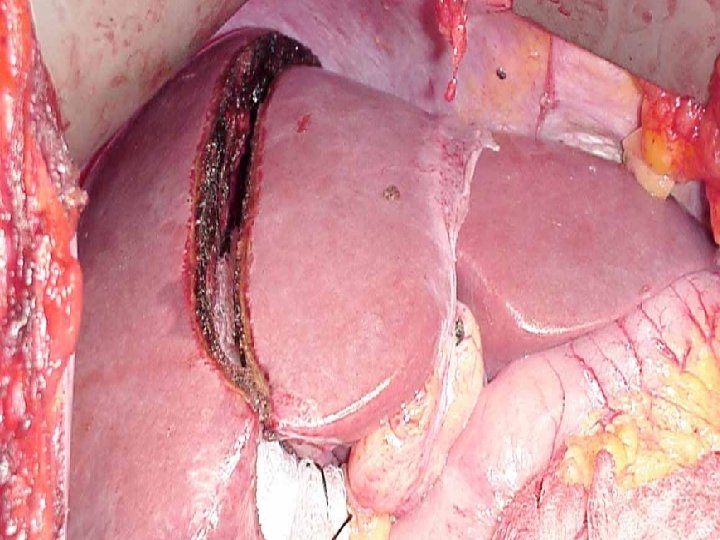
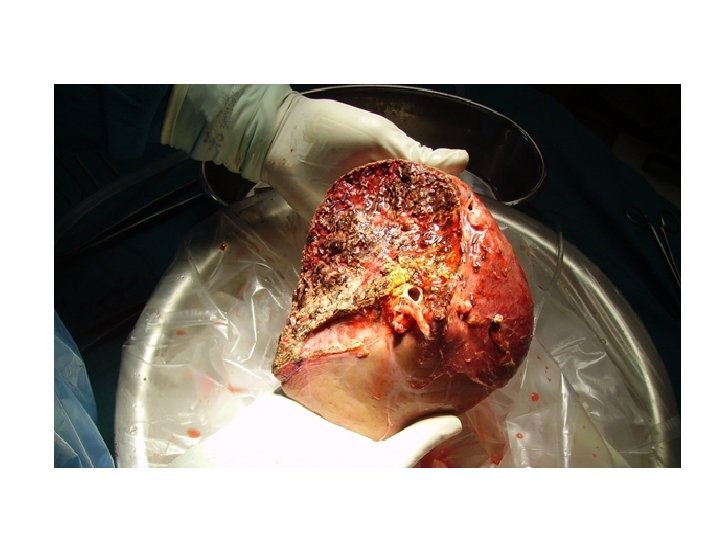
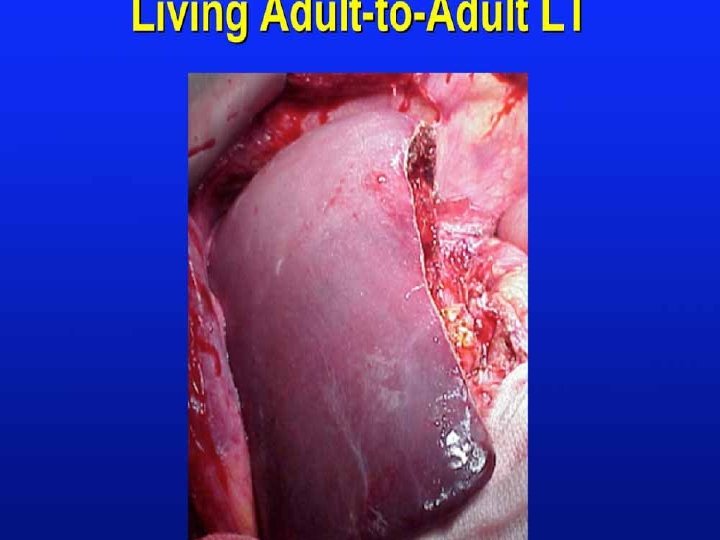
LDLT

 – characterized by encephalopathy,")
Complications of LT 1. Primary Nonfunction – (up to 5%) – characterized by encephalopathy, coagulopathy, minimal bile output, and progressive renal and multi organ dysfunction with increasing serum lactate level, increasing metabolic acidosis, rapidly rising liver enzymes & histological evidence of hepatocyte necrosis in absence of any vascular complication. – Donor risk factors implicated in primary graft dysfunction • • • prolonged cold ischaemia time unstable donor high level of steatosis in the liver allograft older donor high serum sodium level in the donor

……. Complications – Patients with initial primary dysfunction may recover with support but those who progress to show evidence of extra hepatic complications such as hemodynamic instability, renal failure or other organ systems dysfunction may require urgent retransplantation. 2. Hepatic artery thrombosis leads to graft necrosis. Patency of HA is determined by Doppler USG. Early intervention can salvage graft & prevent need for regrafting. 7. Vena caval thrombosis (rare) 3. Biliary leak or obstruction 8. Intraabdominal sepsis 4. Nonspecific Cholestasis 9. Neurologic complications 5. Haemorrhage 6. Portal vein thrombosis (rare) 10. Immunosupprission

- Slides: 33