Norovirus Evonne Curran Nurse Consultant Health Protection Scotland














 The CE puts a letter")



")















- Slides: 42
Norovirus Evonne Curran Nurse Consultant Health Protection Scotland
In this presentation • Norovirus GI infection • Why it causes us problems • Results of a survey of norovirus experience 2009/10 • Plans for 2010/11 • Plans for after 2011
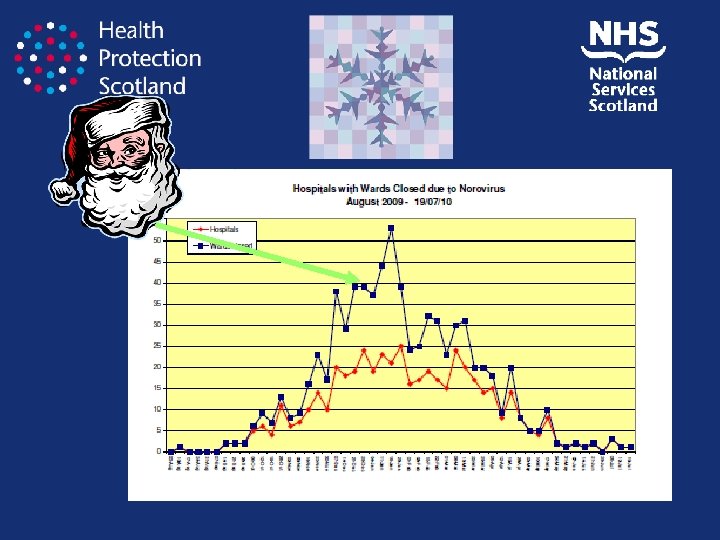
Why is norovirus such a problem in hospitals?
le b i s i v in al t n e onm ion r i v n e at n i m a cont Airborne dissemination SICPs not enough Odd presentations – is it a case? us o i t c nfe vp) i w o L 00 1 ( e Dos Voluminous diarrhoea & vomiting 50% attack rate No prodrom e Immunity short lasting Infectious before symptoms
Martin et al. Eurosurveillance 2004 Age sex distribution norovirus
‘The diarrhoea in norovirus infection is driven by both a leak flux and a secretory component. ’ Schulzke, et al GUT 2008
It’s not always mild and there is an associated mortality
• Nothing can be done • Nothing works • We just go through rituals • Should not bother • No one comes into hospital to get an infection • By being prepared we can reduce the impact of norovirus
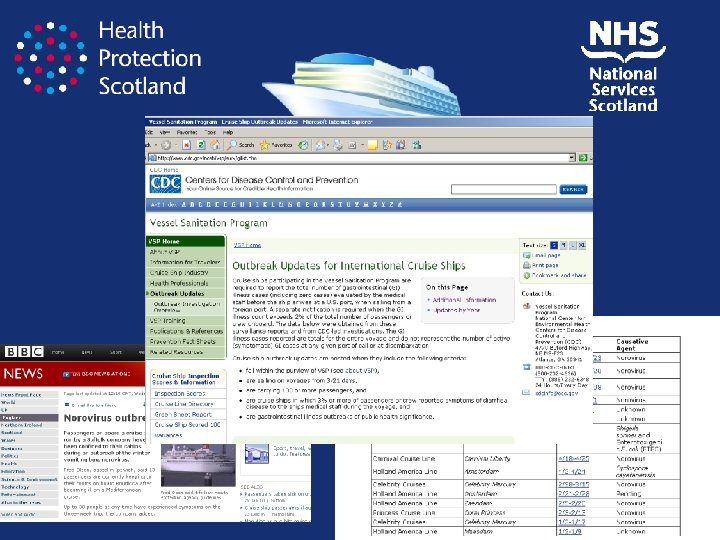
f o ro p e r Fi Reduction in outbreaks on cruises • Changing their ways of working – Surveillance (real time data) – Look for cases – Action when cases • Serve buffet, laundry services, isolation, cabin with window, hand hygiene facilities, check you are doing what you are supposed to be doing, remind people what to do, non buffet but restaurant.
g n i t igh F f e ir
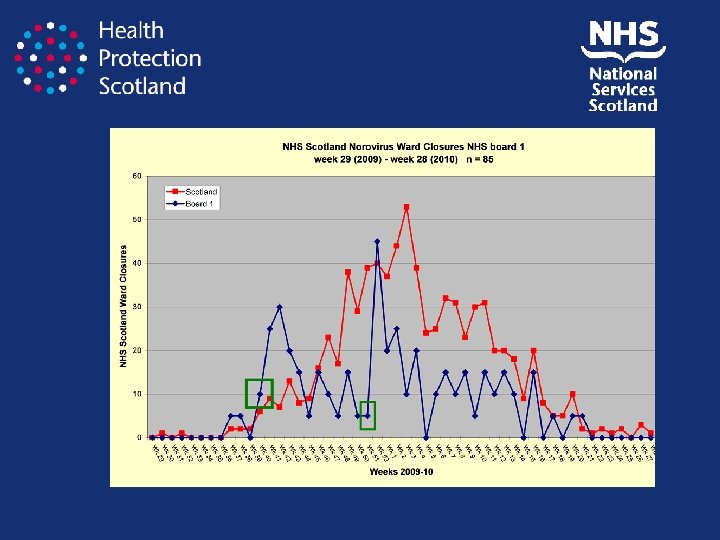
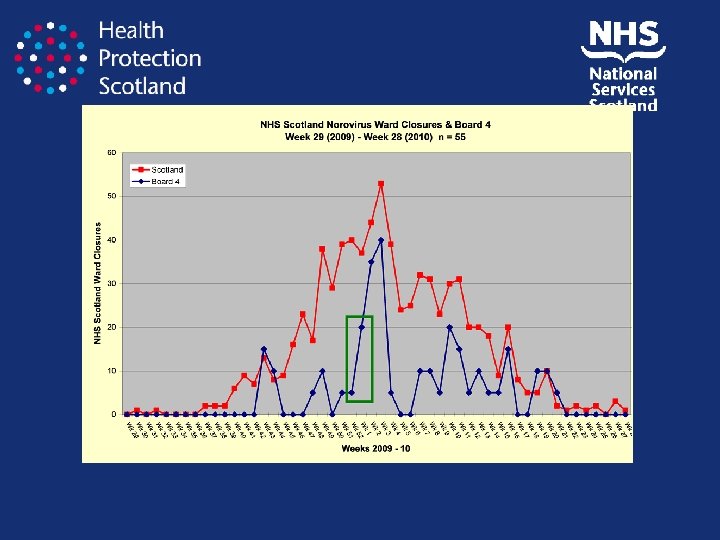
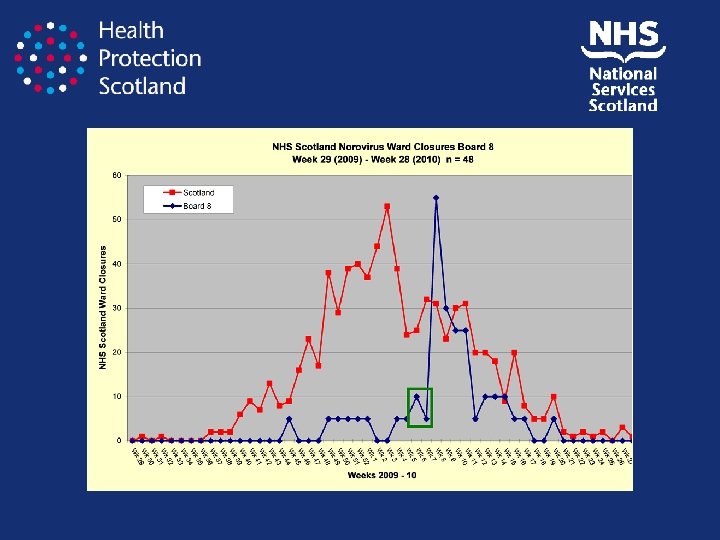
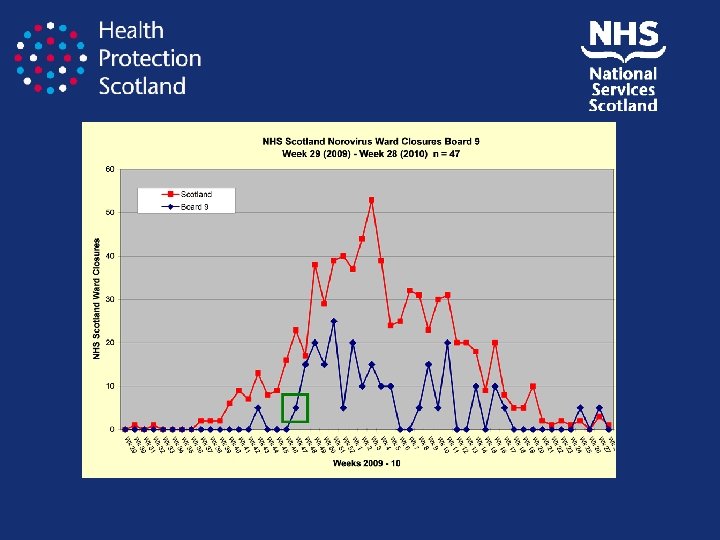
Norovirus season evaluation 2009/10 • How was it for you? Not so bad A pain: the worst ever
Key comments Lots of small fires starting at once When it came quickly Lots of relapses NB The ward reopening is not the point when its no longer a problem it’s the point when its manageable
The perfect norovirus storm • Increased referrals by out of hours GPs • Fewer coping services • Fewer experts to say ‘no’ • Weekends – no full ICN service
What we do • Let everyone know its started 5/11 • Let key HCWs know its started 6/11 • Keep everyone updated once its started 8/11
Good Practice Points • • • Run workshops (doctors) The CE puts a letter out Note in the pay slips Point prevalence data to bed management Whole hospital on alert once it starts Attend daily bed management
Do you remind staff to • Check referring GP if diarrhoea or diarrhoea in care home 4/11 • Provide GPs with advice managing noro in the community 6/11 • Require docs to ask about diarrhoea when taking a history 6/11 • Avoid unnecessary moves 11/0
Do you have • Policy to avoid unnecessary admissions 3/11 • Advice that patients with DV to isolation 11/0 • Advice to minimise CI in home 8/11 • A&E algorithm 5/5 • A&E procedure when Noro + MI 5/11 • Contingency plans 3/11
Do you think that recognising patients with possible norovirus symptoms as an infection risk is a problem in your hospitals ? • Yes 8/11 • Failure to recognise risk
Biggest problem when risk recognised • Insufficient isolation facilities • Competing priorities (A&E targets) • Isolation requirement not passed on
Recognition of outbreak • Early 9/11 established 2/11 • Transfer pre closure 3/11 never • Speed of closure – excellent ‘except at weekends’ • Ward staff are quick sometimes started precautions before I get there
‘How leaky is your bucket? ’
Are you able to continuously apply norovirus guidelines? • Yes 7 / 11
Other Key issues • No data on exactly when each outbreak occurs • Visitors
Lots of good testing ideas • Quarantined not closed • Management of paired wards • Norovirus diaries
Lets plug the holes in the bucket! • • Contingency planning Start date A&E algorithm Admission avoidance at weekends Nursing home admission avoidance Visitors RCA
Contingency planning Pre-start of season: • There is a plan for a norovirus outbreak includes who does what! • A contingency plan to reduce norovirus impact and the likelihood of norovirus outbreaks getting out of control (includes comms and single ward option) • Who at board level CPHM will help • Agreed norovirus activity locally: – Green: single wards in single hospitals – Amber: more than single wards in single hospitals – no pressure on routine services – Red: more than single wards closed – routine services being stopped – Black: One or more hospital closed due to multiple ward closures
Season has started nationally: • • • Confirm Norovirus contingency plan still valid Any changes needed to noro email groups Visit A&E / bed management – remind of algorithm inform of national situation Remind of how noro presents Remind what to ask / what to do Powerpoint for all new staff since last season Collective ID of the weakest links and mitigate Confirm / remind all wards of norovirus (e)folder of what to do Email who to contact for noro – at weekends or after 5 Get board public comms ready – Get top level co-operation Liaise with board re any N home outbreaks Weekend cover of ICN?
Ward X and Y are closed to due to norovirus. Visitor restrictions apply
Season has started locally: • • • Tell everyone – including the media Tell the visitors at the front door All meet and greet Daily meetings with bed-management Daily sit rep with local norovirus assessment Id how did the index case cause the outbreak – feedback • Assess all outbreaks for lessons learned • Share lessons learned locally and with HPS
Season over • Season debrief management and ICT – What worked well? – What could have worked better? – What will make it work better next time? – Share findings – Share with HPS
If we fail to prepare, we prepare to fail B Franklin
Norovirus will continue to be • A severe winter challenge to NHSScotland • Better preparation and execution of preparation plans will reduce its impact on ourselves and our services but more importantly….