Otosclerosis Alan L Cowan MD Tomoko Makishima MD



 n n n Father")









 n n n Osteocytes,")



















 – classification of tympanograms n Type As n Type Ad")






 of the temporal bone n Proponents of CT for")




















 n Temporalis fascia n")


")








 n More prolonged after stapedectomy compared")







- Slides: 96
Otosclerosis Alan L. Cowan, MD Tomoko Makishima, MD, Ph. D Department of Otolaryngology University of Texas Medical Branch Galveston, TX October 18, 2006
Introduction n Otosclerosis Primary metabolic bone disease of the otic capsule and ossicles n Results in fixation of the ossicles and conductive hearing loss n May have sensorineural component if the cochlea is involved n Genetically mediated n n Autosomal dominant with incomplete penetrance (40%) and variable expressivity
History of Otosclerosis and Stapes Surgery 1704 – Valsalva first described stapes fixation n 1857 – Toynbee linked stapes fixation to hearing loss n 1890 – Katz was first to find microscopic evidence of otosclerosis n 1893 – Politzer described the clinical entity of “otosclerosis” n 1890 – Bacon describes medical therapy for the condition, and supports the common view that “surgery should not be considered for a moment. “ n
History of Otosclerosis and Stapes Surgery n Gunnar Holmgren (1923) n n n Father of fenestration surgery Single stage technique Sourdille n n n Holmgren’s student 3 stage procedure 64% satisfactory results
History of Otosclerosis and Stapes Surgery n Julius Lempert n n Popularized the single staged fenestration procedure John House n Further refined the procedure n Popularized blue lining the horizontal canal
History of Otosclerosis and Stapes Surgery n Fenestration procedure for otosclerosis Fenestration in the horizontal canal with a tissue graft covering n >2% profound SNHL n Rarely complete closure of the ABG n May exhibit vestibular disturbances n
History of Otosclerosis and Stapes Surgery n Samuel Rosen n 1953 – first suggest mobilization of the stapes n n Immediate improved hearing Re-fixation
History of Otosclerosis and Stapes Surgery n John Shea n 1956 – first to perform stapedectomy n n Oval window vein graft Nylon prosthesis from incus to oval window
Epidemiology 10% overall prevalence of histologic otosclerosis n 1% overall prevalence of clinically significant otosclerosis n
Epidemiology Race Incidence of otosclerosis Caucasian 10% Asian 5% African American 1% Native American 0%
Epidemiology n Gender Histologic otosclerosis – 1: 1 ratio n Clinical otosclerosis – 2: 1 (W: M) n n Possible progression during pregnancy (10%-17%) n n Studies which have demonstrated changes during pregnancy are often retrospective or lack audiometric data. Studies comparing multigravid vs. nulligravid women with otosclerosis have failed to show audiometric differences. n Bilaterality more common (89% vs. 65%)
Epidemiology n Age 15 -45 most common age range of presentation n Youngest presentation 7 years n Oldest presentation 50 s n 0. 6% of individuals <5 years old have foci of otosclerosis n
Pathophysiology n Osseous dyscrasia Resorption and formation of new bone n Limited to the temporal bone and ossicles n Inciting event unknown n n Hereditary, endocrine, metabolic, infectious, vascular, autoimmune, hormonal
Pathology n Two phases of disease n Active (otospongiosis phase) n n n Osteocytes, histiocytes, osteoblasts Active resorption of bone Dilation of vessels n Schwartze’s sign n Mature (sclerotic phase) n Deposition of new bone (sclerotic and less dense than normal bone)
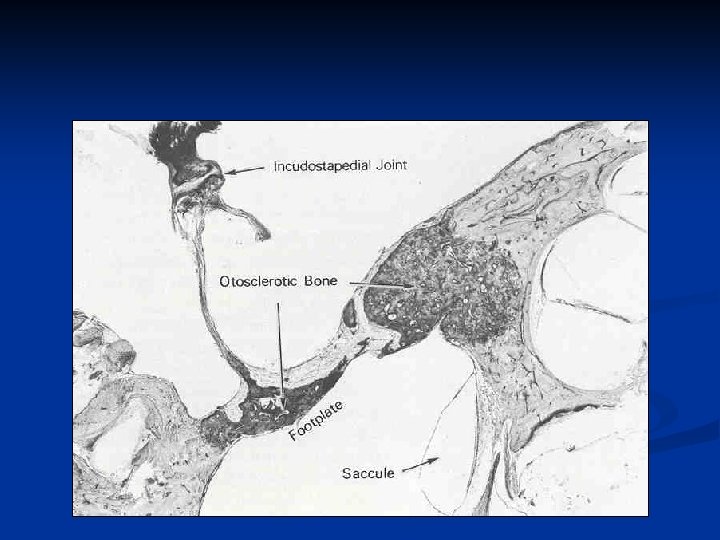
Pathology n Most common sites of involvement n Fissula ante fenestrum n Round window niche (30%-50% of cases) n Anterior wall of the IAC
Non-clinical foci of otosclerosis
Anterior footplate involvement
Annular ligament involvement
Bipolar involvement of the footplate
Round Window
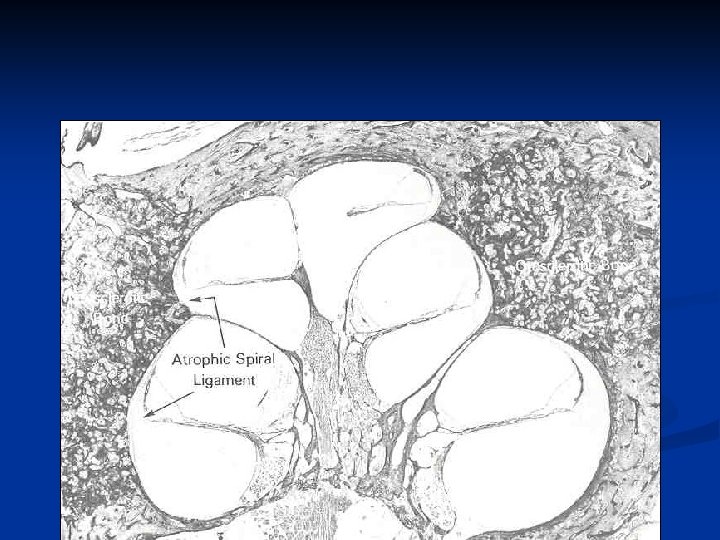
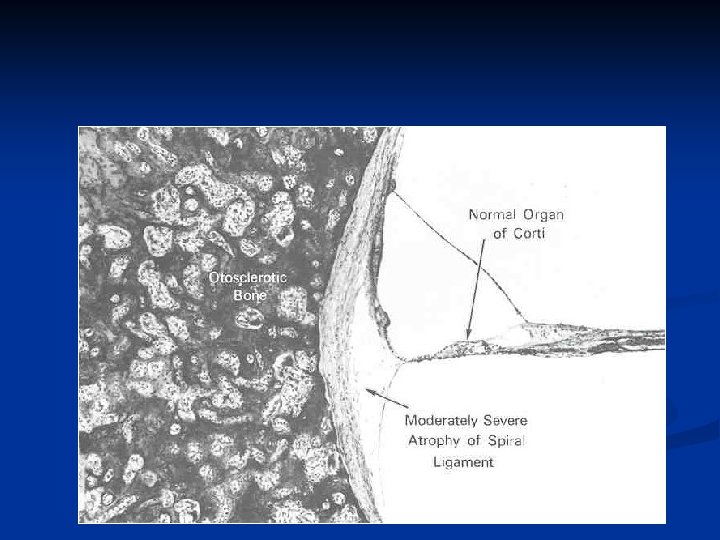
Labyrinthine Otosclerosis n 1912 – Siebenmann described labyrinthine otosclerosis n Suggested otosclerosis may cause SNHL via n Toxic metabolites n Decreased blood supply n Direct extension n Disruption of membranes
Hyalinization of the spiral ligament
Erosion into inner ear
Organ of Corti
Cochlear Otosclerosis n Audiometric studies n n Histiologic studies n n n Cases of documented otosclerosis and a large sensory loss have shown large foci of otosclerosis in the otic capsule. Many cases of large otic capsule foci without sensory loss or of sensory loss without foci have also been described. Biochemical studies n n Some studies have shown that in cases of unilateral otosclerosis ~ 60% may have decreased sensory thresholds even after stapes surgery Some authors have noted increased levels of perilymph protein during stapedotomy in patients with radiographic evidence of otic capsule foci and sensory hearing loss. Conclusion n Many experts believe that extensive involvement of the cochlea will produce sensorineural hearing deficits, although it is not known how this occurs or why it only occurs in a subset of patients with cochlear foci.
Diagnosis of Otosclerosis
History n Most common presentation Women age 20 - 30 n Conductive or Mixed hearing loss n n Slowly progressive, n Bilateral (80%) n Asymmetric n Tinnitus (75%)
History Age of onset of hearing loss n Progression n Laterality n Associated symptoms n Dizziness n Otalgia n Otorrhea n Tinnitus n
History n Family history n n n 2/3 have a significant family history Particularly helpful in patients with severe or profound mixed hearing loss Prior otologic surgery History of ear infections Vestibular symptoms n n n 25% Most commonly dysequilibrium Occasionally attacks of vertigo with rotatory nystagmus
Physical Exam n Otomicroscopy n Most helpful in ruling out other disorders n n n Schwartze’s sign n Middle ear effusions Tympanosclerosis Tympanic membrane perforations Cholesteatoma or retraction pockets Superior semicircular canal dehiscence Red hue in oval window niche area 10% of cases Pneumatic otoscopy n Distinguish from malleus fixation
Physical Exam n Tuning forks Hearing loss progresses form low frequencies to high frequencies n 256, 512, and 1024 Hz TF should be used n n Rinne n n 256 Hz – negative test indicates at least a 20 d. B ABG 512 Hz – negative test indicates at least a 25 d. B ABG
Differential Diagnosis Ossicular discontinuity n Congenital stapes fixation n Malleus head fixation n Paget’s disease n Osteogenesis imperfecta n Superior semicircular canal dehiscence n
Audiometry Tympanometry n Impedance testing n n n Acoustic reflexes Pure tones
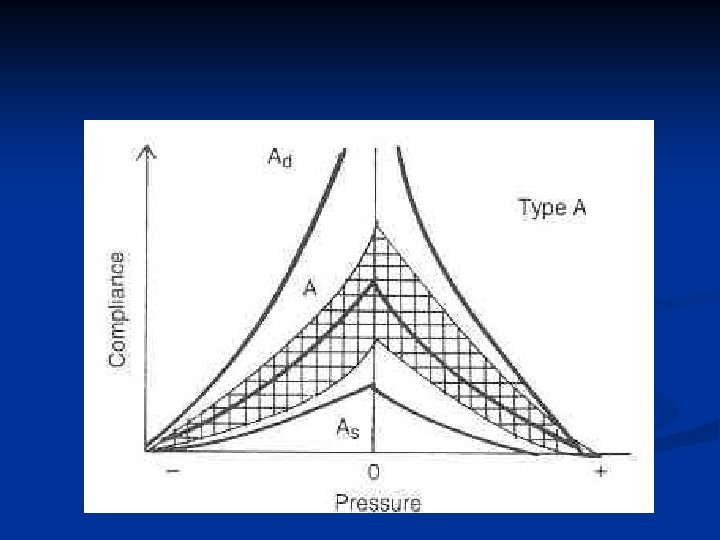
Tympanometry n Jerger (1970) – classification of tympanograms n Type As n Type Ad Type B n Type C n
Acoustic Reflexes Result from a change in the middle ear compliance in response to a sound stimulus n Change in compliance n Stapedius muscle contraction n Stiffening of the ossicular chain n Reduces the sound transmission to the vestibule n
Acoustic Reflexes n Otosclerosis has a predictable pattern of abnormal reflexes over time Reduced reflex amplitude n Elevation of ipsilateral thresholds n Elevation of contralateral thresholds n Absence of reflexes n
Pure Tone Audiometry n Most useful audiometric test for otosclerosis n n n Characterizes the severity of disease Frequency specific Carhart’s notch n n Hallmark audiologic sign of otosclerosis Decrease in bone conduction thresholds n n 5 d. B at 500 Hz 10 d. B at 1000 Hz 15 d. B at 2000 Hz 5 d. B at 4000 Hz
Pure Tone Audiometry n Low frequencies affected first n n Rising air line n n n Below 1000 Hz “Stiffness tilt” Secondary to stapes fixation With disease progression n Air line flattens
Pure Tone Audiometry n Carhart’s notch n Proposed theory n Stapes fixation disrupts the normal ossicular resonance (2000 Hz) n Normal compressional mode of bone conduction is disturbed because of relative perilymph immobility Mechanical artifact n Reverses with stapes mobilization n
Pure Tone Audiometry n Committee on Hearing and Balance n Set standards for reporting results in cases of otosclerosis procedures. n n Operative hearing results should be reported using post-operative data, specifically, the post-operative air-bone gap. This prevents exaggeration of surgical results and “overclosure. ” Adopted by the AAOHNS in 1994 Important in reviewing literature regarding surgical outcomes n n Studies prior to this time often use pre-op bone lines and post-op air conduction measurements which may exaggerate results. This convention is not uniform in all parts of the world, so the methods is very important in determining the consistency of data.
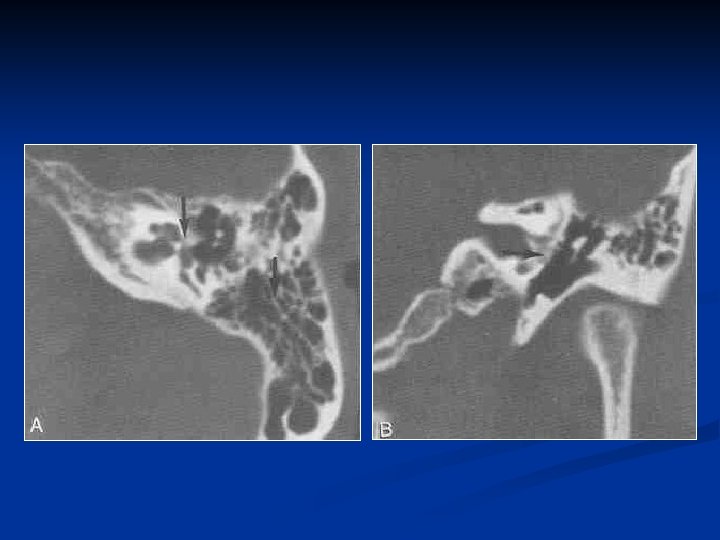
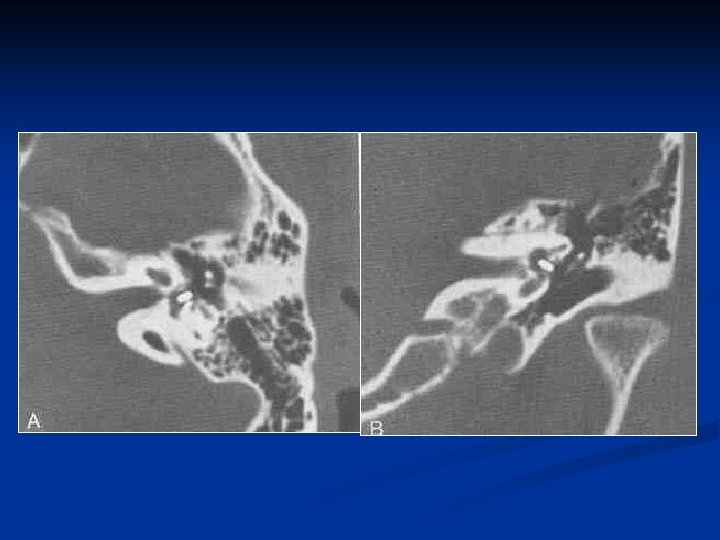
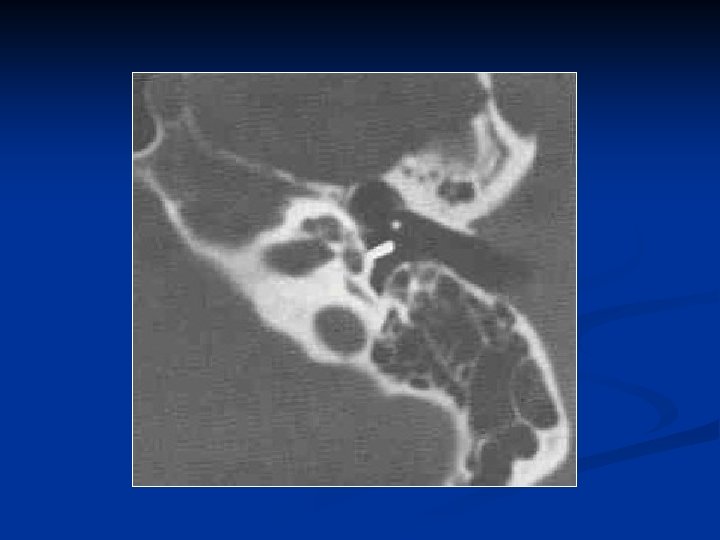
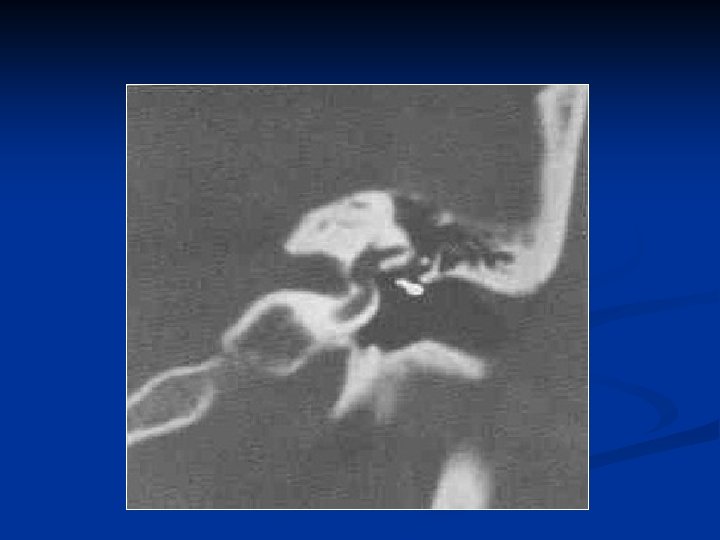
Imaging n Computed tomography (CT) of the temporal bone n Proponents of CT for evaluation of otosclerosis n Pre-op n n n Characterize the extent of otosclerosis Severe or profound mixed hearing loss Evaluate for enlarge cochlear aqueduct n Post-op n Recurrent CHL n Re-obliteration vs. prosthesis dislocation n Vertigo
“Halo sign”
Paget’s disease
Osteogenesis Imperfecta
Management Options Medical n Amplification n Surgery n Combinations n
Patient Selection n Factors Result of tuning fork tests and audiometry n Skill of the surgeon n Facilities n Medical condition of the patient n Patient wishes n
Surgery n Best surgical candidate Previously un-operated ear n Good health n Unacceptable ABG n n 25 to 40 d. B n Negative Rinne test Excellent discrimination n Desire for surgery n
Surgery n Other factors n Age of the patient n Elderly n Poorer results in the high frequencies n Congenital stapes fixation (44% success rate) n Juvenile otosclerosis (82% success rate) n Occupation n Diver n Pilot n Airline steward/stewardess
Surgery n Other factors n Vestibular symptoms n Meniere's disease n Concomitant otologic disease n Cholesteatoma n Tympanic membrane perforation
Surgical Steps n Subtleties of technique and style Local vs. general anesthesia n Stapedectomy vs. partial stapedectomy vs. stapedotomy n Laser vs. drill vs. cold instrumentation n Oval window seals n Prosthesis n
Canal Injection n 2 -3 cc of 1% lidocaine with 1: 50, 000 or 1: 100, 000 epinephrine n 4 quadrants n Bony cartilaginous junction
Raise Tympanomeatal Flap n 6 and 12 o’clock positions n 6 -8 mm lateral to the annulus n Take into account curettage of the scutum
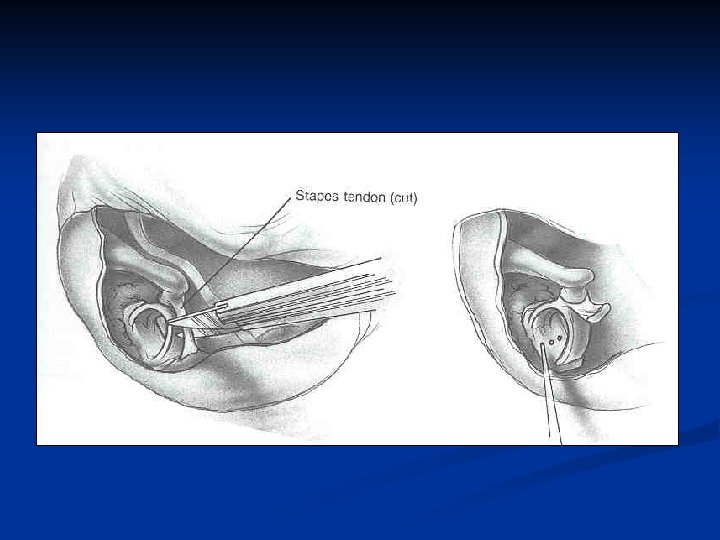
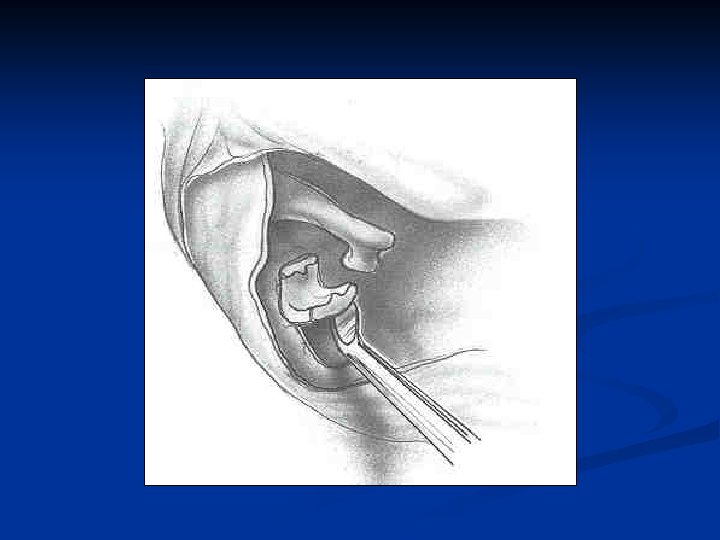
Separation of chorda tympani nerve from malleus n Separate the chorda from the medial surface of the malleus to gain slack n Avoid stretching the nerve n Cut the nerve rather than stretch it
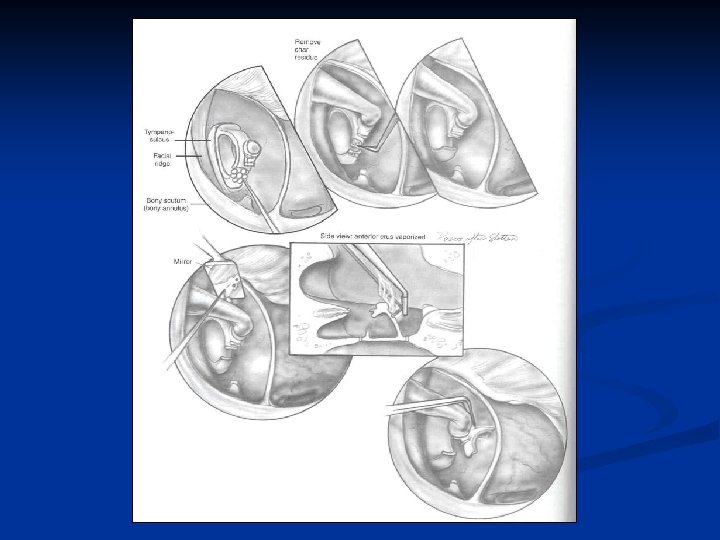
Curettage of Scutum n Curettage a trough lateral to the scutum, thinning it n Then remove the scutum (incus to the round window)
Curettage of Scutum n Exposure n Vertical: n n Horizontal: n n Facial nerve to round window Pyramidal process to malleus Preservation of bone over incus
Middle ear examination n Mobility of ossicles Confirm stapes fixation n Evaluate for malleus or incus fixation n n Abnormal anatomy Dehiscent facial nerve n Overhanging facial nerve n Deep narrow oval window niche n Ossicular abnormalities n
Measurement for prosthesis n Measurement n Lateral aspect of the long process of the incus to the footplate
Total Stapedectomy n Uses Extensive fixation of the footplate n Floating footplate n n Disadvantages Increased post-op vestibular symptoms n More technically difficult n Increased potential for prosthesis migration n
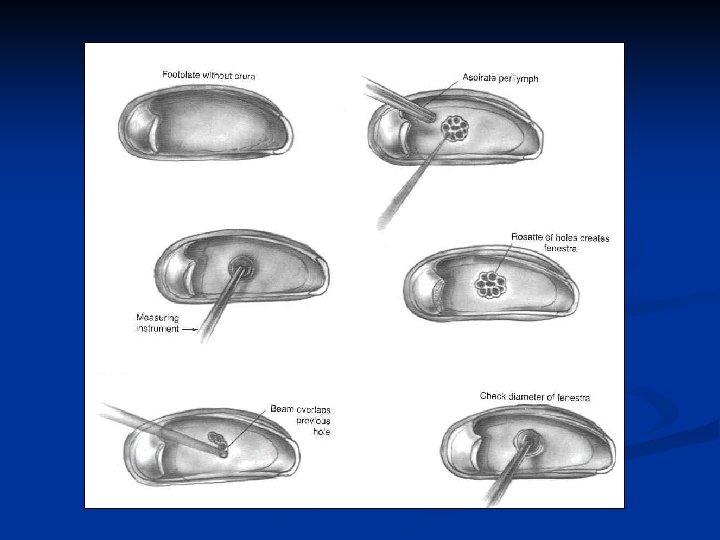
Stapedotomy/Small Fenestra n Originally for obliterated or solid footplates Europe n 1970 -80 n n First laser stapedotomy performed by Perkins in 1978 Less trauma to the vestibule n Less incidence of prosthesis migration n Less fixation of prosthesis by scar tissue n
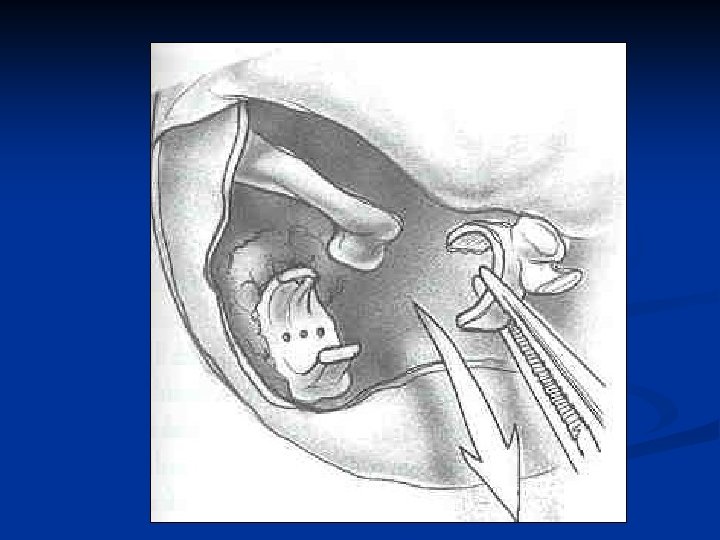
Drill Fenestration n 0. 7 mm diamond burr n n n Motion of the burr removes bone dust Avoids smoke production Avoids surrounding heat production
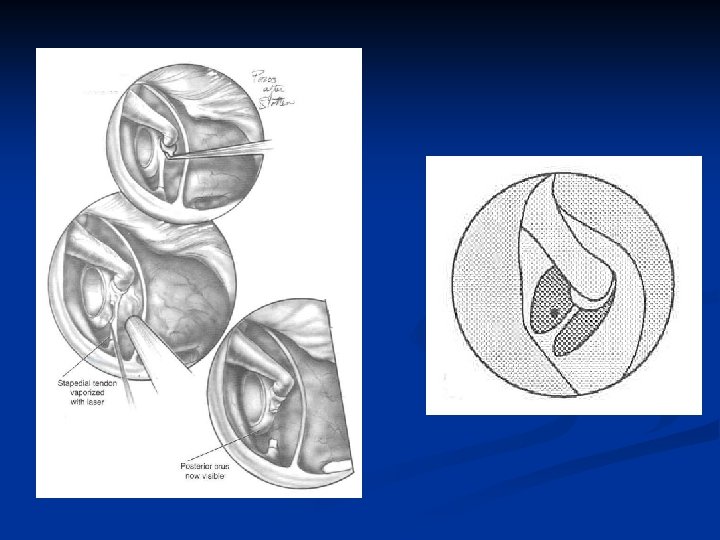
Laser Fenestration n Laser n n Avoids manipulation of the footplate Argon and Potassium titanyl phosphate (KTP/532) n n n Wave length 500 nm Visible light Absorbed by hemoglobin Surgical and aiming beam Carbon dioxide (CO 2) n n n 10, 000 nm Not in visible light range Surgical beam only n n Requires separate laser for an aiming beam (red helium-neon) Ill defined fuzzy beam
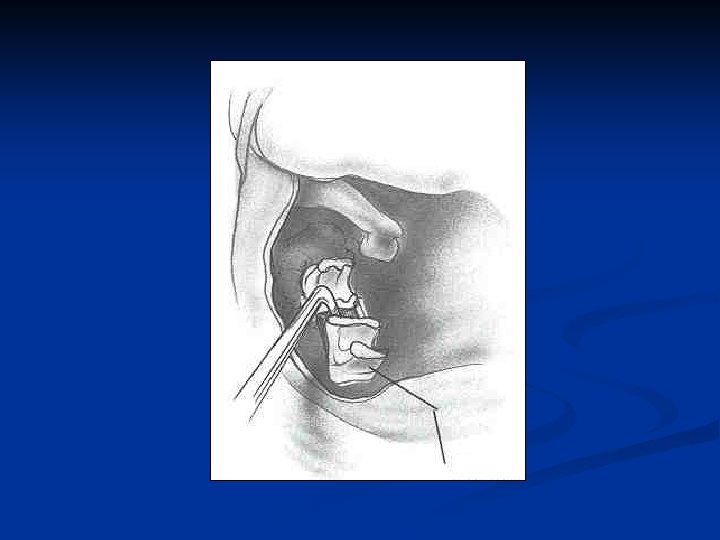
Oval window seal Tragal perichondrium n Vein (hand or wrist) n Temporalis fascia n Blood n Fat n Gelfoam (now discouraged) n
Reconstructing the annular ligament
Placement of the Prosthesis n n Prosthesis is chosen and length picked Some prefer bucket handle to incorporate the lenticular process of the incus
Stapedectomy vs. Stapedotomy n ABG closure < 10 d. B (PTA)
Special Considerations and Complications in Stapes Surgery
Overhanging Facial Nerve n n n Usually dehiscent Consider aborting the procedure Facial nerve displacement (Perkins, 2001) n n Facial nerve is compressed superiorly with No. 24 suction (5 second periods) 10 -15 sec delay between compressions Perkins describes laser stapedotomy while nerve is compressed Wire piston used n Add 0. 5 to 0. 75 mm to accommodate curve around the nerve
Floating Footplate n Footplate dislodges from the surrounding OW niche n n n Prevention n Incidental finding More commonly iatrogenic Laser Footplate control hole Management n n n Abort H. House favors promontory fenestration and total stapedectomy Perkins favors laser fenestration
Diffuse Obliterative Otosclerosis n n n Occurs when the footplate, annular ligament, and oval window niche are involved Closure of air-bone gap < 10 d. B less common. Refixation commonly occurs
Perilymphatic Gusher n n n Associated with patent cochlear aqueduct More common on the left Increased incidence with congenital stapes fixation Increases risk of SNHL Management n n n Rough up the footplate Rapid placement of the OW seal then the prosthesis HOB elevated, stool softeners, bed rest, avoid Valsalva, +/- lumbar drain
Round Window Closure n n 20%-50% of cases 1% completely closed n No effect on hearing unless 100% closed n Opening has a high rate of SNHL
SNHL n 1%-3% incidence of profound permanent SNHL n n Surgeon experience Extent of disease n n n Prior stapes surgery Temporary n n n Cochlear Serous labyrinthitis Reparative granuloma Permanent n n n Suppurative labyrinthitis Extensive drilling Basilar membrane breaks Vascular compromise Sudden drop in perilymph pressure
Reparative Granuloma n n n Granuloma formation around the prosthesis and incus 2 -3 weeks postop Initial good hearing results followed by an increase in the high frequency bone line thresholds Associated tinnitus and vertigo Exam – reddish discoloration of the posterior TM Treatment n n ME exploration Removal of granuloma Prognosis – return of hearing with early excision Associated with use of Gelfoam
Vertigo Most commonly short lived (2 -3 days) n More prolonged after stapedectomy compared to stapedotomy n n n Medialization of the prosthesis into the vestibule n n Due to serous labyrinthitis With or without perilymphatic fistula Reparative granuloma
Recurrent Conductive Hearing Loss n Slippage or displacement of the prosthesis n n Most common cause of failure Immediate n n n Technique Trauma Delayed n n n Slippage from incus narrowing or erosion Adherence to edge of OW niche Stapes re-fixation Progression of disease with re-obliteration of OW Malleus or incus ankylosis
Amplification n Excellent alternative Non-surgical candidates n Patients who do not desire surgery n n Patient satisfaction rate lower than that of successful surgery Canal occlusion effect n Amplification not used at night n
Medical n Sodium Fluoride 1923 - Escot suggested using calcium fluoride n 1965 – Shambaugh popularized its use n Mechanism n n Fluoride ion replaces hydroxyl group in bone forming fluorapatite n Resistant to resorption n Increases calcification of new bone n Causes maturation of active foci of otosclerosis
Medical n Sodium Fluoride n n Reduces tinnitus, reverses Schwartze’s sign, resolution of otospongiosis seen on CT OTC – Florical Dose – 20 -120 mg Indications n n n Non-surgical candidates Patients who do not want surgery Surgical candidates with + Schwartze’s sign n n Treat for 6 mo pre-op Postop if otospongiosis detected intra-op
Medical n Sodium fluoride n Hearing results n 50% stabilize n 30% improve Re-evaluate q 2 yrs with CT and for Schwartze’s sign to resolve n If fluoride are stopped – expect re-activation within 2 -3 years n
Medical n Bisphonates n n n Class of medications that inhibits bone resorption by inhibiting osteoclastic activity Dosing not standard Often supplement with Vitamin D and Calcium Studies conducted on otosclerosis patients with neurotologic symptoms report the majority of patients with subjective improvement or resolution. Future application of this treatment unclear, especially with new reports of bisphonate related osteonecrosis.
References n n n n n n n Bacon, Gorham. A Manual of Otology. . Lea Brothers & Co. New York, NY. 1898. Bacon, Gorham. A Brothers & Co. New York, NY. 1898. Banerjee A, Whyte A, Atlas. Superior canal dehiscence : : review of a new condition. Clinical Otolaryngology. 30, 9 -15. Banerjee A, Whyte A, Atlas. Superior canal dehiscence Otolaryngology. 30, 9 -15. Brooker KH, Tanyeri H. Etidronate for the Neurotologic Symptoms of Otosclerosis : : Preliminary Study. Ear, , Nose & & Throat Journal. June 1997 ; 76 Brooker KH, Tanyeri H. Symptoms of Otosclerosis Study. Ear (6) : p 371 -377. Causse JR et al. Sodium fluoride therapy. Am J Otol 1993; 14(5): 482 -490 Causse JR et al. Sodium fluoride therapy. Am Otol 1993; 14(5): 482 -490 Committee on Hearing and Equilibrium guidelines for the evaluation of results of treatment of conductive hearing loss. Otolaryngology – Head and Neck Surgery. 113 (3) pp. 186 -7. Glasscock II ME, et al. Twenty-five years of experience with stapedectomy. Laryngoscope 1995; 105: 899 -904 Glasscock II ME, et al. Twenty-five years of experience with stapedectomy. Laryngoscope House HP, Kwartler JA. Total stapedectomy. . Otologic Surgery, 2 nd ed. edited by Brackmann, Shelton, and Arriaga, W. B. Saunders 2001; 226 -234 House HP, Kwartler JA. Total Hough J. Partial stapedectomy. Ann Otol Rhinol Laryngol 1960; 69: 571 Hough J. Partial stapedectomy. Laryngol 1960; 69: 571 House J. Otosclerosis. Otolaryngol Clinics 1993; 26(3): 323 -502 Jerger J. Clinical experience with impedance Arch Otolaryngol 1970; 92: 311 Jerger J. Clinical experience with impedance audiometry. Arch Otolaryngol 1970; 92: 311 Lempert J. Improvement in hearing in cases of otosclerosis: A new, one stage surgical technique. Arch Otolaryngol 1938; 28: 42 -97 Lippy WH, Schuring AG. Treatment of the inadvertently mobilized footplate. Otolaryngol Head Neck Surg 1973; 98: 80 -81 Lippy WH, Schuring AG. Treatment of the inadvertently mobilized footplate. Surg 1973; 98: 80 -81 Meyer S. The effect of stapes surgery on high frequency hearing in patients with otosclerosis Am J Otol 1999; 20: 36 -40 Millman B. Giddings, NA and Cole, JM. Long-term follow-up stapedectomy in children and adolescents. Otol Head Neck Surg 1996; 115(1): 78 -81 Millman B. Giddings, NA and Cole, JM. Long-term follow-up stapedectomy Surg 1996; 115(1): 78 -81 Minor L. Clinical Manifestiations of Superior Semicircular Canal Dehiscence. The Laryngoscope. 2005. 115: 1717 -1727. Minor L. Clinical Manifestiations of Superior Semicircular Canal Dehiscence. Laryngoscope. 2005. 115: 1717 -1727. Muller, C. Gadre , A. Otosclerosis. Quinn’s online textbook of Otolaryngology. http: //www. utmb. edu/otoref/Grnds. Index. html. . Muller, C. Gadre, A. Nelson EG, Hinojosa R. Questioning the Relationship between Cochlear Otosclerosis and Sensorineural Hearing Loss: A Quantitative Evaluation of Cochlear Structures in Cases of Otosclerosis and Review of the Literature. The Laryngoscope. 2004; 114: 1214 -1230 Perkins RC. Laser stapedotomy. Otologic Surgery, 2 nd ed. edited by Brackmann, Shelton, and Arriaga, W. B Saunders 2001; 245 -260 Perkins RC. Laser stapedotomy for otosclerosis. Laryngoscope 1980; 91: 228 -241 Perkins RC. Laser stapedotomy for otosclerosis. Politzer. Primary Diseases of the Bony Labyrinthine Capsule. Archives of Otology, 1894, vol. xxiii. P. 255. Politzer. Primary Diseases of the Bony Labyrinthine Capsule. Archives Otology, 1894, vol. xxiii. P. 255. Roland PS. Otosclerosis. www. emedicine. com/ped/topic 1692. htm. 2002; 1 -11 Roland PS, Meyerhoff WL. Otosclerosis. Otolaryngology-Head and Neck Surgery. 3 rd ed. , edited by Byron J. Bailey, Lippincott Roland PS, Meyerhoff WL. Otosclerosis. Williams & Wilkins, Philadelphia 2001; 1829 -1841 Rosen S. Restoration of hearing in otosclerosis by mobilization of the fixed stapedial footplate. An analysis of results. Laryngoscope 1955; 65: 224 Rosen S. Restoration of hearing in otosclerosis by mobilization of the fixed stapedial footplate. An analysis of results. 269 Shea J Jr. Fenestration of the oval window. Ann Otol Rhinol Laryngol 1958; 67: 932 -951 Shambaugh G. Clinical diagnosis of cochlear (labyrinthine) otosclerosis. Laryngoscope 1965; 75: 1558 -1562 Shambaugh GE, Jr. and Glasscock ME, III. Surgery of the ear, 3 rd ed. Philadelphia, W. B. Saunders, 1980; 455 -516 Shambaugh GE, Jr. and Glasscock ME, III. Surgery of the ear Toynbee, Joseph. The Diseases of the Ear: Their Nature, Diagnosis, and Treatment. With a Supplement by James Hinton. London, 1868.