Odessa National Medical University Department of Normal and



 & soft (pulp) tissues Inflammatory")








 separates the primary dentin and")






 Atrophy of")





 fills the coronal defect.")





 Depends on duration: acute chronic with activation")

















.")




 -")

. A, Large, diffuse, and corrugated white lesions of the")
- Slides: 61
Odessa National Medical University Department of Normal and Pathological Clinical Anatomy Lecture on the topic: Diseases of the hard tissues of the tooth (caries, non-carious lesions), pulpitis, periodontitis, periostitis, osteomyelitis of the jaw bones.
Diseases of oral cavity Pathology of teeth Pathology of peri- & paraodontal tissues Pathology of salivary glands Pathology of lips, tongue & soft tissues of oral cavity
Structure of tooth Enamel - mineral substances 96 -97% Dentin-70% nonorganic; 30%- organic substeces Cementum (cellular & acelluar)-65% nonorganic; 23%- organic; 12% -water Pulp – loose connective tissue Periodontum-dens connective tissue
Pathology of tooth Pathology of hard (enamel, dentin, cementum) & soft (pulp) tissues Inflammatory (pulpitis, gingivitis) & noninflammatory (caries, fluorosis) Tumors - benign & malignant Malformation (of teeth or parts of tooth- enamel; dentin)
Caries is the progressive destruction, by bacteria and their products, of the teeth calcified tissues exposed to the oral environment. It is subdivided into: caries of enamel caries of dentine caries of cementum
Development of caries: The acid theory / at first demineralization, after organic matrix destruction happens. It explains development of caries on the sides of crown/. The proteolytic theory / at first organic matrix, demineralization develops after. This theory explains development of caries on the masticatory surfaces of teeth- no cuticle there/. The combined theory /asserts that both foregoing theories are correct /. Lactobacillus acidophilus & Streptococcus mutans
There are 4 stages depends on clinical morphological characteristics: the stage of spot, superficial caries, medium caries, deep caries. Duration of caries can be rapid and slow.
Stage of spot. A white opaque spot appears on the surface of enamel which looks as reminds a lime (chalky spot). A pathological process shows up dismineralization and demineralization of enamel in superficial layer. Superficial caries. Shows up a demineralization and enamel destruction within the limits of dentinal-enamel junction.
Middle caries. This stage destroys dentinalenamel junction, & progress into dentine. Extended dentinal canaliculi are filled by plenty of microorganisms. Deep caries. The large carious cavity appears in soften dentine. Between the bottom of carious cavity and pulp is rim of dentine only, or the carious it spreads to pulp.
Caries. Decalcification of enamel
Deep caries
Deep caries
Physiologic secondary dentin. A distinct line of demarcation (arrow) separates the primary dentin and physiologic secondary dentin. Reparative secondary dentin. Localized deposition of secondary dentin (bottom) at the pulpal end of the dentinal tubules affected by the carious process.
Features of caries in a child 1. Circular. /at this a defeat is localized in the area of neck of tooth. Such caries develops quickly/ 2. An early, subenamel caries /develops directly under the layer of enamel/. 3. A lateral caries /develops on the sides of tooth as well as circular caries, but duration of it more slow/.
4. A stationary /caries develops, as a rule, only in the first molar. A carious defeat is localized only in an enamel and does not make progress/. 5. Retrograde caries. /Development of carious defeat begins from the side of pulp. A dentine is damaged at first, then enamel. Such caries can develop at purulent pulpits, when a causative agent gets in pulp by hematogenic way, at traumas and anomalies of teeth development/.
Fluorosis A fluorosis is a disease which develops at prolonged &/or excessive incorporation of fluorine. Clinically it shows up injury of many organs, including teeth. A disease develops in endemic regions, where content of fluorine in water and food is >2 mg/l (norm 0. 7 -1. 2 mg/l). The process of formation and calcification of enamel is suffered.
4 degrees are distinguished: 1 degree is a very weak defeat. On the vestibular surfaces of teeth no more than 1/3 their areas are observed poorly expressed chalky spots and lines; 2 degree is a weak defeat. Typical defects occupy the about half of teeth crown surface. May be appeared pigmented spots, but localized in an enamel only;
3 degree is the mildly expressed defeat. More than on a half crown is placed by anastomosing spots; 4 degree is a heavy defeat. Unitary and multiple erosions appear on the surface of teeth. They can be with or without color (from yellowbrown to black) As a result of mineralization violation in hard tissues of tooth at 3 and 4 degrees of fluorous defeat teeth become fragile, easily destroyed.
Fluorosis
Reactive changes of pulp Hemo-, lymphodynamic desorders (thrombosis, hypo- hyperemia, edema, hemorrhage) Atrophy of pulp (decreased N of odontoblasts, pulpocytes, fibrosis) Necrosis of pulp Dystrophy of pulp (hydropic & lipid degeneration of odontoblasts; mucoid swelling, hyalinosis, amyloid bodies in stroma) Denticles ( free, pariatal, interstitial; high-or low developed) Intrapulpar cysts (solitary or multyple)
Pulpitis It is the most common and clinically significant lesion of the pulp. It occurs most often due to the extension of the carious process into dentine and then to the pulp. Pulpitis is classified into: Acute: 1. cerous, 2. purulent (incl. abscessis) Chronic: 1. gangrenous, 2. hypertrophic (hyperplasic, granulose), 3. fibrous. Cronic with exacerbation.
Pulpitis develops as the complication of caries, as ascending inflammation with hematogenic or lymphogenic spreading of infection through apical foramen, after trauma & may be: 1. diffuse or local 2. in the crown or root
Acute pulpitis
Chronic pulpitis
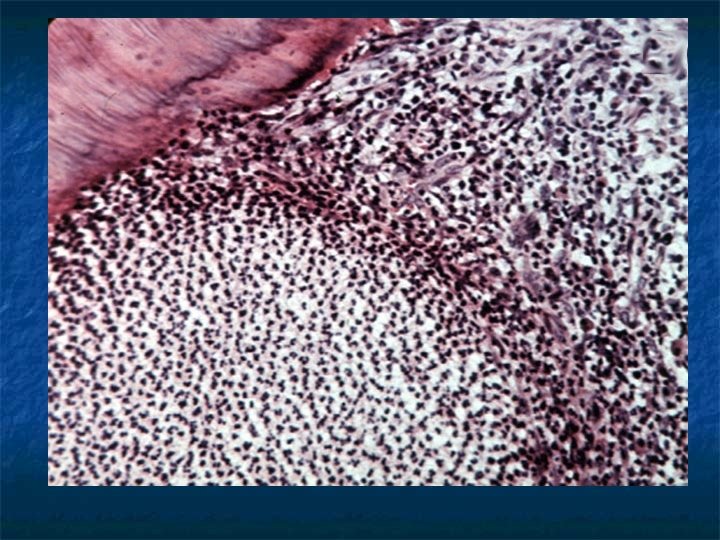
Chronic hyperplastic pulpitis
1 2 Chronic hyperplastic pulpitis. Chronically inflamed granulation tissue (2) fills the coronal defect. Note surface stratified squamous epithelium (1).
Reversible pulpitis. Dental pulp exhibiting hyperemia and edema.
Complications of chronic pulpitis: atrophy, sclerosis, hyalinisis, calcinosis, formation of denticle in the pulp; spreading of inflammation to the periodontal region and following development of periodontitis (most often), paradontitis, formation of periapical granulomas and cysts, generalization of bacterial inflammatory process – odontogenic sepsis.
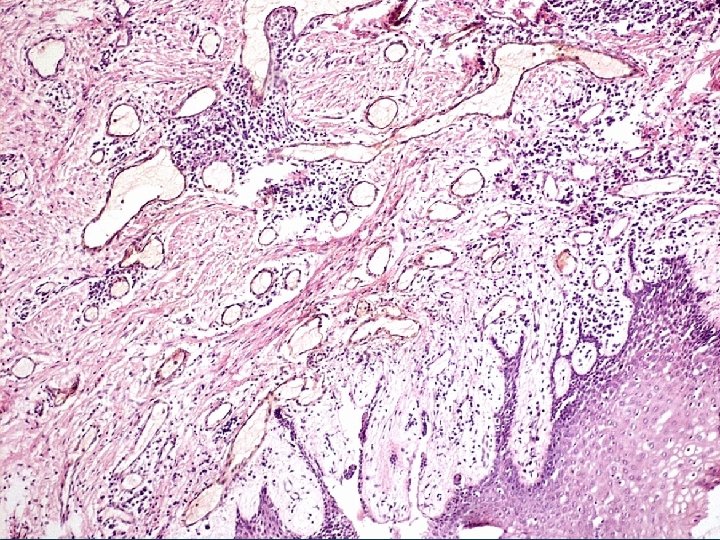
Pariapical granuloma
Periapical granuloma. Higher-power view. Granulation tissue exhibits mixed inflammatory infiltrate consisting of lymphocytes, plasma cells, and histiocytes.
Periodontal abscess. Dark-red and hemorrhagic enlargement of the interdental papilla between the maxillary right lateral incisor and cuspid.
Periodontitis Depends on localization: apical marginal (gingival) Depends on duration: acute chronic with activation
Acute apical periodontitis is subdivided into: serous & purulent. (from 2 -3 days up to 2 weeks with recover or chronic form development) Chronic apical periodontitis is subdivided into: granulating, granulomatous (simple, compound or epithelial granuloma, cystgranuloma), fibrous
granulating chronic apical periodontitis – is a process of granulation tissue formation near the apex of root. Histologically: high vascularized granulation tissue with lymphocytic, monocytic, plasma cells infiltration with intensive osteoclastic resorbtion of alveolar bone & cementum. In prograssion – smooth resorbtion develops (formation of lacunas without osteoclasts, following destruction of cortical bone, sprading of inflammation to surrounded soft tissues) After treatment: maturation of CT
granulomatous chronic periodontitis - simple granuloma is a round small pink-gray nodule connecting with fibrous connective tissue. It consists of granulation tissue, foam cells with cholesterol crystals, inflammatory infiltration. After treatment undergoes scaring. - compound or epithelial granuloma macroscopically looks like simple one. Microscopically: granulation tissue with wide epithelial cords. - cystgranuloma is a cavity lined with epithelium, granulation tissue & fibrous tissue around connecting it with apex of tooth.
Fibrous periodontitis is outcome of granulating one. Sometimes, traumas, presser of prostheses, high amount of dental stones lead to it. Microscopically: layers of fibrous tissue with mononuclear infiltrates, including foamy cells. Complications: Suppuration of granuloma, periostitis, osteomielitis. , sinusitis.
Diseases of gums, paradont gingivitis is an inflammation of gums’ mucous layer without destruction of dental-gingival junction. Local – mechanical trauma of gums, chemical & physical factors; Generalized - infectious, toxic-allergic, endocrine diseases.
There are next morphological types of gingivitis: Catarrhal Ulcerative- necrotic Hypertrophic Atrophic depends on duration: Acute Chronic.
Catarrhal gingivitis 1 - edema 2 - perivascular infiltration
Hypertrophic gingivitis 1 - cellular proliferation 1 – balloon dystrophy 2 - тgranulstion tissue 2 - akantosis 3 – lymphocytic, plasma 3 - parakeratosis & akantosis cell infiltration
Ulcerative gingivitis 1 – necrosis 2 – granulation tissue 3 – edema & cellular infiltration
Paradontitis, paradontosis Paradontitis is inflammation of paradontum with following paradontal, osseous destruction & dental-gingival pouches development. Subdivided into: 1) acute & chronic 2) Local & generalized. - Develops in 30 -40 years old persons. - Depends on deepness there are: mild (up 3, 5 mm), middle (up 5 mm), severe (more than 5 mm)
Etiology: local factors – abnormalities of teeth & soft tissues general factors – diabetes mellitus, reproductive system pathology, autoimmune pathology, neurological, gastrointestinal etc. Combination of factors & bacteria initiate inflammatory process (lysosomal enzymes, bioactive substances, phagocytosis) Morphology: disease starts from chronic catarrhal or hypertrophic gingivitis. Dystrophy→ necrosis → keratinization in epithelial layer
Mucoid swelling → fibrinoid change+vasculites in connective tissue. Resorbtion of cementum, alveolar bone with denudation of dental root happens, osteoporosis develops. Levels of alveolar bone destruction: I – up to ¼ of root high; II – up to 1/2; III – up to 2/3; IV –up to apex of root. In parallel there is new formation of bone & cementum develops – hypercementosis. Distrophy & Atrophy of pulp.
Paradontosis It is primary-dystrophic chronic disease of paradontum and forms 4 -5% from all diseases of it. Real couse of paradontosis is unknown. General clinical characteristics is retruction of gums without signs of gingivitis or periodontitis. Morphologically: there is a slow rebuilding of osseous trabecles showing zones of both osteoporosis and osteosclerosis, sclerosis and hyalinosis of vessels.
Epulis is term used for hyperplastic growths of granulation tissue as a result of chronic mechanical, inflammatory (or other agent) influence, sometimes arise in healing extraction sockets. It develops in 20 -40 years - old person (women offer). Macroscopical morphology: they are round or mushroom-shaped growth, 0, 5 -2, 0 cm in size on the fixed wide bottom. Epulis can be whitish, pale reddish, or brownish in color.
Microscopically these are: Angiomatous epulis looks as capillary hemangioma, contanes hemorrhagic areas and zones of hemosiderosis. Fibrous epulis looks as fibroma. Giant cell epulis (or giant cell granuloma) contains mature connective tissue with high amount of giant cells looking as multinucleated osteoclasts and small osteoblastic-like cells.
Peripheral giant cell granuloma (Epulis).
Peripheral giant cell granuloma. nodular proliferation of multinucleated giant cells in the gingiva
Pyogenic granuloma. Erythematous, hemorrhagic mass arising from the maxillary anterior gingiva. Ulcerated and lobulated mass on the dorsum of the tongue.
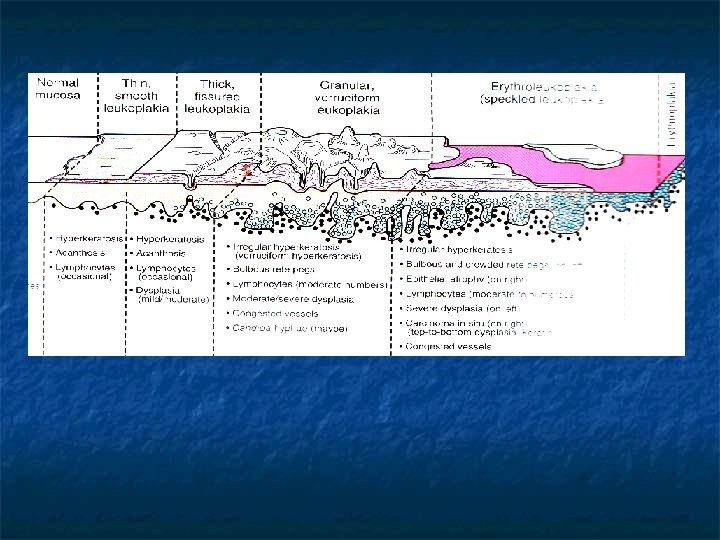
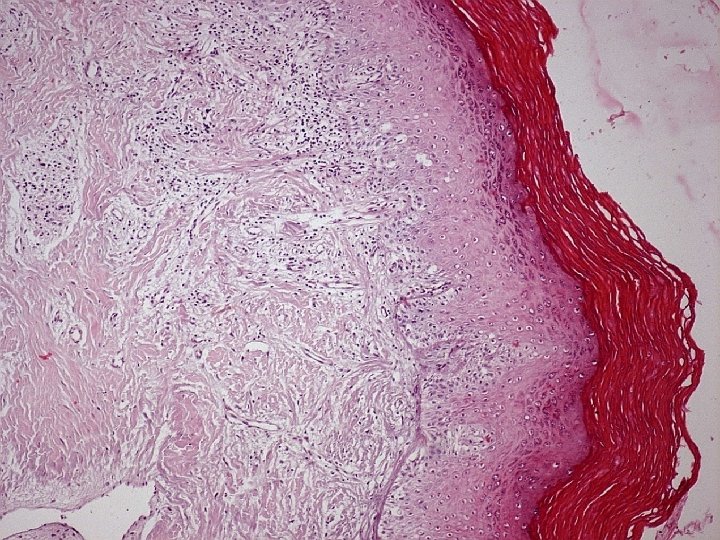
ORAL CAVITY PRETUMOR PROCESSES - Chronic inflammation - Leukoplakia (smooth, Granular & verruciform) - Erythroplakia
Granular leukoplakia. Irregular white patch in the floor of the mouth of a heavy smoker. Early invasive squamous cell carcinoma was found on biopsy. Verruciform leukoplakia. Exophytic papillary lesion of the anterior maxillary alveolar ridge. Biopsy revealed a welldifferentiated squamous cell carcinoma.
A Proliferative verrucous leukoplakia (PVL). A, Large, diffuse, and corrugated white lesions of the buccal mucosa and tongue. B, Same patient showing the extensive thickened and fissured alteration of the tongue. B